Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
Chirurgiewien.at
Cystic neoplasms of the pancreas: conservativeor operative treatment?
B. Akan, K. Sahora, H. Puhalla, M. Gnant, R. Jakesz, P. Götzinger
Division of General Surgery, Department of Surgery, Medical University of Vienna, Vienna, Austria
Received November 17, 2007; accepted after revision July 15, 2008
Zystische Tumore des Pankreas: Konservative oder
of diagnosis. 33 (78%) underwent operative treatment,
whereas 10 (22%) were treated conservatively. Malignancywas found in nine (27%) operated patients. Seven patients
Zusammenfassung. Grundlagen: Die modernen bildge-
(78%) with malignant cystic neoplasm and 15 patients
benden Verfahren haben zu einem Anstieg der Inzidenz
(63%) with a benign cystic neoplasm had symptoms.
der prima¨r zystischen Pankreastumore gefu
Median cyst size was 3.5 cm (1.5–12). There was one case
die chirurgische Behandlung obligat. Nach Art und Gro¨ße
of malignancy within cystic lesion smaller than 3 cm.
des Tumors kann jedoch auch ein konservativer Ansatz
Conclusions: Therapy can be tailored depending on
size and character of the pancreatic cyst. Surgical treat-
Ergebnisse: Von 43 zystischen Neoplasmen wur-
Keywords: Pancreas, intraductal papillary mucinous
den 11 (33 %) zufa¨llig entdeckt, 22 (77 %) Patienten hatten
neoplasm, serous cystic neoplasms, mucinous cystic neo-
Symptome zum Zeitpunkt der Diagnose. 33 (78 %) Pat-
ienten wurden operativ, 10 (22 %) Patienten jedoch kon-servativ behandelt. Bei neun (27 %) Patienten wurdeMalignita¨t festgestellt. Sieben (78 %) mit malignen und
15 (63 %) mit benignen Pankreastumor hatten Symptome.
Cystic pancreatic neoplasms are diagnosed in 0.7% of
Die mediane Zystengro¨ße lag bei 3,5 cm (1,5–12).
patients among 24,000 CT or MRI scans [1] and represent
Schlussfolgerungen: Die Therapie kann, nach Gro¨ße
less than 10% of pancreatic neoplasms [2]. Non-neoplas-
und Charakter der Pankreaszyste, adaptiert werden.
tic, inflammatory cysts found in patients with a history of
Die chirurgische Behandlung allein ist nicht mehr die
pancreatitis represent the vast majority of cystic lesion of
einzige Behandlungsmo¨glichkeit der prima¨r zystischen
the pancreas, originate on necrosis and have no malig-
¨sselwo¨rter: Pankreas, IPMN, SCN, MCN, zystische
The most common neoplastic type of cyst, the mu-
cinous cystic neoplasm (MCN) represented 44–49% [3, 4]. MCNs occur typically in middle-aged women and are usu-
Summary. Background: Owing to modern imaging tech-
ally located in the body or the tail region. Often the diam-
niques, the incidence of primary cystic neoplasms of the
eter exceeds 5 cm at the time of diagnosis, containing
pancreas is increasing. During the past decades all pan-
areas of malignant transformation in 10% of all patients.
creatic cysts were treated operatively. Depending on type
Typical cystic architecture is built of large multi-locular
and size a more conservative approach can be advocated.
cysts, with extensive mucin production without any com-
Method: Review of the literature and presentation of
munication to the pancreatic duct. They can be charac-
terized benign, borderline or malignant. The prognosis of
Results: From 43 patients, 11 (33%) were discovered
patients with resected mucinous cystadenocarcinoma is
incidentally and 22 (77%) had symptoms at the time
slightly better than patients with ductal adenocarcinoma,with 5-year survival of approximately 50% [3–8].
The second most common primary cystic neoplasm
Correspondence: Klaus Sahora, M.D., Division of General Surgery,
of the pancreas is serous cystadenoma (SCA), represent-
Department of Surgery, Medical University of Vienna, Waehringer-
ing 30% [3, 4]. SCAs are predominantly located in the
guertel 18-20, 1090 Vienna, Austria.
head of the gland and also mostly diagnosed in middle
Fax: þþ43-1-40400 5641E-mail: klaus.sahora@meduniwien.ac.at
aged women (35 vs. 65%) They are built of multiple smal-
220 5/2008 Cystic neoplasms of the pancreas: conservative or operative treatment?
ler cysts of different diameter, presenting a tumorous
Medical University of Vienna, Department of Surgery,
mass often greater than 7 cm when they are discovered.
were recorded within a database designed for this pur-
A typical radiomorphologic finding is a star-like shaped
pose. Patient information was anonymized and recorded
scar in the center of whole cyst. The cystic fluid does not
according to law and IRB regulations. The clinicopatho-
contain mucin. They are classified as benign even if there
logic findings during hospital stay were analyzed. Follow-
are some reports on very rare cases of serous cystad-
up of these patients was performed by telephone and=or
enocarcinoma [3, 6, 7, 9]. In most cases, symptoms are
query of the systematic Statistic Austria Database on
depending from size of the cystic neoplasm and lesions
patient’s date of death, executed annually by institution,
larger than 4 cm tend to cause symptoms [9].
thus providing follow-up data on 100% of patients.
The intraductal papillary mucinous neoplasm
Patients who presented only once at time of diagnosis
(IPMN) represents 20–25% of all cystic neoplasms. IPMN
are not listed in the database. Patient data were collected
is more frequently seen in the head of the pancreas and
at the outpatient clinic inspection and retrospectively
can be of benign, borderline or malignant character [3, 6].
with the assistance of the ‘‘clinical information system’’
Unlike other cystic neoplasms, it occurs more often in
of the hospital, providing an archive of all patient-specific
men than in women (55 vs. 45%). The pancreatic head
reports, leading to completeness of data. Surgery reports,
is the area of predominance. The cystic tumor is formed
discharge letters, histology reports and chemotherapy
by papillary formations rising from the ductal epithelium
treatment records were evaluated for every single patient.
and always communicates with the main or branch duct
All results of the patients are reported in median (range)
of the pancreas. Cystic fluid contains mucin, and is held
back because of duct occlusion. IPMNs are potentiallymalignant and are classified like MCN in benign, border-line or malignant. At the time of diagnosis, an invasive
carcinoma is found in about 40% of patients. Five-yearsurvival after the resection of malignant IPMN is 45%.
Between 1997 and 2007, 43 patients were diagnosed with
Solid and cystic papillary neoplasms also called
primary cystic lesions of the pancreas. The mean age was
Franz- or Hamoudi-tumors occur primarily in women of
68 years (24–82) and there were 32 (74%) female and 11
all age. They are seen in all regions of the pancreas and
(26%) male patients included. Forty seven per cent of
consist of solid, cystic and papillary components. Most of
cystic neoplasms were discovered incidentally and 53%
the patients are cured even after resection, vascular inva-
due to symptoms. The radiographic method most com-
sion and metastases have been reported.
monly used was CT (n ¼ 29, 67%) and MRI (n ¼ 13, 30%).
Within the majority of patients, cystic neoplasms of
The average cyst diameter was 3 cm (0.5–12). Thirty three
the pancreas are not symptomatic and are often inciden-
out of 43 patients underwent surgical resection at our
tal findings [1–3]. The standard diagnostic methods to
institution and 10 were treated conservatively.
distinguish between benign and malignant cysts are mul-tislice computed tomography (CT) and magnetic reso-nance images (MRI) [3]. There is no reported difference
in the superiority of neither CT nor MRI. MRI tends to be
Patient and cyst characteristics are summarized in
more sensitive in smaller lesions (<2 cm) and offer the
Table 1. The median age of nine male (27%) and 24 fe-
opportunity of non-invasive cholangiopancreaticography.
male patients (73%) was 65 years (24–85). Five (15%)
Endosonography may offer additional information after
patients had a positive family anamnesis of neoplasms,
inconclusive CT or MRI scan. There is low evidence on
17 (52%) had history of nicotine abuse and 20 (61%) of
the therapy of primary cystic neoplasms because of the
alcohol abuse. Six Patients had at least one episode of
small number of patients in studies and limited therapy
pancreatitis, five (15%) diabetes mellitus and seven
options. Today the most common approach in all cystic
(21%) suffered from a second neoplasm.
pancreatic lesions is curative resection [1–3, 10, 11]. De-
The standard radiographic method was CT (n ¼ 23,
pendent on size, symptoms, solid component and septa-
70%). Eighteen out of 23 histopathologic results con-
tion, some authors claim that selected patients with cystic
firmed the findings of CT prior to surgery (sensitivity
lesions <3 cm should be followed radiographically. Al-
50%). Endoscopic retrograde cholangiopancreatography
though malignant transformation is possible at low risk,
(ERCP) was performed in 11 (33%) with a correct histo-
mortality after pancreatic resection exceeds this level,
pathologic correlation within four patients, eight (24%)
even in high volume centers [10, 11].
patients underwent abdominal ultrasonography with four
The aim of this report is to review patients with
correlating diagnostic results, nine (27%) patients had
cystic neoplasms who underwent operative treatment at
MRIs with six correct diagnostic results and performed
a single institution, to review literature and to define an
endosonography correlated in four (12%) patients.
algorithm in decision making of either conservative oroperative treatment.
Symptomatic vs. asymptomatic patientsin the operative group
Eleven patients (33%) were discovered incidentally and 22
During the period 1997 to 2007, all patients diagnosed
(77%) had symptoms at the time of diagnosis. The most
with primary cystic neoplasms of the pancreas at the
common symptom was upper abdominal pain (n ¼ 14,
Cystic neoplasms of the pancreas: conservative or operative treatment?
Tab. 1: Clinic pathologic features of all patients and comparison of patients with malignant and benigncystic neoplasms of the pancreas in the operated group
42%). Six patients (18%) reported weight loss and four
(12%) had cholestasis. Other symptoms were abdominal
Thirty-three patients underwent surgical treatment. Thir-
pain, diarrhea and emesis. Symptomatic patients had an
teen patients (39%) underwent distal pancreatectomy, 8
average age of 66 years and asymptomatic patients of 63
patients (24%) had pylorus-preserving pancreaticoduode-
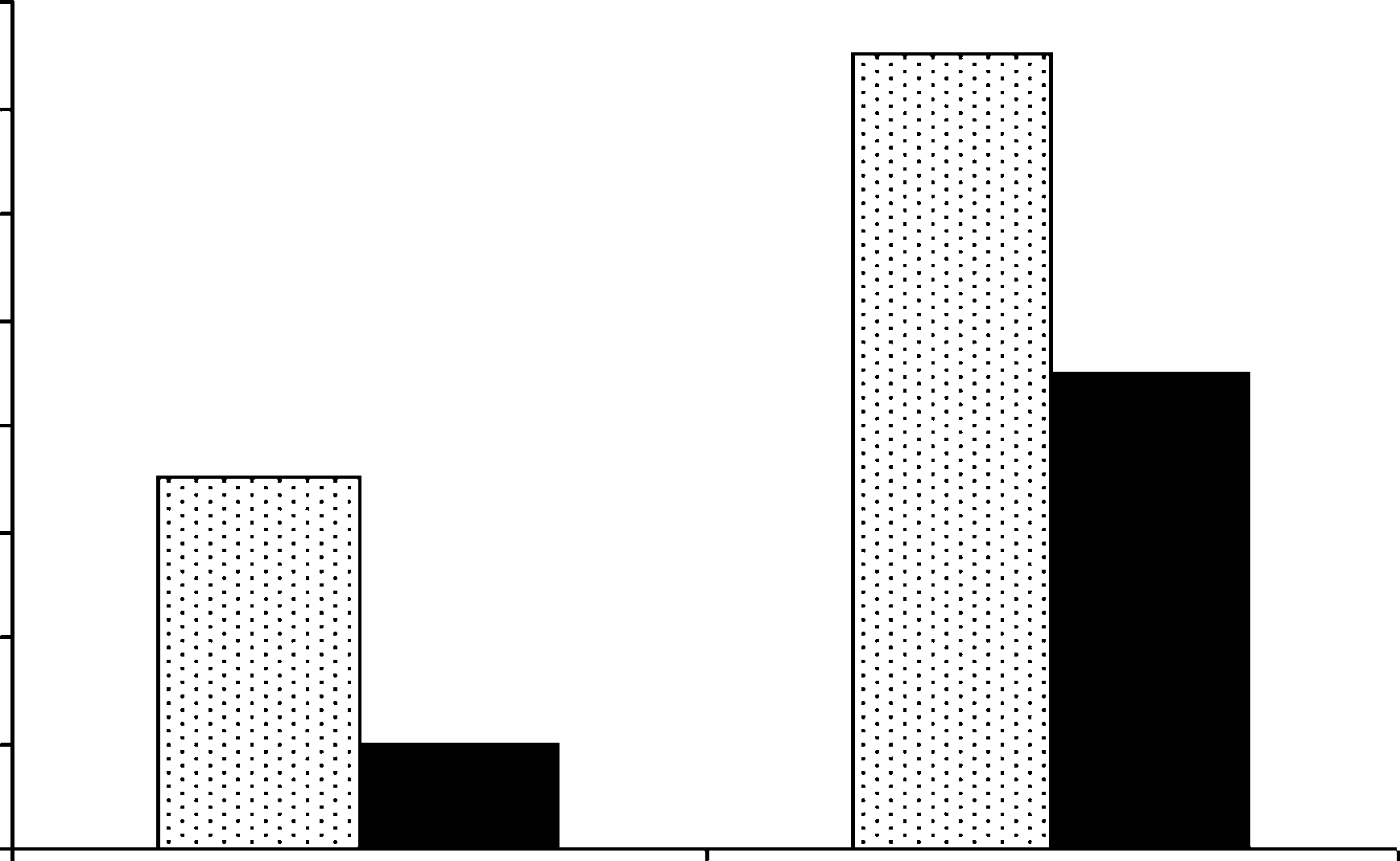
years (Fig. 1). Seven patients (78%) with a malignant cys-
nectomy and 6 patients (18%) classical whipple pancrea-
tic neoplasm reported symptoms at the time of diagnosis
ticoduodenectomy. Histopathologic findings were 12
and 15 patients (63%) died within the group of benign
MCNs (37%), 11 IPMNs (33%) and 10 SCAs (30%).
All three types of cystic neoplasms of the pancreas
occurred predominantly in women. There was no signifi-cant difference concerning patient’s age. Patients withSCAs reported the largest cyst size with a median of4.2 cm (2–10 cm). Further details of MCNs, SCAs andIPMNs are reported in Table 2.
There was no significant difference between median agesof patients with benign or malignant cystic neoplasms (68[59–83] vs. 67 [24–85] years). Five malignant (56%) and 19benign neoplasms (79%) were detected in women. Biliru-bin, CEA and CA 19-9 were more likely to be higher inpatients with malignant neoplasms. Benign and malig-nant cystic lesions are compared in Table 1.
Fig. 1: Symptoms and character of disease: Seven (78%) patients
The median age of two male and eight female patients
with malignant cystic neoplasms had symptoms at diagnosis versus15 (63%) of patients with benign cystic neoplasms
was 68 years (42–82) (Table 3). Two of 10 patients had
222 5/2008 Cystic neoplasms of the pancreas: conservative or operative treatment?
Tab. 2: Comparison between intraductal papillary mucinous neoplasm, mucinous cystic neoplasmand serous cystic neoplasm (operated group)
SD Standard deviation; MCN mucinous cystic neoplasms; SCA serous cystadenoma; IPMN intraductal papillary mucinous neoplasm.
Tab. 3: Demographics, cyst characteristics and therapy of 10 patients with conservative treatment
symptoms and eight were discovered incidentally. The
another patient an intra-abdominal abscess. During fol-
standard radiographic method was CT and MRI. An en-
low-up seven (21%) patients had a relapse of the cystic
doscopic fine needle aspiration was performed in five
(50%) patients, with negative cytology. Also two patients
All 10 patients who had conservative treatment
from 10 had cyst drainage. The median cyst size was 3 cm
were alive at the end of the study and did not report any
(1.5–12). The median radiographic follow-up time was 4.5
years (1–10). No patient reported a progredience, eightpatients had a constant cyst size and in two the size de-creased. Radiographic characteristics were without a solid
component, septation and infiltration.
Owing to modern imaging techniques, the incidence andimpact of primary cystic neoplasms of the pancreas isincreasing. In the past all patients underwent surgical
resection on behalf of this uncertain diagnosis leading
The 30-day mortality in the operative group was 0%. Five
to surgical overtreatment in some of them. Up to now
(15%) patients suffered from postoperative complications.
the problem is focused on missing consensus guidelines
Two patients developed pancreatic fistula: one patient
concerning diagnosis and treatment modalities for
had relaparotomy because of secondary hemorrhage,
patients suffering from cystic pancreatic lesions. Even
one patient developed an anastomotic dehiscence and
modern imaging and interventional techniques are able
Cystic neoplasms of the pancreas: conservative or operative treatment?
Fig. 2: Algorithm of how to manage patients with pancreatic cystic neoplasms. Operation should be performed in symptomatic patients or in caseof insecure diagnosis. Serous cystic neoplasms (SCN) smaller than 4 cm, no symptoms, can be followed conservatively. Intraductal papillarymucinous neoplasms (IPMN) of the main duct and mucinous cystic neoplasms (MCN) should be resected. IPMNs of a branch duct less than 1 cmcan be observed until growth occurs
to provide almost secure diagnosis in many patients;
intervals. According to the low perioperative mortality in
there are still numerous depending on surgical resection
centers of pancreatic surgery, they should be resected to
to verify the correct pathologic finding. Depending on
avoid the potential risk of malignancy, if diagnosis is not
cyst size, architecture and symptoms, within a defined
100% clear and the patient is young or in good physical
group of patients, the physician is confronted with the
condition. Some also claim that cysts greater than 4 cm
nearly equal risk of operative mortality and the risk of
indicate operation, because the median growth rate of
under diagnosed malignancy. The right decision to ob-
the neoplasms is significantly greater in larger lesions
serve or operate exceptionally depends on the correct
(0.12 cm=year for lesions <4 cm versus 1.98 cm=year for
diagnosis based on radiological imaging supported by
biopsy and cytology [12]. In particular small asymptom-
Mucinous cystic neoplasms are of unsecured dignity
atic lesions which potentially can be treated conservative
and have a high potential of malignancy or malignant
are the most difficult to differentiate because of the ab-
transformation. Patients should undergo resection after
sence of clear pathognomonic findings (Fig. 2).
diagnosis is secured, regardless of cyst size.
Until now the greatest series of 369 conservatively
Intraductal papillary mucinous neoplasms are also
treated patients is reported by Allen et al. [10]. In this
of high potential of malignancy but IPMN involving the
study the presence of a solid component was the stron-
main duct have a higher risk than the branch duct (64%
gest factor leading to surgical resection, followed by cyst
vs. 19%) [14]. Therefore, IPMN with main duct disease
size, age and symptoms. All non-operative treated
should be resected and IPMN with branch duct disease
patients had small cysts, mean being 2.4 cm, without a
<1–3 cm can be observed, if there is no enlargement of
solid component. Twenty nine of them underwent resec-
cyst size, symptoms or solid component of the lesion.
tion, due to changes during follow-up. Adenocarcinoma
During the diagnostic process, there are cases
was found in 8 of these patients, median follow-up was 24
where it is not possible to determine the type of the
cystic pancreatic lesion. This makes decision in conser-
Similar results are reported by Walsh et al. [13] on
vative or operative treatment difficult. Table 4 shows
treatment strategy of pancreatic cystic lesions from ac-
Serous cystic neoplasms are benign lesions. If diag-
tual literature presenting the largest number of cases
nosis is clear, cysts do not contain a solid component and
the patient is asymptomatic, they may be managed con-
Treatment recommendations are differing. There
servatively. These cysts can be followed by computer to-
are comments that with some selected patients, cyst size
mography or magnet resonance tomography at regular
smaller than 3 cm without solid component, do not need
224 5/2008 Cystic neoplasms of the pancreas: conservative or operative treatment?
Tab. 4: Treatment strategy of pancreatic cysts from different authors
Smaller than 3 cm without solid component does not operate
Symptoms, size, age are not sufficiently reliable indetermining the malignant potential
operate if increasing, symptomatically and in fit elders
operate symptomatically SCAs, all MCN, all unclear cystic neoplasms
SCA Serous cystadenoma; MCN mucinous cystic neoplasm.
the strict strategy of operating. This group of patients
have a low risk of malignancy, which approximate the risk
[1] Spinelli KS, Fromwiller TE, Daniel RA, Kiely JM, Nakeeb A,
Komorowski RA, Wilson SD, Pitt HA. Cystic pancreatic neo-
Other investigators advocate surgical treatment for
plasms: observe or operate. Ann Surg 2004;239:651–7; discus-
all primary cystic lesions of the pancreas. Characteristics
[2] Brugge WR, Lauwers GY, Sahani D, Fernandez-del Castillo C,
such as cyst size, age and symptoms are not precise
Warshaw AL. Cystic neoplasms of the pancreas. N Engl J Med
enough to determine the malignant potential [15]. Malig-
nant or premalignant pancreatic cysts were found in 47%
[3] Sakorafas GH, Sarr MG. Cystic neoplasms of the pancreas; what
of asymptomatic patients. They argue that cyst size smal-
a clinician should know. Cancer Treat Rev 2005;31:507–35.
[4] Compagno J, Oertel JE. Mucinous cystic neoplasms of the
ler than 2 cm does not predict malignant or benign po-
pancreas with overt and latent malignancy (cystadenocarci-
tential. Within patients older than 70 years, the indication
noma and cystadenoma). A clinicopathologic study of 41 cases.
of surgical treatment is more difficult. There is no rep-
[5] Sarr MG, Carpenter HA, Prabhakar LP, Orchard TF, Hughes S,
orted higher risk for malignancy, within these patients,
van Heerden JA, DiMagno EP. Clinical and pathologic correla-
but an increased risk of operation and short life expectan-
tion of 84 mucinous cystic neoplasms of the pancreas: can one
cy after resection. Therefore a conservative approach may
reliably differentiate benign from malignant (or premalignant)neoplasms? Ann Surg 2000;231:205–12.
be acceptable for the elderly patient. Finding the best
[6] Kosmahl M, Pauser U, Anlauf M, Sipos B, Peters K, Luttges J,
treatment modality for each patient, they also claim that
Kloppel G. Cystic pancreas tumors and their classification:
correct preoperative diagnosis is achieved only in 22% of
features old and new. Pathologe 2005;26:22–30.
[7] Goh BK, Tan YM, Yap WM, Cheow PC, Chow PK, Chung YF,
Wong WK, Ooi LL. Pancreatic serous oligocystic adenomas:
In the present study, we found similar results. Neither
clinicopathologic features and a comparison with serous micro-
cyst size nor symptoms predict malignancy. Cyst size of
cystic adenomas and mucinous cystic neoplasms. World J Surg
malignant neoplasms ranged from 2 to 12 cm in the pres-
¨ gger R. Pancreatic carcinoma. Eur Surg 2006;38:112–17.
ent analysis. Comparable to investigations by Fernandez
[9] Tseng JF, Warshaw AL, Sahani DV, Lauwers GY, Rattner DW,
et al., we could not find a significant correlation between
Fernandez-del Castillo C. Serous cystadenoma of the pancreas:
cyst size and malignancy [16]. Two (18%) from 11 with
tumor growth rates and recommendations for treatment. Ann
incidental found cysts and seven (31%) from 22 symptom-
Surg 2005;242:413–9; discussion 419–21.
[10] Allen PJ, D’Angelica M, Gonen M, Jaques DP, Coit DG,
atic cysts were malignant neoplasms (p <0.05). Malignan-
Jarnagin WR, DeMatteo R, Fong Y, Blumgart LH, Brennan
cy was observed only in patients older than 61 years
MF. A selective approach to the resection of cystic lesions of
compared to patients with benign lesions, who ranged
the pancreas: results from 539 consecutive patients. Ann Surg2006;244:572–82.
from 24 to 85 years. Age was, however, not reported as a
[11] Allen PJ, Jaques DP, D’Angelica M, Bowne WB, Conlon KC,
prognostic factor in larger trials and patients’ number with-
Brennan MF. Cystic lesions of the pancreas: selection criteria
in this study is too small to make further conclusions.
for operative and nonoperative management in 209 patients. J Gastrointest Surg 2003;7:970–7.
CT and MRI are the best imaging modalities for
[12] Wrba F. Oncological surgery and standards in surgical patholo-
detection, characterization and follow-up of cystic neo-
plasm [17, 18], but they are not 100% reliable in the
[13] Walsh RM, Vogt DP, Henderson JM, Zuccaro G, Vargo J, Dumot
diagnosis of pancreatic cysts. CT is able to reliably differ-
J, Herts B, Biscotti CV, Brown N. Natural history of indetermi-nate pancreatic cysts. Surgery 2005;138:665–70; discussion
entiate between serous, mucinous and intraductal papil-
lary cystic neoplasms of the pancreas [19]. Preoperative
[14] Serikawa M, Sasaki T, Fujimoto Y, Kuwahara K, Chayama K.
CT can also be used to different malignant intraductal
Management of intraductal papillary-mucinous neoplasm ofthe pancreas: treatment strategy based on morphologic classi-
papillary neoplasms. Signs like dilated main duct, mural
fication. J Clin Gastroenterol 2006;40:856–62.
nodules or thickness of cyst wall can predict malignancy
[15] Goh BK, Tan YM, Cheow PC, Chung YF, Chow PK, Wong WK, Ooi
[20]. In the present report we had five from 23 CTs that
LL. Cystic lesions of the pancreas: an appraisal of an aggressive
resectional policy adopted at a single institution during 15 years. Am J Surg 2006;192:148–54.
In conclusion, decision making in conservative or
[16] Fernandez-del Castillo C, Targarona J, Thayer SP, Rattner DW,
operative treatment should depend on size, symptoms,
Brugge WR, Warshaw AL. Incidental pancreatic cysts: clinico-
patient age and reliable secure diagnosis. In the case of
pathologic characteristics and comparison with symptomaticpatients. Arch Surg 2003;138:427–34; discussion 433–34.
uncertain cyst character, surgical resection is indicated
[17] Sahani DV, Kadavigere R, Saokar A, Fernandez-del Castillo C,
Brugge WR, Hahn PF. Cystic pancreatic lesions: a simple imag-
Cystic neoplasms of the pancreas: conservative or operative treatment?
ing-based classification system for guiding management.
noma and intraductal papillary mucinous tumor. Am J
[18] O’Toole D, Palazzo L, Hammel P, Ben Yaghlene L, Couvelard A,
[20] Chiu SS, Lim JH, Lee WJ, Chang KT, Oh DK, Lee KT, Lee JK, Choi
Felce-Dachez M, Fabre M, Dancour A, Aubert A, Sauvanet A,
SH. Intraductal papillary mucinous tumour of the pancreas:
Maire F, Levy P, Ruszniewski P. Macrocystic pancreatic cystade-
differentiation of malignancy and benignancy by CT. Clin
noma: the role of EUS and cyst fluid analysis in distinguishing
mucinous and serous lesions. Gastrointest Endosc 2004;59:823–9.
[21] Le Borgne J, de Calan L, Partensky C. Cystadenomas and
[19] Kim SY, Lee JM, Kim SH, Shin KS, Kim YJ, An SK, Han CJ, Han JK,
cystadenocarcinomas of the pancreas: a multiinstitutional ret-
Choi BI. Macrocystic neoplasms of the pancreas: CT differenti-
rospective study of 398 cases. French Surgical Association. Ann
ation of serous oligocystic adenoma from mucinous cystade-
226 5/2008 Cystic neoplasms of the pancreas: conservative or operative treatment?
Innovator duty of care in the pharmaceutical industryDoes the inventor or “innovator” of a brand-name drug have a duty of care to the consumers of that drug’s generic equivalent manufactured by a competitor? The Ontario Superior Court of Justice considered this question in the recent case of Goodridge v Pfizer Canada1 and determined that, for now, no such duty exists. In that decision, th
 Tab. 1: Clinic pathologic features of all patients and comparison of patients with malignant and benigncystic neoplasms of the pancreas in the operated group
42%). Six patients (18%) reported weight loss and four
(12%) had cholestasis. Other symptoms were abdominal
Thirty-three patients underwent surgical treatment. Thir-
pain, diarrhea and emesis. Symptomatic patients had an
teen patients (39%) underwent distal pancreatectomy, 8
average age of 66 years and asymptomatic patients of 63
patients (24%) had pylorus-preserving pancreaticoduode-
years (Fig. 1). Seven patients (78%) with a malignant cys-
nectomy and 6 patients (18%) classical whipple pancrea-
tic neoplasm reported symptoms at the time of diagnosis
ticoduodenectomy. Histopathologic findings were 12
and 15 patients (63%) died within the group of benign
MCNs (37%), 11 IPMNs (33%) and 10 SCAs (30%).
Tab. 1: Clinic pathologic features of all patients and comparison of patients with malignant and benigncystic neoplasms of the pancreas in the operated group
42%). Six patients (18%) reported weight loss and four
(12%) had cholestasis. Other symptoms were abdominal
Thirty-three patients underwent surgical treatment. Thir-
pain, diarrhea and emesis. Symptomatic patients had an
teen patients (39%) underwent distal pancreatectomy, 8
average age of 66 years and asymptomatic patients of 63
patients (24%) had pylorus-preserving pancreaticoduode-
years (Fig. 1). Seven patients (78%) with a malignant cys-
nectomy and 6 patients (18%) classical whipple pancrea-
tic neoplasm reported symptoms at the time of diagnosis
ticoduodenectomy. Histopathologic findings were 12
and 15 patients (63%) died within the group of benign
MCNs (37%), 11 IPMNs (33%) and 10 SCAs (30%).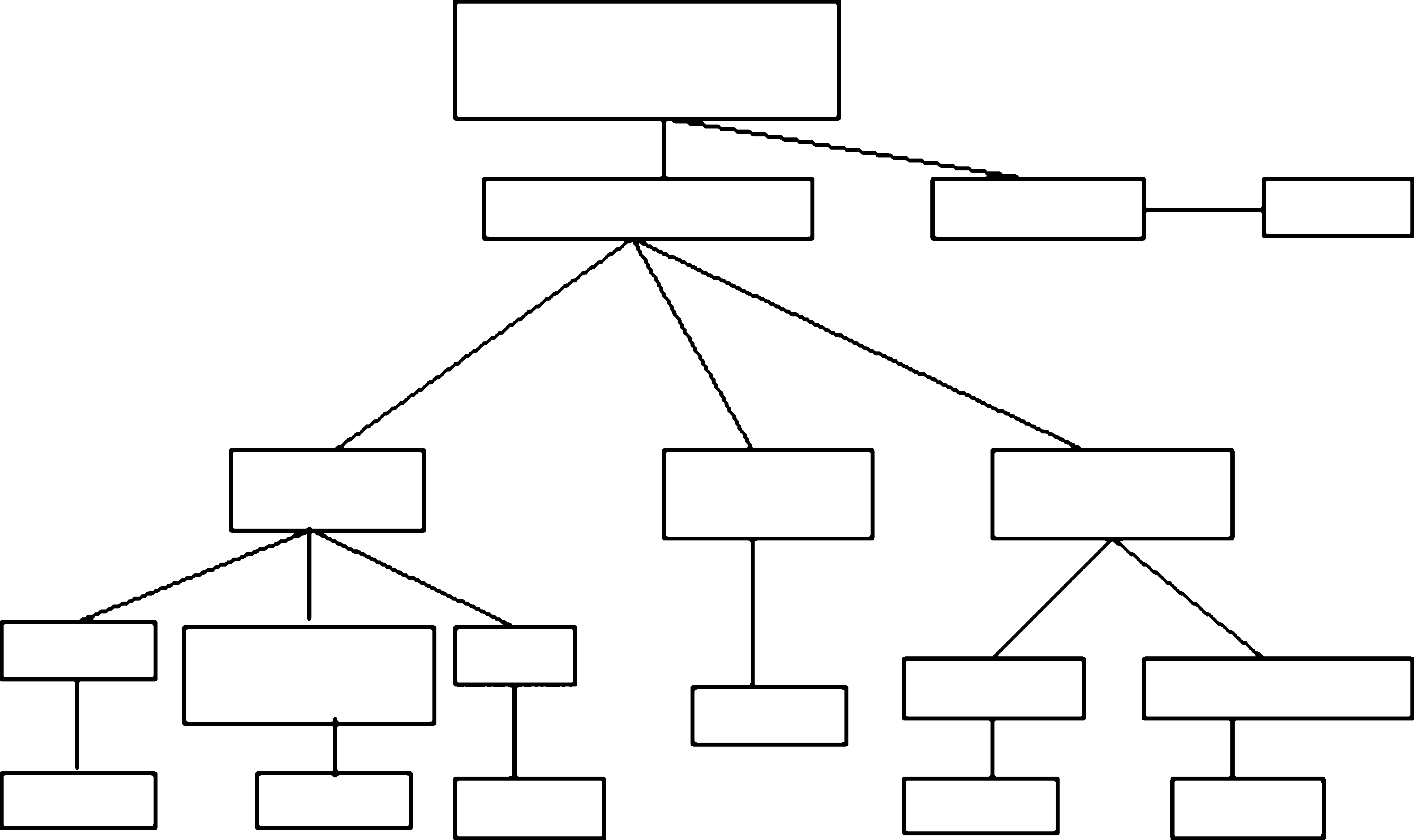 Fig. 2: Algorithm of how to manage patients with pancreatic cystic neoplasms. Operation should be performed in symptomatic patients or in caseof insecure diagnosis. Serous cystic neoplasms (SCN) smaller than 4 cm, no symptoms, can be followed conservatively. Intraductal papillarymucinous neoplasms (IPMN) of the main duct and mucinous cystic neoplasms (MCN) should be resected. IPMNs of a branch duct less than 1 cmcan be observed until growth occurs
to provide almost secure diagnosis in many patients;
intervals. According to the low perioperative mortality in
there are still numerous depending on surgical resection
centers of pancreatic surgery, they should be resected to
to verify the correct pathologic finding. Depending on
avoid the potential risk of malignancy, if diagnosis is not
cyst size, architecture and symptoms, within a defined
100% clear and the patient is young or in good physical
group of patients, the physician is confronted with the
condition. Some also claim that cysts greater than 4 cm
nearly equal risk of operative mortality and the risk of
indicate operation, because the median growth rate of
under diagnosed malignancy. The right decision to ob-
the neoplasms is significantly greater in larger lesions
serve or operate exceptionally depends on the correct
(0.12 cm=year for lesions <4 cm versus 1.98 cm=year for
diagnosis based on radiological imaging supported by
biopsy and cytology [12]. In particular small asymptom-
Mucinous cystic neoplasms are of unsecured dignity
atic lesions which potentially can be treated conservative
and have a high potential of malignancy or malignant
are the most difficult to differentiate because of the ab-
transformation. Patients should undergo resection after
sence of clear pathognomonic findings (Fig. 2).
Fig. 2: Algorithm of how to manage patients with pancreatic cystic neoplasms. Operation should be performed in symptomatic patients or in caseof insecure diagnosis. Serous cystic neoplasms (SCN) smaller than 4 cm, no symptoms, can be followed conservatively. Intraductal papillarymucinous neoplasms (IPMN) of the main duct and mucinous cystic neoplasms (MCN) should be resected. IPMNs of a branch duct less than 1 cmcan be observed until growth occurs
to provide almost secure diagnosis in many patients;
intervals. According to the low perioperative mortality in
there are still numerous depending on surgical resection
centers of pancreatic surgery, they should be resected to
to verify the correct pathologic finding. Depending on
avoid the potential risk of malignancy, if diagnosis is not
cyst size, architecture and symptoms, within a defined
100% clear and the patient is young or in good physical
group of patients, the physician is confronted with the
condition. Some also claim that cysts greater than 4 cm
nearly equal risk of operative mortality and the risk of
indicate operation, because the median growth rate of
under diagnosed malignancy. The right decision to ob-
the neoplasms is significantly greater in larger lesions
serve or operate exceptionally depends on the correct
(0.12 cm=year for lesions <4 cm versus 1.98 cm=year for
diagnosis based on radiological imaging supported by
biopsy and cytology [12]. In particular small asymptom-
Mucinous cystic neoplasms are of unsecured dignity
atic lesions which potentially can be treated conservative
and have a high potential of malignancy or malignant
are the most difficult to differentiate because of the ab-
transformation. Patients should undergo resection after
sence of clear pathognomonic findings (Fig. 2).