Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
Fdl28(3).book(fdl029.fm)
Journal of Public Health | Vol. 28, No. 3, pp. 192–196 | doi:10.1093/pubmed/fdl029 | Advance Access Publication 29 June 2006
A survey of staff attitudes to smoking-related policy and intervention in psychiatric and general health care settings
Lisa McNally1, Adenekan Oyefeso1, Jan Annan2, Katherine Perryman1, Roger Bloor3, Steve Freeman3, Barbara Wain3, Hilary Andrews4, Martin Grimmer5, Arthur Crisp1, Deji Oyebode6, A. Hamid Ghodse2 1Department of Mental Health—Addictive Behaviour, St George’s, University of London, Cranmer Terrace, London SW17 0RE, UK 2International Centre for Drug Policy, St George’s, University of London, Cranmer Terrace, London SW17 0RE, UK 3Keele University Medical School, Academic Psychiatry Unit, Harplands Hospital, Stoke-on-Trent ST4 6TH, UK 4Suffolk Stop Smoking Service, The Ipswich Hospital NHS Trust, Heath Road, Ipswich IP4 5PD, UK 5The Ipswich Hospital NHS Trust, Heath Road, Ipswich IP4 5PD, UK 6South West London and St George’s Mental Health Trust, Springfield University Hospital, London SW17 7DJ, UK Address correspondence to A. Hamid Ghodse, E-mail: A B S T R A C T Background Although the move to smoke-free hospital settings is generally a popular initiative, it may be a more challenging and controversial
issue in mental health care. A survey was carried out to investigate differences in attitudes between clinical staff in psychiatric and general medical
settings to smoke-free policy and intervention. Method The sample comprised 2574 NHS staff working in two Acute Hospital Trusts and one Mental Health Trust in England. Attitudes were
examined on two factors: health care settings as smoke-free environments and the role of staff in stop smoking intervention. Results The findings indicated that attitudes on the two factors were only moderately correlated. Psychiatric staff expressed significantly less
favourable attitudes than general staff to smoke-free health care settings and also to the role of staff in stop smoking intervention. The largest
difference between the settings concerned the implementation of smoking bans. While approximately 1 in 10 staff in the general setting disagreed
with a smoking ban in their wards or clinics, nearly one in three psychiatric staff was against such a ban in their setting. Conclusions Staff attitudes need to be carefully considered, particularly in psychiatric settings, in attempts to implement smoke-free policies in Keywords smoke-free policy, smoking, staff survey, tobacco Introduction
support as a fundamental step towards achieving a smoke-free NHS and advises that, ‘training should be provided for
The question of whether smoking in public places should beprohibited is currently high on the agenda in many countries,including the UK. It is unsurprising, and maybe appropriate, thatamong those organizations leading the way towards a smoke-
Lisa McNally, Honorary Lecturer in Tobacco Addiction
free environment are health care settings such as hospitals and
Adenekan Oyefeso, Reader in Addiction Psychology
outpatient clinics. However, while the adoption of smoke-free
Jan Annan, Associate Director
policies in health care settings is a generally popular move,1 one
Katherine Perryman, Research Fellow Roger Bloor, Senior Lecturer in Addiction Psychiatry
area in which less favourable attitudes to smoke-free policy can
Steve Freeman, Researcher
be found is inpatient mental health care, which many see as
Barbara Wain, Researcher
appropriate for exemption to policies prohibiting smoking.2
Hilary Andrews, Co-ordinator
Policy changes are not the only relevant factor in creating
Martin Grimmer, Consultant Physician
smoke-free environments. The recent ‘Guidance for Smoke-
Arthur Crisp, Emeritus Professor of Psychiatry
free Hospital Trusts’ from the UK Health Development
Deji Oyebode, Medical Director
Agency identifies the widespread accessibility of stop-smoking
A. Hamid Ghodse, Director
The Author 2006, Published by Oxford University Press on behalf of Faculty of Public Health. All rights reserved.
ATTITUDES TO SMO KING-RELATED POLICY AND INTE RVENTION
all health professionals on how to give opportunistic stop-
Because smoking-related attitudes in an organization are
likely to be determined by a range of factors, including
Despite such clear messages, the effectiveness of smoking-
organizational policy and personal clinical experience, prin-
related policy and intervention would inevitably depend on
cipal component analyses were performed to examine the
the attitudes of health care staff to these initiatives. There
underlying factor structure of the questionnaire. Analyses of
is already some evidence that smoking-related attitudes differ
variance (ANOVAs) were carried out to investigate differ-
by professional groups.4 So far, however, no direct compari-
ences in attitudes across health care settings (i.e. psychiatric
sons have been made between staff attitudes in general and
versus general) while controlling for the influence of
Such comparative data would be of value in view of the
widespread perception that psychiatric settings are one of the
most difficult hospital settings within which to implementsmoking restrictions.5 This may be related to the unique
Sample characteristics and response rates
place occupied by smoking within the practice and culture of
Overall, the survey achieved a sample of 2574, comprising
psychiatric care. For example, smoking rooms are frequently
1737 general hospital staff and 837 psychiatric staff. The
the social hub of a mental health unit and smoking is often a
response rate was 51% overall, and higher in the general set-
major source of structure and activity to the patients’ day.6
ting (53%) than in the psychiatric setting (46%). The largest
Studies have also reported that mental health staff may often
professional group represented in the survey was that of
use cigarettes to appease or engage patients.7 Arguments for
nurses (including midwives and health care assistants) who
exempting mental health units from smoke-free policy also
made up 68% of the total sample. The next largest group was
often make reference to human rights and to the fact that
that of professionals allied to medicine (including physio-
many patients are resident in hospitals for extended periods
therapists, occupational therapists, social workers and psy-
chologists) who made up 17% of the sample. Medical
The study reported here compared attitudes to smoke-free
doctors (physicians, surgeons and psychiatrists) accounted
health care environments and to stop-smoking intervention
for 10% of the sample. A further 5% of the sample declined
between clinical staff in psychiatric and general NHS settings.
to indicate their professional group. The sample proportions
representing each of the professional groups were similarbetween the two settings. Concerning smoking status, 17%
of the sample were current smokers, with nearly a quarter of
The postal survey employed a cross-sectional design, with
questionnaires administered to staff across three NHSTrusts. Questionnaires were sent to clinical staff employed at
Internal reliability and data reduction
South West London and St Georges Mental Health Trust,
The questionnaire had a high level of internal reliability
University Hospital of North Staffordshire NHS Trust and
(Cronbach’s α = 0.84). The underlying factor structure of the
The Ipswich Hospital NHS Trust. Local research ethics
attitude questionnaire was examined to distinguish key
committee approval was obtained at all the three sites. The
themes related to the issue of smoking. Principal component
survey was confidential, and no attempt was made to identify
analysis was performed, with a subsequent Varimax rotation
staff through the information they provided.
on the data relating to the eight attitude items. The criterion
An eight-item questionnaire was administered to staff ask-
for extraction was an eigen value >1.
ing about opinions on issues relating to smoking. Answers
The analysis extracted two factors (see Table 1). Items 1, 2
were given on a 5-point Likert-type scale ranging from
and 3 reflected an ‘organizational’ (anti-smoking) orientation
‘strongly agree’ to ‘strongly disagree’ (items were reversed in
and explored views on health care settings as smoke-free
analyses so that a higher score indicated a more positive
environments. Alternatively, items 4, 5, 6, 7 and 8 tapped
attitude). Pilot work demonstrated that the questionnaire
into a ‘good practice’ orientation and reflected views on the
took 2–3 min to complete. Each questionnaire was distrib-
role of staff in stop-smoking intervention (including training
uted along with a return envelope addressed to the research
and delivery). The two factors were only moderately corre-
team. Staff were able to return their questionnaire by post, by
lated (r = 0.49), indicating that, while there was some shared
hand to a member of the project team or by email on request.
variance between them, they tapped into distinct issues. Table 1 Questionnaire items: rotated component matrix
2. Staff should not smoke in the presence of patients
3. Smoking should be banned in ward/clinic
5. Staff should be trained to offer advice and support
6. Hospitalization is a good opportunity for intervention
7. A qualification would be useful for me
8. A cessation programme would be useful in my ward/clinic
Fig. 1 Differences in attitudes between settings (n = 2509). All group
differences significant at P < 0.001. Fig. 2 Staff for, against and undecided in relation to smoking bans in
health care settings (n = 2544). ‘Organizational orientation’ factor: attitudes to health care settings as smoke-free environments
where between ‘undecided’ and ‘agree’; this score is less
The ‘organizational’ factor explored staff attitudes to health
favourable than the response to the organizational orientation
care settings as no-smoking environments. The mean score
factor. In the general setting sample, the mean score was 3.88
on this factor for the entire sample was 4.32 (95%CI = 4.29–
(95%CI = 3.85–3.92), whereas in the psychiatric sample, the
4.35), indicating an overall response somewhere between
mean attitude score was 3.71 (95%CI = 3.66–3.76) (Figure 2).
‘agree’ and ‘strongly agree’. In the general setting sample, the
ANOVA revealed that staff members working in the psychi-
mean response was 4.46 (95%CI = 4.42–4.49), whereas in
atric setting exhibited significantly less favourable attitudes
the psychiatric sample, the mean response was 4.04 (95%CI =
than general setting staff to stop-smoking intervention (mean
3.99–4.09) (Figure 1). One-way ANOVA revealed that staff
difference = 0.17, 95% CI = 0.11–0.23) (F1,2455 = 30.34, P <
members working in the psychiatric setting were significantly
0.001). This difference was less than that observed on the pre-
less favourable than general setting staff to smoke-free health
vious factor, and it should be noted that the large sample size
care settings (mean difference = 0.42, 95% CI = 0.36–0.47)
allowed for the detection of relatively small differences. How-
(F1,2516 = 195.50, P < 0.001). This effect remained significant
ever, group differences on this factor were again independent
after controlling for age, sex, smoking status and professional
of age, sex, smoking status and professional group. Attitudes to smoking bans in health care settings ‘Good practice orientation’ factor: attitudes to
Owing to the central position of smoking prohibition in
stop-smoking interventions in health care settings
recent NHS policy developments, staff views on the pro-
The ‘good practice’ factor explored attitudes to stop-smoking
posal that smoking should be banned in their ward or clinic
supportive interventions, including the role of staff in such
(item 3) were examined separately. Overall, the average rating
intervention and the value of training in intervention tech-
approximately corresponded to an ‘agree’ rating (mean =
niques. The mean score on this factor for the entire sample
4.11, 95%CI = 4.06–4.15). In the general setting sample,
was 3.83 (95%CI = 3.80–3.86), indicating a response some-
the mean response exceeded the ‘agree’ rating with a mean
ATTITUDES TO SMO KING-RELATED POLICY AND INTE RVENTION
of 4.33 (95%CI = 4.28–4.39), whereas in the psychiatric
towards smoke-free policies after the policy has been put in
sample, the mean attitude score was 3.64 (95%CI = 3.56–
place for some time. This shift in opinion may flow from the
3.72) (Figure 1). ANOVA revealed that psychiatric staff
fact that smoking bans have rarely been found to lead to
expressed significantly less positive attitudes than general
increased aggression and adverse incidents and, in fact, have
setting staff to smoking bans (mean difference = 0.69, 95%
even had a positive effect on ward functioning in many
CI = 0.60–0.79) (F1,2544 = 203.81, P < 0.001). This was
cases.8,9 However, despite claims that smoking occupies a
again independent of age, sex, smoking status and profes-
unique place within the culture of psychiatric care,6 this may
lead to smoke-free policies facing unpopularity in psychiatric
In relation to the item on smoking bans, respondents were
settings. There is currently no published data directly com-
divided into whether they were supportive of a smoking ban
paring attitudes to smoking policy and intervention among
(‘strongly agree’ or ‘agree’), against a smoking ban (‘strongly
staff in psychiatric settings with those of staff in general med-
disagree’ or ‘disagree’) or undecided. The proportion of staff
ical settings. This is because previous work on smoking ces-
indicating that they were against a smoking ban differed
sation in health care environments has either excluded
markedly between the groups, with only 10% of general set-
psychiatric settings or confined analyses to either general or
ting against a ban compared to nearly one-third (29%) of
What this study adds Attitudes by professional group
This survey is the first in the UK to provide direct compara-
ANOVAs were also used to examine differences in
tive data on smoking-related attitudes between staff in gen-
responses to the survey across professional groups. In rela-
eral and psychiatric settings. The implication of the findings
tion to staff attitudes to health care settings as no-smoking
is that the enactment of no-smoking policy, and the concur-
environments, doctors exhibited significantly more positive
rent provision of routine stop-smoking intervention, may
attitudes than nurses or professionals allied to medicine
well encounter more resistance from staff in psychiatric set-
(F1,2737 = 16.08, P < 0.001). Regarding attitudes to interven-
tings than in general settings. The study is salient in the light
tion, however, it was nurses who exhibited significantly more
of the recent stipulation from the UK Government that ‘by
positive attitudes than the other two groups, although the
the end of 2006. the NHS will be smoke-free’.11 Attitudes
group differences on this factor were of a lesser magnitude
to no-smoking policies and smoking cessation strategies
than in relation to no-smoking environments (F1,2576 = 6.29,
among the staff are likely to be crucial in achieving this aim,
P < 0.001). All professional group differences remained sig-
and the findings of the present study serve to reinforce the
nificant after controlling for age, sex and smoking status.
need for careful consultation and inclusion of staff in thedecision-making process. In particular, organizations may
Discussion
benefit from ensuring that policy changes are made withinthe context of a widespread system of staff-led smoking ces-
Main findings of this study
sation support, which, as the previous research suggests,
More favourable attitudes to smoke-free health care environ-
would be welcomed by staff as an opportunity to learn new
ments, smoking bans and stop-smoking intervention were
observed among clinical staff in general medical settingscompared with staff working in psychiatric settings. The larg-
Limitations of this study
est group difference in attitudes was observed in relation to
The response rate from staff to the survey was only moderate
smoking bans. While approximately 1 in 10 staff in the gen-
(51%), and questions may be raised as to whether the sample
eral setting disagreed with a smoking ban in their wards or
represents the full range of views held by health care staff.
clinics, nearly one in three psychiatric staff was against such a
However, it should be noted that the response rate is compa-
ban in their setting. In relation to professional group, doctors
rable to that achieved in most other UK surveys of clinicians’
exhibited the most favourable attitudes towards smoke-free
attitudes to smoking-related practice4,12,13 and also that the
health care environments, while nurses were the most posit-
sample size was large and represented all the main groups of
ive towards taking a role in smoking cessation intervention.
NHS staff having clinical contact with patients.
In addition, while a response bias was possible, it is was
What is already known on this topic
found that the emergent group differences were significant
Findings from literature reviews have demonstrated that staff
after controlling for age, sex and smoking status and are
in psychiatric settings develop a much more positive view
The present study did not examine attitudes to indoor and
Memorandum by Rethink (SP39) in House of Commons Health
outdoor smoking policies separately. It may well be that res-
Committee Smoking in Public Places First Report of Session 2005–06 Vol-ume II – Written Evidence. London: HMSO.
istance towards smoking bans in mental health settings maybe motivated by the fact that a policy covering grounds and
Health Development Agency. Guidance for Smoke-free Hospital Trusts. London: HDA, 2005.
buildings would in practice equate to an enforced abstinence
Dickens GL, Stubbs JH, Haw CM. Smoking and mental health
on patients unable to leave the grounds. This may be seen as
nurses: a survey of clinical staff in a psychiatric hospital. J Psychiatr
unrealistic as well as unethical. Alternatively, designated
Ment Health Nurs 2004;11:445–51.
outdoor smoking areas may lead to challenges and staff anxi-
Health Education Authority. Been there done that. Revisiting tobacco con-
ety towards the practicalities of how patients can be super-
trol policies in the NHS. London: HEA, 1999.
vised in these areas when available staff numbers are limited.
Brow n C . Tobacco and Mental Health: A Literature Review. Action on
Furthermore, research into the effects of allowing outdoor
smoking areas on attitudes to smoking policy may therefore
Mester R, Toren P, Ben-Moshe Y et al. Survey of smoking habits andattitudes of patients and staff in psychiatric hospitals. PsychopathologyAcknowledgements
1993;26:69–75.
el-Guebaly N, Cathcart J, Currie S et al. Public health and therapeutic
The research was funded by the Department of Health as
aspects of smoking bans in mental health and addiction settings. Psy-
part of a grant awarded to Professor Ghodse for the Reduc-
chiatr Serv 2002;53(12):1617–22.
tion in Tobacco Addiction programme. All researchers are
Lawn SJ and Pols RG. Smoking bans in psychiatric inpatient set-
independent of the funding body. Ethical approval was
tings? A review of the research. Aust N Z J Psychiatry 2005;39:874–93.
granted by the Local Research Ethics Committees at all three
10 Rigotti NA, Munafo MR, Murphy MFG et al. Interventions for
project sites—St Georges and South West London Mental
smoking cessation in hospitalised patients. The Cochrane Database of
Health NHS Trust, The Ipswich Hospital NHS Trust and
Systematic Reviews 2003;4.
North Staffordshire Combined Healthcare NHS Trust.
11 Department of Health. Choosing Health: Making Healthy Choices Easier.
12 Watt RG, McGlone P, Dykes J et al. Barriers limiting dentists’ active
References
involvement in smoking cessation. Oral Health Prev Dent 2004;2:95–102.
13 McEwen A, West R, Owen L. GP prescribing of nicotine replace-
1 MORI and Smoke-Free London (2003). Attitudes to Smoking in Public
ment and bupropion to aid smoking cessation in England and Wales. Addiction 2004;9:1470–4.
BRCA: Twenty Years of Advances Fifth International Symposium on Hereditary Breast and Ovarian Cancer April 23-25, 2014 Centre Mont-Royal, Montréal Wednesday, April 23, 2014 REGISTRATION & CONTINENTAL BREAKFAST . Foyer 4th Floor Welcome and Introduction to the Programme . Salon Mont-Royal Harley Eisman , MD, Co-Founder, Hereditary Breast and Ovarian Cancer Foundatio
Pharmakogenetik - patientenindividuell therapieren Information für Heilberufe Die Pharmakogenetik befasst sich mit dem Einfluss genetischer Variabilität auf die Arzneimittelwirkung. Als innovativer Teil der Pharmakologie gewinnt die noch am Anfang stehende Wissenschaft zunehmende Bedeutung am Arzneimittelmarkt, während bereits heute schon viele Forschungsarbeiten mit brauchbaren Erge
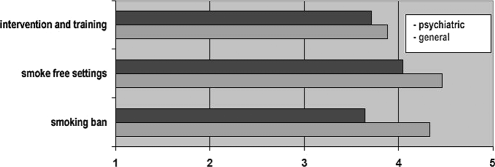
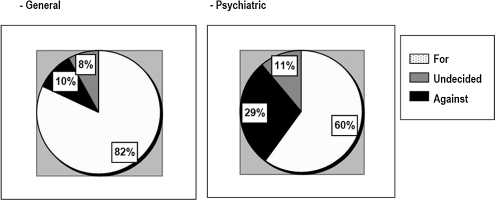 Table 1 Questionnaire items: rotated component matrix
Table 1 Questionnaire items: rotated component matrix