Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
Effect of craniosacral therapy on lower urinary tract signs and symptoms in multiple sclerosis
Complementary Therapies in Clinical Practice 15 (2009) 72–75
Complementary Therapies in Clinical Practice
Effect of craniosacral therapy on lower urinary tract signs and symptomsin multiple sclerosis
Gil Raviv ,,Shai Shefi , Dalia Nizani Anat Achiron
a Urology Department, Sheba Medical Center, Tel Hashomer, Affiliated to the Sackler School of medicine, Tel Aviv University, Israelb Multiple Sclerosis Center, Sheba Medical Center, Tel Hashomer, Affiliated to the Sackler School of medicine, Tel Aviv University, Israel
To examine whether craniosacral therapy improves lower urinary tract symptoms of multiple sclerosis
(MS) patients. A prospective cohort study. Out-patient clinic of multiple sclerosis center in a referral
medical center. Hands on craniosacral therapy (CST). Change in lower urinary tract symptoms, post
voiding residual volume and quality of life. Patients from our multiple sclerosis clinic were assessedbefore and after craniosacral therapy. Evaluation included neurological examination, disability statusdetermination, ultrasonographic post voiding residual volume estimation and questionnaires regardinglower urinary tract symptoms and quality of life. Twenty eight patients met eligibility criteria and wereincluded in this study. Comparison of post voiding residual volume, lower urinary tract symptomsand quality of life before and after craniosacral therapy revealed a significant improvement(0.001 > p > 0.0001). CST was found to be an effective means for treating lower urinary tract symptomsand improving quality of life in MS patients.
Ó 2008 Elsevier Ltd. All rights reserved.
urinary bladder sphincter in the form of detrusor sphincter dys-synergia (DSD) may be present in a subset of MS patients.
Lower urinary tract symptoms (LUTS), especially increased
In an attempt to ease the burden of LUTS in MS patients, several
urinary frequency and urgency are common complaints and a cause
pharmalogical and non-pharmalogical treatments have been
of impaired quality of life (QoL) in multiple sclerosis (MS) patients
Among the pharmacological available agents, several
with resultant significant physical and emotional stress upon
options are available for MS patients in order to decrease number
them.It has been shown that the correlation between subjective
and amplitude of involuntary bladder contractions and increase its
and objective measures of urinary function in MS patients is quite
storage capacity. These include the oral anticholinergic drugs oxy-
complex, further complicating follow-up, decision to treat and
butynin, tolterodine and trospium in varying doses, and the intra-
treatment evaluation.In the majority of MS patients LUTS have
been shown to stem from bladder dysfunction and can be classified
Recently, complementary medicine and unconventional thera-
to have an upper motor neuron etiology. The pathological process
pies have been shown to be effective for a wide range of medical
in MS consists of a demyelinating process most commonly
problems, including MS.Of those modalities, craniosacral therapy
involving the posterior and lateral columns of the cervical spinal
(CST) has been shown to be effective in treating several neurolog-
cord, and therefore voiding dysfunction is quite Addi-
ical conditions affecting the central nervous system
tionally, the loss of supraspinal control which stems from demye-
The craniosacral system is an integrated physiological system
linating insult to the brain leads to involuntary reflexive bladder
which consists of the membranes and cerebrospinal fluid that
contractions having specific urodynamic characteristics, and
surround and protect the brain and spinal cord, the bones to which
sometimes to neurogenic incontinence.Moreover, bladder are-
these membranes attach, and connective tissue elements ulti-
flexia or impaired coordination of the detrusor muscle and the
mately related to the membranes . The system extends from thebones of the skull, face and mouth which make up the craniumdown to the sacrum, or tailbone area. As with other human phys-iological systems, the craniosacral system may be either influenced
* Corresponding author. Urology Department, Sheba Medical Center, Tel
by or influences other systems, like the nervous, musculoskeletal,
Hashomer, Affiliated to the Sackler School of medicine, Tel Aviv University, Israel.
vascular, lymphatic, endocrine and respiratory systems. Early
Tel.: þ972 3 530 2231; fax: þ972 3 535 1892.
observations originating in the 1970’s have shown that the fluid
1744-3881/$ – see front matter Ó 2008 Elsevier Ltd. All rights reserved. doi:10.1016/j.ctcp.2008.12.006
G. Raviv et al. / Complementary Therapies in Clinical Practice 15 (2009) 72–75
within the dural membrane has a rhythmical and independent
motion, which persists throughout life. Craniosacral therapy isa gentle, hands-on technique which may be used to detect and
Each patient underwent four cycles of CST. All treatments were
correct imbalances in the craniosacral system that may be the cause
performed by a single dedicated member of our treatment and
of sensory, motor or neurological dysfunction. It takes advantage of
follow-up team at the MS ambulatory center (ND). This therapist
the fact that applying external force to specific bony elements of
was trained to perform general physical therapy as well as CST for
this system can be transmitted within We postulated that CST
MS patients. The treatment plan in this study consisted of a weekly
could be useful for treating LUTS in MS patients. Specifically, our
50 min session. Each session in turn consisted of the 10 step
aim in this study was to evaluate the effects of CST on various LUTS
protocol of CST as previously described by Upledger.Patients were
and on associated QoL in these patients.
treated while lying on their back, with the therapist applying verygentle pressure on specific key points.
Statistical analysis of results included paired t-test using Med-
This study was approved by the institutional review board.
Inclusion criteria were: (1) diagnosis of definitive MS; (2) LUTS
Data are presented as mean Æ SD. P < 0.05 was considered
duration of at least 3 months; (3) failure of past antimuscarinic
a statistically significant result.
treatment for LUTS; and (4) OAB-V8 questionnaire score !8 (seebelow). Exclusion criteria were: (1) antimuscarinic treatment
within the last 3 months; (2) indwelling or intermittent urinarycatheter; (3) post voiding residual volume (PVR) >200 cc; and (4)
One hundred consecutive MS patients followed at the Sheba
ultrasonographic evidence of upper urinary tract decompensation
Medical Center MS Center were assessed for participation in this
study. Twenty four MS females and four men met eligibility criteriaand were included in this study. Demographic and clinical char-acteristics are shown in Mean patient’s age was 51.5 Æ 12.6
(range 23–75) years. The mean duration of disease from diagnosiswas 9.1 Æ 7.1 (range 1–29) years. Urodynamic evaluation confirmed
Pre-treatment clinical evaluation included a complete neuro-
bladder hyperreflexia in all patients. In 16 (57%) detrusor sphincter
logical examination, Expanded Disability Status Scale (EDSS) score
dyssinergia was noted. Mean PVR decreased from 150.9 ml before
determination, ultrasonography of the kidneys and ureters to rule
CST to 66.1 ml after CST (p < 0.01, t-test). Both voiding frequency
out signs of upper urinary tract decompensation (hydronephrosis)
and urinary urgency episodes were significantly reduced from
with PVR estimation, assessment of urinary frequency and urgency,
5.1 Æ 0.9 and 5.4 Æ 1.1, respectively, before intervention, to 3.1 Æ 1.0
QoL estimation using a numeric 7-grade scale ) and
and 3.4 Æ 1.4, respectively after CST (p < 0.001 for both, t-test).
formal urodynamic study. The EDSS is a MS specific tool used to
Twenty two patients (79%) reported improved quality of life, while
quantify neurological disability. The EDSS consists of an eight-
six patients (21%) reported no change. Mean QoL score improved
functional-system scale including motor, sensory, cerebellar,
from 5.7 Æ 1.0 pre- to post-treatment 3.6 Æ 1.6 (p < 0.001, t-test)
brainstem, visual, mental, sphincteric, and other functions. The
(). No side effects of CST were observed, and compliance to
EDSS score ranges from 0 (normal examination) to 10 (death from
MS). A score of 6 indicates moderate disability requiring assistancewith walking a distance of 100 m.Post-treatment evaluation was
performed after completion of four cycles of CST and includedultrasonographic PVR estimation, assessment of urinary frequency
In addition to possible serious sequelae such as upper tract
and urgency, and QoL estimation. Urinary frequency and urgency
decompensation due to DSD, a significant proportion of MS
were evaluated separately using the same numeric 6-grade scale
patients suffer irritative LUTS like increased urinary frequency and /
in which 1 is defined as ‘‘not at all’’, 2 – ‘‘less than one time in
or urgency, which can adversely affect QoL.There are several
five’’, 3 – ‘‘less than half the cases’’, 4 – ‘‘approximately half thecases’’, 5 – ‘‘more than half the cases’’, 6 – ‘‘almost always or
always’’. Focused medical history with emphasis on disturbances of
Demographic and clinical characteristics of the study group (n ¼ 28).
the urinary system was obtained from the OAB-V8 self question-naire, followed by clinical interviews. The OAB-V8 was previously
described and validated for overactive bladder symptoms assess-ment.Briefly, eight questions are used to assess four aspects
of LUTS including frequency and urgency of urination, nocturia and
urinary incontinence. Each question is scored between 0 and 5, and
a cumulative score of ! 8 is considered to indicate an overactive
Ultrasonographic examination of the kidneys, ureters, bladder
and PVR estimation was performed with the Aloka SSD-500, using
EDSS: Expanded Disability Status Scale.
b PVR: post voiding residual volume.
a 3.5 MHz transducer. Urodynamic study was employed prior to
initiation of CST as a part of our routine evaluation of all MS patients
e See text for explanation of urinary frequency / urgency assessment.
G. Raviv et al. / Complementary Therapies in Clinical Practice 15 (2009) 72–75
Figure 1. Effect of CST on select parameters in MS patients. Left and right bars represent mean pre- and post-treatment results, respectively. 1: All paired t-test results for thecompared parameters were statistically significant: PVR – p < 0.01, Frequency – p < 0.001, Urgency – p < 0.001, QoL – p < 0.001.
pathophysiological mechanisms capable of causing neurological
bladder a crede maneuver or CIC are usually helpful. Recently, it
dysfunction related to the lower urinary tract in MS patients.
was suggested that non-pharmacological treatment alone or in
Autopsy studies in this population have revealed almost constant
combination with pharmacological treatment may be used to treat
evidence of demyelinative process in the cervical spinal cord, but
some of the functional disturbances of the urinary sy
involvement of the lumbar and sacral cord occurs in approximately
One of those treatment modalities is CST. The craniosacral
system consists of the membranes and cerebrospinal fluid that
Based on these findings, one would expect the characteristic
surrounds and protect the brain and spinal cord. In this study we
voiding dysfunction in MS to be detrusor hyperreflexia with some
showed that applying the therapeutic principles of CST was useful
degree of sphincter abnormality. Indeed, detrusor hyperreflexia
in alleviating LUTS associated with MS. The concept of the cranio-
was the most common urodynamic abnormality detected in
sacral physiological system was popularized in the early 1980s by
50–90% in various studies, while 30–65% of them had coexistent
Upledger and other pioneers following their observations and
However, it should be kept in mind that DSD can result in
investigations. They characterized it as a semi-closed hydraulic
elevated bladder pressures during micturation which leads to
system which envelopes the brain and spinal cord and bounded by
structural bladder damage, vesicoureteral reflux and subsequent to
the meninx. Inside this system is the cerebrospinal fluid (CSF),
renal damage and insufficiency. Therefore, management strategies
which shapes to some extent the meningeal borders of the system
in these patients should fulfill three main principles: adequate
deep to the cranial bones. These bones are used both as means for
urine drainage, low pressure urine storage and low pressure void-
evaluating and diagnosing patients and as handles in their treat-
ing. By achieving these objectives patients will achieve better
ment. Since the movement of the CSF is believed to be negligible, it
control on their urinary function and decrease risk of upper urinary
was postulated that applying pressure to a boundary of the
craniosacral system results in its transmission throughout this
Pharmacological treatment with the use of antimuscarinic
system. Hence, CST is a method of alternative medicine involving
agents has been used widely, especially for those with detrusor
a form of physical therapy. The therapist manually applies a subtle
hyperreflexia. However, in one hand, such treatment has potential
movement to the spine and cranial bones in order to assess and
unpleasant side effects like dry mouth, constipation and CNS irri-
cause a coordinated movement of the CSF.
tability that affects treatment compliance and prevents part of the
By gently working with the spine, the skull and its cranial
patients from achieving maximal efficacy due to sub-optimal
sutures, diaphragms, and fascia, the restrictions of nerve passages
medication dose. On the other hand, caregivers have to remember
are eased, the movement of CSF through the spinal cord can be
that such treatment can also impair bladder contractility and lead
optimized, and misaligned bones can be restored to their proper
to urinary retention especially in those patients with DSD. In cases
position. It is believed that the CSF has specific types of movement
where DSD and involuntary high pressure reflexive bladder
which can be adversely affected by pathological conditions causing
contractions are present, clean intermittent catheterizations (CIC)
neurological impairment like diseases and trauma.
is suggested with or without antimuscarinic drugs. In the minority
As was expected the urodynamic evaluation showed detrusor
of patients with difficulties of bladder emptying as a cause of atonic
hyperreflexia in all patients as well DSD at 57% of them. The
G. Raviv et al. / Complementary Therapies in Clinical Practice 15 (2009) 72–75
majority of those patients tried various type of treatments and part
of them had clear indication to start CIC. Therefore, the mostobjective parameter evaluated at the time of CST treatments was
1. Quarto G, Autorino R, Gallo A, De Sio M, D’Armiento M, Perdona` S, et al. Quality
of life in women with multiple sclerosis and overactive bladder syndrome. Int
the PVR. As the PVR decreased from 150.9 ml before CST to 66.1 ml
Urogynecol J Pelvic Floor Dysfunct 2007;18:189–94.
after CST (p ¼ 0.005, t-test) it seems that such treatment objectively
2. Kragt JJ, Hoogervorst EL, Uitdehaag BM, Polman CH. Relation between objective
succeeds. Both voiding frequency and urinary urgency episodes are
and subjective measures of bladder dysfunction in multiple sclerosis. Neurology2004;63:1716–8.
well known complaints in the majority of MS patients. Some of
3. Fingerman JS, Finkelstein LH. The overactive bladder in multiple sclerosis. J Am
those problems are well treated by antimuscarinic agents, but those
Osteopath Assoc 2000;100(3 Suppl):S9–12.
pills are with side effects and the new drugs are costly.
4. Lemack GE, Frohman EM, Zimmern PE, Hawker K, Ramnarayan P. Urodynamic
Based on our results it was found that such complaints were
distinctions between idiopathic detrusor overactivity and detrusor overactivitysecondary to multiple sclerosis. Urology 2006;67:960–4.
significantly reduced using our CST protocol (p < 0.0001 for both,
5. de Seze M, Ruffion A, Denys P, Joseph PA, Perrouin-Verbe B. International
t-test). As 79% of those patients who completed four cycles of CST
Francophone Neuro-Urological expert study group (GENULF). The neurogenic
reported improved quality of life and no patient reported a wors-
bladder in multiple sclerosis: review of the literature and proposal ofmanagement guidelines. Mult Scler 2007;13:915–28.
ening in quality of life following CST, it seems that such treatment
6. Ethans KD, Nance PW, Bard RJ, Casey AR, Schryvers OI. Efficacy and safety of
could be used in rehabilitation programs for MS patients. The
tolterodine in people with neurogenic detrusor overactivity. J Spinal Cord Med
significant portion of patients found to have an improvement of
7. Horstmann M, Schaefer T, Aguilar Y, Stenzl A, Sievert KD. Neurogenic bladder
treatment by doubling the recommended antimuscarinic dosage. Neurourol
Taking into account the known importance of QoL in chronic
conditions generally, and in MS specifically, it seems that this
8. Fader M, Glickman S, Haggar V, Barton R, Brooks R, Malone-Lee J. Intra-
vesical atropine compared to oral oxybutynin for neurogenic detrusor
therapy may be capable of alleviating part of the disease burden in
overactivity: a double-blind, randomized crossover trial. J Urol 2007;177:
9. Nayak S, Matheis RJ, Schoenberger NE, Shiflett SC. Use of unconventional
therapies by individuals with multiple sclerosis. Clin Rehabil 2003;17:
10. Upledger JE, Vredevoogd J. Craniosacral therapy. Seattle: Eastland Press; 1983. 11. Kurtzke JF. Rating neurologic impairment in multiple sclerosis: an expanded
Although the exact mechanism of action of CST still remains to
disability status scale (EDSS). Neurology 1983;33:1444–52.
be elucidated, this therapy proved to be both effective and safe in
12. Coyne KS, Zyczynski T, Margolis MK, Elinoff V, Roberts RG. Validation of an
treating LUTS of MS patients. Further studies are recommended.
overactive bladder awareness tool for use in primary care settings. Adv Ther2005;22:381–94.
13. Giannantoni A, Scivoletto G, Di Stasi SM, Grasso MG, Vespasiani G, Castellano V.
Urological dysfunctions and upper urinary tract involvement in multiple scle-rosis patients. Neurourol Urodyn 1998;17:89–98.
14. Blaivas JG, Kaplan SA. Urologic dysfunction in patients with multiple sclerosis.
In case you had to spend the rest of your life at your current
15. McGuire EJ, Savastano JA. Urodynamic findings and long-term outcome
management of patients with multiple sclerosis-induced lower urinary tract
urination status, what would have been your response?
dysfunction. J Urol 1984;132:713–5.
16. Alhasso AA, McKinlay J, Patrick K, Stewart L. Anticholinergic drugs versus non-
drug active therapies for overactive bladder syndrome in adults. CochraneDatabase Syst Rev
17. McClurg D, Ashe RG, Marshall K, Lowe-Strong AS. Comparison of pelvic floor
muscle training, electromyography biofeedback, and neuromuscular electrical
stimulation for bladder dysfunction in people with multiple sclerosis:
a randomized pilot study. Neurourol Urodyn 2006;25:337–48.
18. Yagci S, Kibar Y, Akay O, Kilic S, Erdemir F, Gok F, et al. The effect of biofeedback
treatment on voiding and urodynamic parameters in children with voiding
dysfunction. J Urol 2005;174:1994–7.
ORIGINAL CONTRIBUTION Intramuscular Ketorolac Versus Osteopathic Manipulative Treatment in the Management of Acute Neck Pain in the Emergency Department: A Randomized Clinical Trial Tamara M. McReynolds, DOBarry J. Sheridan, DO Ketorolac tromethamine injected intramuscularly (IM) In the ED, providing pain relief for patients with neck has been shown to be an effective analgesic in trea
LAW LIBRARY OF CONGRESS ARGENTINA HAGUE CONVENTION ON INTERNATIONAL CHILD ABDUCTION Introduction The Hague Convention on the Civil Aspects of International Child Abduction adopted on October25, 1980, during the 14th Session of the Hague Conference on Private International Law, was ratified byArgentina1 effective June 1, 1991. On May 31, 1998, pursuant to article 45 of the Convention,
 Complementary Therapies in Clinical Practice 15 (2009) 72–75
Complementary Therapies in Clinical Practice
Effect of craniosacral therapy on lower urinary tract signs and symptomsin multiple sclerosis
Gil Raviv ,,Shai Shefi , Dalia Nizani Anat Achiron
a Urology Department, Sheba Medical Center, Tel Hashomer, Affiliated to the Sackler School of medicine, Tel Aviv University, Israelb Multiple Sclerosis Center, Sheba Medical Center, Tel Hashomer, Affiliated to the Sackler School of medicine, Tel Aviv University, Israel
To examine whether craniosacral therapy improves lower urinary tract symptoms of multiple sclerosis
(MS) patients. A prospective cohort study. Out-patient clinic of multiple sclerosis center in a referral
medical center. Hands on craniosacral therapy (CST). Change in lower urinary tract symptoms, post
voiding residual volume and quality of life. Patients from our multiple sclerosis clinic were assessedbefore and after craniosacral therapy. Evaluation included neurological examination, disability statusdetermination, ultrasonographic post voiding residual volume estimation and questionnaires regardinglower urinary tract symptoms and quality of life. Twenty eight patients met eligibility criteria and wereincluded in this study. Comparison of post voiding residual volume, lower urinary tract symptomsand quality of life before and after craniosacral therapy revealed a significant improvement(0.001 > p > 0.0001). CST was found to be an effective means for treating lower urinary tract symptomsand improving quality of life in MS patients.
Complementary Therapies in Clinical Practice 15 (2009) 72–75
Complementary Therapies in Clinical Practice
Effect of craniosacral therapy on lower urinary tract signs and symptomsin multiple sclerosis
Gil Raviv ,,Shai Shefi , Dalia Nizani Anat Achiron
a Urology Department, Sheba Medical Center, Tel Hashomer, Affiliated to the Sackler School of medicine, Tel Aviv University, Israelb Multiple Sclerosis Center, Sheba Medical Center, Tel Hashomer, Affiliated to the Sackler School of medicine, Tel Aviv University, Israel
To examine whether craniosacral therapy improves lower urinary tract symptoms of multiple sclerosis
(MS) patients. A prospective cohort study. Out-patient clinic of multiple sclerosis center in a referral
medical center. Hands on craniosacral therapy (CST). Change in lower urinary tract symptoms, post
voiding residual volume and quality of life. Patients from our multiple sclerosis clinic were assessedbefore and after craniosacral therapy. Evaluation included neurological examination, disability statusdetermination, ultrasonographic post voiding residual volume estimation and questionnaires regardinglower urinary tract symptoms and quality of life. Twenty eight patients met eligibility criteria and wereincluded in this study. Comparison of post voiding residual volume, lower urinary tract symptomsand quality of life before and after craniosacral therapy revealed a significant improvement(0.001 > p > 0.0001). CST was found to be an effective means for treating lower urinary tract symptomsand improving quality of life in MS patients.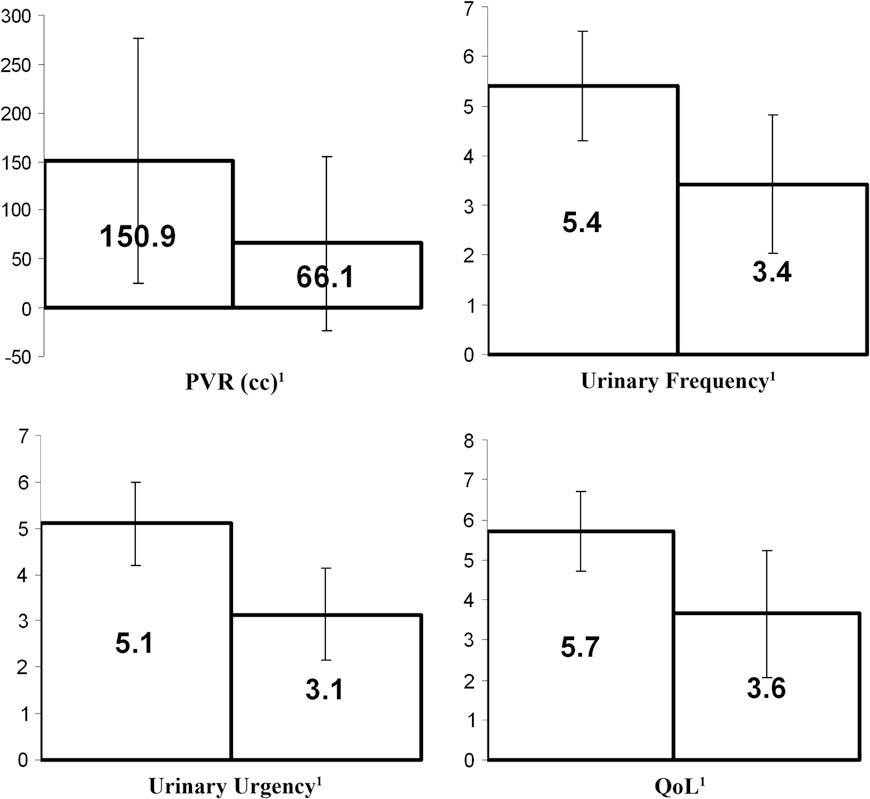 G. Raviv et al. / Complementary Therapies in Clinical Practice 15 (2009) 72–75
Figure 1. Effect of CST on select parameters in MS patients. Left and right bars represent mean pre- and post-treatment results, respectively. 1: All paired t-test results for thecompared parameters were statistically significant: PVR – p < 0.01, Frequency – p < 0.001, Urgency – p < 0.001, QoL – p < 0.001.
G. Raviv et al. / Complementary Therapies in Clinical Practice 15 (2009) 72–75
Figure 1. Effect of CST on select parameters in MS patients. Left and right bars represent mean pre- and post-treatment results, respectively. 1: All paired t-test results for thecompared parameters were statistically significant: PVR – p < 0.01, Frequency – p < 0.001, Urgency – p < 0.001, QoL – p < 0.001.