Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
272 1.9999
Journal of Thrombosis and Haemostasis, 1: 1398–1402
Cardiovascular pharmacogenetics in the SNP era
V . M O O S E R , D . M . W A T E R W O R T H , T . I S E N H O U R and L . M I D D L E T O NGenetics Research, GlaxoSmithKline, King of Prussia, Pennsylvania, USA
To cite this article: Mooser V, Waterworth DM, Isenhour T, Middleton L. Cardiovascular pharmacogenetics in the SNP era. J Thromb Haemost
across several haplotype blocks, thus potentially reducing the
Summary. In the past pharmacological agents have contribu-
number of SNPs for future whole-genome scans. Finally, a
ted to a significant reduction in age-adjusted incidence of
modest number of cases and controls appears to be sufficient to
cardiovascular events. However, not all patients treated with
detect genetic associations. There is little doubt that this type of
these agents respond favorably, and some individuals may
approach will have an impact on the way cardiovascular drugs
develop side-effects. With aging of the population and the
will be developed and prescribed in the future.
growing prevalence of cardiovascular risk factors worldwide,it is expected that the demand for cardiovascular drugs will
Keywords: cardiovascular disease, genes, pharmacogenetics,
increase in the future. Accordingly, there is a growing need to
identify the ‘good’ responders as well as the persons at risk fordeveloping adverse events. Evidence is accumulating to indi-
‘The right drug for the right patient’, a new
cate that responses to drugs are at least partly under genetic
control. As such, pharmacogenetics – the study of variability indrug responses attributed to hereditary factors in different
Age-adjusted cardiovascular mortality has markedly decreased
populations – may significantly assist in providing answers
in Western countries over the last few decades [1]. There is
toward meeting this challenge. Pharmacogenetics mostly relies
substantial evidence to indicate that this success is partly
on associations between a specific genetic marker like single
accounted for by the development of thrombolytic therapies
nucleotide polymorphisms (SNPs), either alone or arranged in a
and the prescription of antiplatelet and other agents in the
specific linear order on a certain chromosomal region (haplo-
secondary prevention of cardiovascular diseases, as well as
types), and a particular response to drugs. Numerous associa-
by a wider use of more effective pharmacological interventions
tions have been reported between selected genotypes and
to treat hypertension and dyslipidemia [2]. Despite these major
specific responses to cardiovascular drugs. Recently, for in-
accomplishments, cardiovascular diseases remain the major
stance, associations have been reported between specific alleles
cause of death in industrialized countries. This is due in part
of the apoE gene and the lipid-lowering response to statins, or
to the facts that cardiovascular risk factors remain highly
the lipid-elevating effect of isotretinoin. Thus far, these types of
prevalent, underdiagnosed and/or insufficiently treated [3];
studies have been mostly limited to a priori selected candidate
not all patients respond equally well to pharmacological inter-
genes due to restricted genotyping and analytical capacities.
ventions; and the population is aging. Moreover, there is ample
Thanks to the large number of SNPs now available in the public
evidence to indicate that, with the growing epidemics of obesity
domain through the SNP Consortium and the newly developed
[4,5] and Type 2 diabetes [6] progressively affecting Western
technologies (high throughput genotyping, bioinformatics soft-
countries, and the increasing prevalence of cardiovascular risk
ware), it is now possible to interrogate more than 200 000 SNPs
factors in developing countries [7,8], the incidence of cardio-
distributed over the entire human genome. One pharmacoge-
vascular diseases and the demand for safe and effective drugs to
netic study using this approach has been launched by Glaxo
prevent/treat these diseases will steadily increase worldwide.
SmithKline to identify the approximately 4% of patients who
Accordingly, there is a growing need for ways to better identify
are predisposed to developing a hypersensitivity reaction to
people who have the highest chance to benefit from pharma-
abacavir, an anti-HIV agent. Data collected thus far on the HLA
cological interventions, and those who have the lowest risk of
locus on chromosome 6 indicate that this approach is feasible.
developing side-effects when exposed to cardiovascular drugs.
Extended linkage disequilibrium can be detected readily, even
To date, only a fraction of people treated with a particular
drug fully benefit from such interventions. This is particularlyapparent in the case of antihypertensive therapies. It is esti-
Correspondence: Dr Vincent Mooser, Director Medical Genetics (Cardio-
vascular), Genetics Research, GlaxoSmithKline, 709 Swedeland Road, King
À50% of patients who receive one type of
therapy (for instance an ACE inhibitor or a calcium channel
Tel.: þ1 610 270 7732; e-mail: vincent.2.mooser@gsk.com
blocker) will have their blood pressure controlled by this
# 2003 International Society on Thrombosis and Haemostasis
treatment [9]. The remaining 50À75% will have received the
these two disciplines have their own characteristics. Tradition-
treatment, may experience side-effects, and yet their blood
ally, the goal of disease genetics is to identify genetic variants
pressure will not be normalized. This lack of consistency
associated with a particular susceptibility to developing a
[10] in terms of efficacy not only affects the individual patients,
disease. The genetic contribution to diseases and the way such
but also drug-producing companies. Indeed, many programmes
diseases are inherited can be estimated from twin and family-
have been terminated because the average response to one
based studies. Moreover, because genetically determined dis-
particular drug has been insufficient, yet a substantial propor-
eases can be evaluated in multiple members within families, it is
tion of patients may have adequately responded to this inter-
possible to perform family-based molecular genetic studies,
vention. Similarly, effective drugs have been removed from the
such as linkage analyses. Linkage studies have been shown to be
market because a fraction of patients have developed intolerable
very powerful in identifying the molecular basis of Mendelian
side-effects. It is obvious that a better way to identify the people
disorders (for instance Liddle’s syndrome, a rare form of salt-
who will adequately respond to the drug, and those who are
sensitive hypertension due to gain-of-function mutation within
prone to develop side-effects, would have a major impact on the
the epithelial sodium transporter in the proximal tubule of the
development and prescription of new cardiovascular drugs.
kidneys [18]). Most common diseases, however, are thought to
Evidence is accumulating to indicate that pharmacogenetics
be polygenic and multifactorial, due to interactions of environ-
may significantly assist in meeting the challenge of ‘the right
mental factors and a particular genetic make-up. As an example,
drug for the right patient’ [11,12].
it has recently been demonstrated that smoking is very prevalentin early onset (usually considered highly genetically deter-mined) forms of coronary artery disease [19]. This observation
further illustrates the need to include the environment as a factor
The way individuals respond to a particular drug – in terms of
in genetic studies on complex conditions.
both efficacy and side-effects – depends on a variety of para-
Pharmacogenetics can rarely rely on family-based studies,
meters, including compliance, bioavailability, drug–drug inter-
because usually only one family member is treated with a
actions, catabolization of the drug and its metabolites, the
particular drug. Accordingly, the heritability and the mode of
molecular mechanism responsible for the disease for which
inheritance of such responses are hard to predict, and family-
patients are treated, and what our ignorance prompts us to
based molecular genetic studies would be difficult to perform.
designate as ‘idiosyncratic reactions’. Because a variety of
At this stage pharmacogenetics is an experimental science that
genes encoding enzymes, transporters or receptors involved
mostly relies on association studies, i.e. studies comparing the
in drug absorption, metabolism, excretion and mode of action
distribution of sequence variants between cases who develop a
are polymorphic (with some of these polymorphisms being
particular response to the drug and appropriate controls who do
functionally active), a genetic predisposition is likely to account
not develop this type of response. The chance is that, in contrast
for part of the interindividual variability in response to drugs
to disease genetics, the environmental factor is limited (i.e. to
[13,14]. The example of slow acetylators who carry a particular
the drug), simplifying the analysis to some degree.
sequence variant within the N-acetyl-transferase 2 gene and
A recent study illustrates how pharmacogenetics may assist
thus poorly catabolize isoniazid or procainamide, illustrates
in exploring the genetic basis of a complex disease, in this
how one single gene variant can contribute to the occurrence of
particular case hypertriglyceridemia. In this study, the authors
severe side-effects, in this particular case hypersensitivity reac-
postulated that hypertriglyceridemia, which occasionally ac-
tions [15]. Another recent example of a particular response to
companies the administration of isotretinoin (a vitamin A
drugs that is mostly dependent on one single gene is provided by
derivative used to treat acne), occurs preferentially in indivi-
hyperbilirubinemia during administration of Tranilast. This
duals who have a predisposition to lipid disorders, and that
side-effect preferentially develops in carriers of one particular
elucidation of the genetic basis for this side-effect may assist in
variant of the UDG-glucuronosyltransferase 1 gene, the gene
our understanding of hyperlipidemia. The data showed that
responsible for Gilbert syndrome [16].
those individuals have a higher risk of developing metabolic
It is anticipated, however, that atypical drug responses are
syndrome (an aggregation of lipid disorders, hypertension and
rarely due to one gene only. For instance, it is generally accept-
glucose intolerance) than individuals for whom plasma trigly-
ed that African-Americans respond better to diuretics (and less
ceride levels remained unchanged during this therapy. As a
well to ACE inhibitors [17]) than Caucasians, due to a higher
proof of concept, it was shown that the lipid response to iso-
susceptibility to salt retention (and thus a lesser activated renin-
tretinoin was closely associated with the apoE E2 allele (which
angiotensin system), and that this susceptibility does not seem
is associated with Fredrickson Type III hyperlipoproteinemia)
to be dependent on one single gene. Elucidation of the genetic
and apoE E4 allele (which is associated with higher lipid levels
basis for this particular response to antihypertensive agents may
in the plasma than the wild-type apoE E3 allele) [20].
not only allow us to accurately predict who will most likely benefitfrom one particular type of drug, it would also significantly
Pharmacogenetics: the candidate–gene association studies
contribute to our understanding of the hypertensive disease.
This latter example illustrates how discoveries in pharmaco-
Thus far, restricted genotyping and analytical capacities have
genetics may impact on disease genetics, and vice versa, even if
limited pharmacogenetics to association studies of a priori
# 2003 International Society on Thrombosis and Haemostasis
Table 1 Pharmacogenetic studies: candidate-gene vs. whole-genome SNP association studies
selected candidate genes. In this approach, genes to be tested are
identify genes of susceptibility to a particular drug response
usually selected based on a previous understanding of the way
[16] (Table 1). One particular advantage of such an approach is
drugs are metabolized, or based on the biological pathway that
that, beyond finding tests to better predict the response to the
drug, this unbiased approach may reveal totally unexpected
A variety of conditions need to be met simultaneously for
genetic associations. As such, this type of pharmacogenetic
genetic associations to be detected, both for medical genetics
approach may yield major benefits to disease genetics, as
and pharmacogenetics. The example of apoE-associated lipid
response to isotretinoin may help illustrate this point. For such
The concept of whole-genome-based association studies is
an association to be detected, genetic variants obviously need to
relatively simple and takes advantage of the accumulating
be identified and accurately analyzed (using methods like
knowledge on SNPs. SNPs represent changes in nucleotides
restriction fragment length polymorphisms, allele-specific am-
that are present in a substantial proportion of the population.
plification or direct sequencing). These variants should by
Most SNPs are bi-allelic, making binary technologies applic-
themselves be functionally active (for instance by modifying
able to identify and analyze them. It is estimated that there is
the affinity of apoE to the LDL-receptor), or should be in
one SNP on average for every 1000 base pairs (hence the
linkage disequilibrium (see below) with other variants located
concept that humans share 99.9% of the genome in common),
in exons, in intron-exon junctions or regulatory sequences that
and that there are approximately 3 million SNPs in the human
are functionally active. In addition, the functional impact of
genome (which contains $3 billion base pairs). Accordingly,
these variants should not be fully compensated by other me-
the basic idea of a whole-genome SNP association study is to
chanisms (for instance by upregulation of the LDL-receptor)
compare the frequency of these variants between cases and
that would abolish the phenotypic expression of this particular
controls. To be successful, this type of approach relies on seve-
genotype. Moreover, the distribution of the variant should be
ral factors: the availability of SNPs in sufficient numbers to
sufficiently different in cases and controls, and the number of
cover the entire genome; very powerful and accurate genotyp-
cases and controls examined should be large enough (usually
ing capabilities to examine large collections of SNPs; appro-
several hundred individuals) for associations to be detected.
priate analytical approaches to detect significant associations;
Finally, appropriate environmental factors may need to be evalu-
and the availability of genomic DNA from large cohorts of well-
ated and included in the analysis to reveal genetic associations.
phenotyped cases and controls. Moreover, because analysis of 3
A large number of associations between predefined candi-
million SNPs for each case and control is not presently feasible,
date-genes and specific responses to drugs have been described
one must rely on the fact that several SNPs will provide the
so far [for reviews, see, among others refs 14, 15, 21 and 22]. In
same information as many SNPs in a particular region, due to
particular, associations have been reported between sequence
the phenomenon of linkage disequilibrium (Fig. 1).
variants within genes encoding metabolizing enzymes (like
The SNP Consortium (http://www.snp.cshl.org/), a joint
CYP2D6) and increased response to warfarin (and subsequent
academia–industry initiative, was commissioned to identify
risk of bleeding) or higher incidence of side-effects when
and release sequences of SNPs. The success of this initiative
exposed to b-blockers. Similarly, severe arrhythmias have been
has been tremendous, in the sense that the Consortium has re-
associated with sequence variants within genes encoding po-
cently made available in the public domain more than 2 million
tassium channels and exposure to antiarrhythmics. In the same
SNP sequences distributed over the entire human genome (for
way, the lipid-lowering effect of statins has been associated with
examples see http://www.ncbi.nlm.nih.gov/). The major ques-
specific alleles of the apoE or the CETP genes.
tions that now arise are (i) how to genotype these SNPs at areasonable cost, (ii) how many of these SNPs are needed toprovide adequate sensitivity and specificity for pharmacoge-
Pharmacogenetics: moving to whole-genome SNP
netic studies, and (iii) what is the required sample size.
At present, the only reliable way to answer these questions is
Rapid technological improvements in high-throughput geno-
to perform the experiments and generate experimental data.
typing, and developments in bioinformatics are now opening
GlaxoSmithKline has recently launched such an initiative. The
the way for an unprejudiced exploration of the entire genome to
goal of this project is to identify genetic variants that are
# 2003 International Society on Thrombosis and Haemostasis
Fig. 1. Schematic representation of the linkagedisequilibrium block structure of genomic DNA. Haplotype blocks and recombination hotspots areshown in green and red, respectively. Identification of recombination hotspots is basedon observed recombinations in the commonhaplotypes, shown as gaps or crossovers in thehaplotypes. Once this structure is known, SNPsthat contain all the mapping information can bechosen. Using this type of strategy, the numbersof informative SNPs is expected to be reduced to3–5 per haplotype block.
associated with hypersensitivity reaction to abacavir, an anti-
the genome is required to establish the degree of generality of
HIV agent [23]. Data accumulated thus far on the HLA locus on
chromosome 6 are very encouraging. They indicate that such an
Whatever the mechanism, the observation of haplotype blocks
experiment is feasible. Moreover, large regions of linkage
has clear implications for linkage disequilibrium mapping, be it
disequilibrium have been detected, forming haplotype blocks.
for whole SNP genome scans or for specific gene regions (Fig. 1).
These data are important, as they suggest that the number of
One advantage is that fewer SNPs will be required to map
SNPs to be examined can be reduced in other similar future
associations, as a relatively smaller number will be required to
initiatives (see below), and that cluster-analysis algorithms may
provide sufficient representative information within the blocks.
be developed and standardized to generate individual SNP
Furthermore we will know exactly where a greater saturation of
profiles (SNP Printssm) that define genetic-susceptibility re-
markers is required, in the regions of low linkage disequilibrium.
sponses to drugs. Finally, the data indicate that a modest number
However, the presence of large haplotype blocks will also limit
of cases and controls may be sufficient to achieve adequate
the resolution of association methods to fine-map a susceptibility
sensitivity and specificity [23,24].
gene, if it falls within one of these blocks, as additional markerswill not necessarily provide any more information.
Determining these haplotype blocks may therefore be pivotal
Linkage disequilibrium and haplotype blocks: potential
in the success of whole-genome association studies, and to this
end a major worldwide effort is underway to create a haplotype
Haplotypes are ancestral segments of chromosomes that have
map of the human genome, which is expected to be completed
been inherited as a unit throughout the generations with little
in 2–3 years. The question then arises, how different are the
genetic shuffling or mutation. They can be directly observed by
patterns of linkage disequilibrium among different ethnic
typing individuals within families for genetic markers and
groups, and will it be necessary to have separate maps for each
following the coinheritance of alleles from neighbouring mar-
group? A recent study found that Caucasian and Asian haplo-
kers through the generations. An alternative way to determine
types are very similar, but haplotypes of African origin are quite
haplotypes is to perform allele-specific sequencing, a technol-
different [27]. The authors estimate that approximately half the
ogy that is just starting to be utilized for that very purpose [25].
human genome exists in blocks of 44 kb or larger in Caucasian
Alleles that occur together in this fashion are said to show allelic
and Asian samples, and 22 kb or larger in African and African-
association, and ‘linkage disequilibrium’ is the extent of this co-
American individuals. Within each block 3–5 haplotypes typi-
cally capture about 90% of all chromosomes in each population.
It was originally thought that linkage disequilibrium would
They propose that to perform a fully powered association study
mostly reflect genetic distance and would decay in a fairly linear
will require as many as 300 000 SNPs in non-Africans and
manner over increasing distances. However, closer examination
1 million SNPs in Africans. Theoretically, this would suggest
of specific chromosomal regions has revealed instead irregular
that populations who have undergone population bottlenecks
linkage disequilibrium patterns that are mostly position depen-
and hence have more extensive linkage disequilibrium would be
dent. These patterns are composed of large stretches of DNA
more useful for initial localizations, and that populations with
($5–100 kb) where recombinations are not observed and link-
shorter range linkage disequilibrium would be more useful for
age disequilibrium is high (haplotype blocks), and short inter-
fine mapping. At this stage, it is still debated whether the
vening regions ($1–5 kb) where linkage disequilibrium is low.
optimal strategy will be that simple.
Jeffreys et al. showed that regions of linkage disequilibrium
A haplotype map of the human genome may therefore be
breakdown in the class II region of the major histocompatibility
critical in streamlining the process involved in association
complex correspond precisely with meiotic recombination hot-
mapping and may provide much information on the structures
spots observed by typing sperm [26], suggesting a possible
and histories of human populations. However, assuming that the
explanation for the position-dependent nature of linkage dis-
‘common variant–common disease’ theory is correct, it is
equilibrium breakdown. However, replication in other areas of
possible that rare variants will easily be missed with this
# 2003 International Society on Thrombosis and Haemostasis
strategy and more than one mutation in one disease gene will
changing demography and disease prevalence in the US. Diabetes Care
split the association signal, rendering it undetectable. Thus,
7 Yusuf S, Reddy S, Ounpuu S, Anand S. Global burden of cardiovascular
there is a great deal of speculation and projection at the current
diseases: Part II. Variations in cardiovascular disease by specific ethnic
time, which will only be resolved by the elucidation of some
groups and geographic regions and prevention strategies. Circulation
common disease or drug-response genes that will allow proof of
8 Reddy KS. Cardiovascular diseases in the developing countries: dimen-
sions, determinants, dynamics and directions for public health action. Public Health Nutr 2002; 5: 231–7.
Cardiovascular pharmacogenetics: hopes, hurdles and
9 Sever P. The heterogeneity of hypertension: why doesn’t every patient
respond to every antihypertensive drug? J Hum Hypertens 1995; 9(Suppl. 2): S33–S36.
The data accumulated thus far are very encouraging, and
10 Waeber B, Brunner HR. The multifactorial nature of hypertension: the
suggest that the concept of ‘the right drug for the right patient’
greatest challenge for its treatment? J Hypertens Suppl 2001; 19 (Suppl. 3): S9–16.
is becoming a closer reality. There are still major hurdles to
11 Marshall A. Getting the right drug into the right patient. Nat Biotechnol
overcome. Large clinical trials need to be performed (in various
ethnic groups) to consolidate the validity of this approach; such
12 Roses AD. Pharmacogenetics. Hum Mol Genet 2001; 10: 2261–7.
initiatives are underway in industry and academia (ex GenHat)
13 Evans WE, Relling MV. Pharmacogenomics: translating functional
[21], and the results of these experiments should be available
genomics into rational therapeutics. Science 1999; 286: 487–91.
14 Roden DM, George AL Jr. The genetic basis of variability in drug
within the next few years. Next, additional technological
responses. Nat Rev Drug Discov 2002; 1: 37–44.
improvements are necessary to bring the cost of genotyping
15 Meyer UA. Pharmacogenetics and adverse drug reactions. Lancet 2000;
down to a level that allows pharmacogenetics to become
economically attractive; here again, DNA chip technologies
16 Roses AD. Genome-based pharmacogenetics and the pharmaceutical
are presently being developed that should generate tests that are
industry. Nat Rev Drug Discov 2002; 1: 541–9.
17 Gibbs CR, Beevers DG, Lip GY. The management of hypertensive
affordable. In addition, regulators, payers, physicians and
disease in black patients. QJM 1999; 92: 187–92.
patients should agree with such projects. In this respect, phar-
18 Rossier BC, Pradervand S, Schild L, Hummler E. Epithelial sodium
macogenetics may raise ethical issues that are similar to the
channel and the control of sodium balance: interaction between genetic
ones raised by disease genetics. A major effort will be required
and environmental factors. Annu Rev Physiol 2002; 64: 877–97.
from the patients, their physicians, academia and industry to
19 Jomini V, Oppliger-Pasquali S, Wietlisbach V, Rodondi N, Jotterand V,
Paccaud F, Darioli R, Nicod P, Mooser V. Contribution of major
overcome these hurdles. In our opinion, the potential beneficial
cardiovascular risk factors to familial premature coronary artery dis-
impact of pharmacogenetics for the patients and society in
ease: the GENECARD project. J Am Coll Cardiol 2002; 40: 676–84.
20 Rodondi N, Darioli R, Ramelet AA, Hohl D, Lenain V, Perdrix J, Wiet-
lisbach V, Riesen WF, Walther T, Medinger L, Nicod P, Desvergne B,Mooser V. High risk for hyperlipidemia and the metabolic syndrome after
an episode of hypertriglyceridemia during 13-cis retinoic acid therapy foracne: a pharmacogenetic study. Ann Intern Med 2002; 136: 582–9.
The authors are employees of GlaxoSmithKline. They thank
21 Arnett DK, Boerwinkle E, Davis BR, Eckfeldt J, Ford CE, Black H.
Allen Roses, Virginia Schmith, Wayne Anderson and Sanjay
Pharmacogenetic approaches to hypertension therapy: design and
rationale for the Genetics of Hypertension Associated Treatment(GenHAT) study. Pharmacogenomics J 2002; 2: 309–17.
22 Ordovas JM, Mooser V. The APOE locus and the pharmacogenetics of
lipid response. Curr Opin Lipidol 2002; 13: 113–7.
23 Hetherington S, Hughes AR, Mosteller M, Shortino D, Baker KL, Spreen
1 Tunstall-Pedoe H, Vanuzzo D, Hobbs M, Mahonen M, Cepaitis Z,
W, Lai E, Davies K, Handley A, Dow DJ, Fling ME, Stocum M, Bowman
Kuulasmaa K, Keil U. Estimation of contribution of changes in coronary
C, Thurmond LM, Roses AD. Genetic variations in HLA-B region and
care to improving survival, event rates, and coronary heart disease
hypersensitivity reactions to abacavir. Lancet 2002; 359: 1121–2.
mortality across the WHO MONICA Project populations. Lancet 2000;
24 Lai E, Bowman C, Bansal A, Hughes A, Mosteller M, Roses AD.
Medical applications of haplotype-based SNP maps: learning to walk
2 Kuulasmaa K, Tunstall-Pedoe H, Dobson A, Fortmann S, Sans S, Tolonen
before we run. Nat Genet 2002; 32: 353.
H, Evans A, Ferrario M, Tuomilehto J. Estimation of contribution of
25 Patil N, Berno AJ, Hinds DA, Barrett WA, Doshi JM, Hacker CR,
changes in classic risk factors to trends in coronary-event rates across
Kautzer CR, Lee DH, Marjoribanks C, McDonough DP, Nguyen BT,
the WHO MONICA Project populations. Lancet 2000; 355: 675–87.
Norris MC, Sheehan JB, Shen N, Stern D, Stokowski RP, Thomas DJ,
3 Wong MD, Shapiro MF, Boscardin WJ, Shapiro MF, Boscardin WJ,
Trulson MO, Vyas KR, Frazer KA, Fodor SP, Cox DR. Blocks of limited
Ettner SL. Contribution of major diseases to disparities in mortality.
haplotype diversity revealed by high-resolution scanning of human
chromosome 21. Science 2001; 294: 1719–23.
4 Freedman DS, Khan LK, Serdula MK, Galuska DA, Dietz WH. Trends
26 Jeffreys AJ, Kauppi L, Neumann R. Intensely punctate meiotic recom-
and correlates of class 3 obesity in the United States from 1990 through
bination in the class II region of the major histocompatibility complex.
5 Flegal KM, Carroll MD, Ogden CL, Carroll MD, Ogden CL, Johnson
27 Gabriel SB, Schaffner SF, Nguyen H, Moore JM, Roy J, Blumenstiel B,
CL. Prevalence and trends in obesity among US adults, 1999–2000.
Higgins J, DeFelice M, Lochner A, Faggart M, Liu-Cordero SN, Rotimi
C, Adeyemo A, Cooper R, Ward R, Lander ES, Daly MJ, Altshuler D.
6 Boyle JP, Honeycutt AA, Narayan KM, Hoerger TJ, Geiss LS, Chen H,
The structure of haplotype blocks in the human genome. Science 2002;
Thompson TJ. Projection of diabetes burden through 2050: impact of
# 2003 International Society on Thrombosis and Haemostasis
Beacon Medical Practice Pre-Travel Questionnaire 1 It is essential that you visit our Travel Clinic well in advance of travelling abroad. Our Nurse will be able to advise you personallyregarding vaccinations, malaria prevention and general health issues you should consider for your destination. To help you have all the right information at hand, print off this form, complete the details, and ha
SHAKTI PRANA -CELEBRATE YOUR INNER FLOW mit HP Helen Levant & LSB Karin Roth Retreat 18.- 20. Oktober 2013 / Seminarhaus Die Lichtung IN WO Shakti ist das Sinnbild für schöpferische Kraft, göttliche Weiblichkeit und die Manifestation wahren Reichtums. Shakti Energie ist fein, verbunden mit Schönheit, Intuition und Weisheit. Der weibliche Körper unterliegt aus yogischer Sicht b
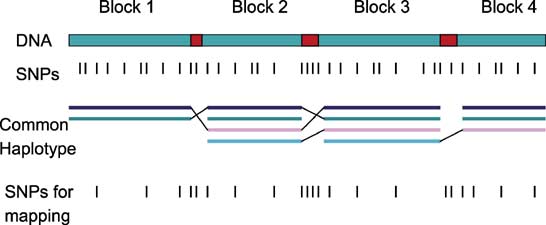 Fig. 1. Schematic representation of the linkagedisequilibrium block structure of genomic DNA.
Fig. 1. Schematic representation of the linkagedisequilibrium block structure of genomic DNA.