Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
Epi_1007.tex
Epilepsia, 48(3):464–469, 2007 Blackwell Publishing, Inc.
C 2007 International League Against Epilepsy
Compulsory Generic Switching of Antiepileptic Drugs: High
Switchback Rates to Branded Compounds Compared with Other
∗Frederick Andermann, †Mei Sheng Duh, ‡Antoine Gosselin, and ‡Pierre Emmanuel Paradis
∗Montreal Neurological Institute and Hospital, McGill University, Montr´eal, Qu´ebec, Canada; †Analysis Group, Inc., Boston,Massachusetts, U.S.A.; and ‡Groupe d’Analyse, Lt´ee, Montr´eal, Qu´ebec, CanadaSummary: Purpose: Compulsory generic substitution of Results: The 1,354 patients (403 monotherapy, 951 polyther-
antiepileptic drugs (AEDs) may lead to adverse effects in
apy) were prescribed generic LTG, of whom 12.9% switched
epilepsy patients because of seizure recurrence or increased tox-
back to Lamictal (11.7% monotherapy, 13.4% polytherapy).
icity. The study objectives were (a) to quantify and compare the
Switchback rates of other AEDs were ∼20% for CLB and
switchback rates from generic to brand-name AEDs versus non-
VPA. The switchback rates for AEDs were substantially higher
AEDs, and (b) to assess clinical implications of switching from
than for non-AEDs (1.5–2.9%). Significant increases in LTG
branded Lamictal to generic lamotrigine (LTG) and whether sig-
doses were observed after generic substitution for those who did
nals exist suggesting outcome worsening.
not switch back (6.2%; p < 0.0001). The average number of
Methods: By using a public-payer pharmacy-claims database
codispensed AEDs and non-AED drugs significantly increased
from Ontario, Canada, switchback rates from generic to branded
(p < 0.0001) after LTG generic entry, especially in the generic
AEDs [Lamictal, Frisium (clobazam; CLB), and Depakene
(VPA; divalproex)] were calculated and compared with non-
Conclusions: These results reflect poor acceptance of switch-
AED long-term therapies, antihyperlipidemics and antidepres-
ing AEDs to generic compounds. They may also indicate
sants, in January 2002 through March 2006. We then assessed
increased toxicity and/or loss of seizure control associated
pharmacy utilization and AED dosage among LTG patients
with generic AED use. Key Words: Epilepsy—Antiepileptic
switching back to branded Lamictal compared with those staying
drugs—Generic substitution—Lamictal—Lamotrigine.
In recent years, increasing medical costs have forced
(AUC) and peak plasma concentration (Cmax) lie within
healthcare systems to adopt measures to limit expendi-
an interval of 80% to 125% (Borgherini, 2003). The FDA
ture and maximize cost savings. A common example has
accepts −20% to 25% variation in AUC and Cmax that
been the encouragement or mandatory requirement for
are considered bioequivalent, whereas the brand standard
the use of cheaper generic medicines instead of branded
ranges from −5% to +5% (Borgherini, 2003). Therefore
products. However, as generic medications are required to
it is theoretically possible for a patient to receive an al-
demonstrate only short-term bioequivalence to be granted
most 50% increase in serum concentration if switched
product license, their bioavailability may differ from that
from a low-bioavailability generic formulation to a high-
of their branded counterparts, which could lead to de-
bioavailability one (Feely et al., 2005). An additional con-
creased efficacy and/or tolerability. Specifically, the U.S.
cern is that bioavailability studies are carried out on a small
Food and Drug Administration (FDA) criteria for bioe-
number of healthy volunteers by using single doses of a
quivalence are designed to achieve 90% confidence that
drug. These studies may not represent a clinical practice
the ratios of the test to reference log-transformed mean
setting, where patients have a wide range of characteris-
values for area under the plasma concentration–time curve
tics, may have other concomitant diseases, and can usepotentially interacting drugs (Besag, 2000).
In medication classes in which a “narrow therapeutic
Accepted December 8, 2006. Address correspondence and reprint requests to Dr. F. Ander-
index” is present, such as antiepileptic drugs (AEDs),
mann at Department of Neurology and Paediatrics, McGill Univer-
generic substitution raises particular concern. In addition
sity, 3801 University Street, Montreal QC H3A 2B4, Canada. E-mail:
to individual response, tolerability and toxicity are im-
portant considerations when selecting an AED therapy. ADVERSE OUTCOMES WITH GENERIC SWITCHING TO LAMOTRIGINE
Many AEDs are CNS depressants and may produce
in Ontario before and after the government-mandated
undesirable sedation impact on activities requiring skilled
switch, by using LTG as a case-study example.
coordination and alertness (Sander, 2004). Discontinua-tion of or changeover from one AED to another must
be done gradually to avoid precipitating seizures. For a
Data source
patient in stable long-term control, prevention of seizure
We used a public-payer database from Ontario, Canada,
recurrence is paramount, as even a single breakthrough
comprising patient-level prescription drug dispensing
seizure could have serious consequences, on both a per-
claims paid for by the Ontario Drug Benefit (ODB) Formu-
sonal (loss of driver’s license, employment, injury to self,
lary. Data elements included patient demographics, drug
etc.) and a social level (injury to others, increased health
use, product manufacturer, strength, form, and treatment
cost to society) (Feely, 2005; Crawford, 2006). As short-
term bioequivalence may not translate to equivalent ef-ficacy with respect to long-term seizure control, generic
Study design
AEDs may be less acceptable and paradoxically increase
The objectives of the study were twofold. First, we
aimed to quantify the switchback rates from generic to
Increased toxicity or intolerance and/or breakthrough
brand-name AEDs in comparison with other drugs used
seizures have been reported after generic substitutions of
over the long term. Second, we documented the poten-
AEDs, including phenytoin (PHT) (Tyrer et al., 1970), val-
tial adverse clinical consequences of generic switching,
proic acid (VPA) (Macdonald, 1987), primidone (PRM)
(Wyllie et al., 1987) and carbamazepine (CBZ) (Gilman
To address the first objective, the switchback rates were
et al., 1993). In a survey of 301 neurologists in the United
calculated from generic to three branded AEDs: Lamictal,
States, 67.8% reported breakthrough seizures, and 56% re-
Frisium, and Depakene, in comparison with other com-
ported increased side effects in their patients after a switch
monly used long-term medications, antihyperlipidemics
from brand-name to generic AEDs (Wilner, 2004). In the
(Statin 1: simvastatin, Zocor) and antidepressants [se-
largest patient survey reported to date, involving 251 pa-
lective serotonin reuptake inhibitor (SSRI) 1: fluoxetine,
tients who had been switched to generic AEDs, 10.8%
Prozac; and SSRI 2, citalopram, Celexa]. In every case,
experienced a confirmed breakthrough seizure or toxicity
only one brand name was available for each of these prod-
attributable to the substitution (Crawford et al., 1996).
ucts, whereas five different generic formulations exist for
Analyses have suggested that the cost saved by generic
Lamictal, six for Frisium, 15 for Depakene, and >10
switching of AEDs could be outweighed by the price
generic formulations for other non-AEDs. To be selected
of increased monitoring and loss of seizure control.
in this study, the drug had to be on the market only as a
(Crawford et al., 1996; Jobst and Holmes, 2004). An-
branded version in 1995 or later, and then a generic for-
other problem is that physicians typically underestimate
mulation had to be introduced in 2004 or before. Of all
the frequency of generic substitution taking place at the
the possible AED candidates, only Neurontin (gabapentin)
pharmacy (Guberman and Corman, 2000; Wilner, 2004).
was excluded, as it is also widely used for indications other
Consequently, many recommend that physicians be more
vigilant in their prescription-writing practices to pre-
“Switchback” was defined as switching a patient from
vent unwarranted generic substitution (Wilner, 2004). The
the branded drug to the generic, and then back to the
American Academy of Neurology has issued a guideline
branded drug. Switchback rates were estimated for pa-
recommending that switching between proprietary and
tients initially taking the branded drug during a time when
generic formulations of AEDs be avoided unless medi-
no generic version was available in Ontario and who were
cally indicated (American Academy of Neurology, 1990).
then switched to a generic formulation. Among those pa-
tients, those who were converted back to the branded drug
Brentford, Middlesex, U.K.] is a newer drug in the AED
were considered switchback patients. Figure 1 lists the
formulary that has a narrow therapeutic index, but better
drugs under study, their therapeutic class, and the date
toxicity profile and less drug interaction compared with
(quarter/year) of generic entry on the Ontario market.
older AEDs. It is one of the first of the new-generation
For all these medications, the study populations com-
AEDs to have a generic version, and understanding the
prised patients who continuously used the branded drugs
effect of substitution of branded Lamictal to generic LTG
for ≥3 months in the 6 months preceding generic entry.
would further the knowledge in the generic substitution of
“Continuous use” was defined as drug supplies without
new AEDs. Starting in January 2003, the province of On-
a gap of >30 days, or a time interval between two dis-
tario required that all branded prescriptions of Lamictal
pensing dates of ≤60 days. The study period ranged from
be switched to its generic version. In this study, we assess
1 year before generic entry until March 2006. Because
the impact of generic substitution by comparing pharmacy
generic substitution is compulsory in Ontario, the use of a
claims data on cohorts of epilepsy patients receiving AEDs
branded medication is not allowed without a physician
FIG. 1. Patient disposition. SSRI, selective serotonin reuptake inhibitor.
letter of medical necessity. Therefore we did not use
Potential adverse clinical consequences associated with
the few patients who remained taking their branded
switching from Lamictal to lamotrigine
medication after generic entry as a comparator group, as
The following outcomes were used as proxies for possi-
it was too small (∼2%) for a reliable statistical analysis.
ble adverse clinical consequences: mean and median daily
For the second objective, we assessed the potential clin-
Lamictal or LTG doses and utilization of concomitant
ical consequences of switching from branded Lamictal to
AED and non-AED medications. These outcomes were
generic LTG by using two cohorts of patients: (a) those
compared in the following time periods: 90-day base-
switching back to branded Lamictal after being converted
line branded Lamictal period, generic LTG period, and
to generic LTG (switchback group), and (b) those stay-
switchback to branded Lamictal period among those who
ing with generic LTG after generic entry (generic group)
as of January 1, 2003. The baseline dosages and numberof entities for this case study were calculated by using a
Statistical analysis
90-day period of Lamictal use before generic substitution
Univariate statistics were calculated to describe popula-
occurred. Similar to the switchback analysis, the follow-up
tion characteristics, switchback rates, and dosages. Statis-
period lasted until March 2006. A stratified analysis was
tical comparisons of means of continuous variables before
conducted on Lamictal patients receiving monotherapy
and after generic entry were conducted by using paired
versus polytherapy of AEDs. Monotherapy was defined
Student’s t-tests. Comparisons of medians were tested
as patients taking only Lamictal during the 90 days before
based on Signed Rank tests. Linear regressions were used
generic entry, whereas polytherapy referred to Lamictal
to measure changes occurring during the generic period.
patient using at least one other AED at the baseline pe-
Statistical significance was defined at a two-sided 0.05
α level. All statistical analyses were performed by usingSAS release 9.1.3 (SAS Institute, Inc., Cary, NC, U.S.A.). Outcome measures
Switchback rates were estimated by using the Kaplan–
Meier method, which is a conditional probability approach
Patient characteristics
based on the subjects who were on the generic drug at
Figure 1 depicts the patient disposition and sample size
the beginning of the interval. This calculation yields the
for each of the seven drugs under study, stratified by
probability that a patient will eventually switch back to the
monotherapy and polytherapy. A large share of branded
branded drug after being switched to the generic. Patients
products users (83% to 93%) received generic dispens-
who were lost to follow-up were censored. The switch-
ings after generic availability. Most AED patients were
back rate was calculated as the cumulative probability of
polytherapy users (59% to 91%), meaning that they also
a patient switching back to the branded drug, given that
received another AED during the baseline period. Almost
he was on the generic drug at each time interval.
all patients taking Statin 1 were receiving polytherapy
ADVERSE OUTCOMES WITH GENERIC SWITCHING TO LAMOTRIGINETABLE 1. Baseline characteristics of study populations TABLE 2. Patient disposition and baseline characteristics of
Patients in 90-day baseline with at least
SSRI, selective serotonin reuptake inhibitor. bSum could differ from patient disposition because of unknown
(96%), whereas a majority of SSRI 1 (9%) and SSRI 2(20%) users were not.
Table 1 describes the age and gender distributions of
rate was higher among those taking polytherapy of AEDs
patients in each drug-user cohort. Compared with other
compared with monotherapy (13.4 vs. 11.7%). A larger
AED users, Depakene patients were older (mean age, 44.4
share of polytherapy patients switched back in the case for
years), whereas Lamictal was used by more female pa-
Depakene (21.3 vs. 20.6%), but not for Frisium (19.8vs.
tients (53.5%). In the other three non-AED groups, Statin
27.1%). In contrast, the switchback rates for non-NTI
1 and SSRI 2 patients were older than SSRI 1 patients
drugs were substantially lower at 1.5–2.9% for the statins
(73.8 years, 69.0 years, and 56.0 years, respectively), and
the proportion of female patients was higher for SSRI 1
Dosing patterns
Table 3 shows the dosing patterns of Lamictal and LTG,
Table 2 describes the patient disposition and charac-
before and after generic entry. Among the switchback
teristics of patients in the Lamictal case study. Because
group, the average daily prescription dose of Lamictal was
this was a large subset of the previous Lamictal cohort,
at 252.2 mg during the baseline period before generic en-
their age and gender characteristics were almost identical
try, and this average dosage barely increased to 254.6 mg
(mean age, 38.5 years; 53.2% female patients).
(0.9% increase; p = 0.6925) during the generic period, fol-
Switchback rates
lowed by a decrease to 250.7 mg when switched back to
Figure 2 compares the switchback rates from generic
branded Lamictal (−1.5%; p = 0.8836). The median daily
to branded drugs under study. AEDs had much higher
prescription dose remained constant at 200 mg during the
switchback rates compared with other long-term drugs.
Depakene (20.9%) and Frisium (20.7%) patients experi-
Among the generic group, the average daily dispensed
enced the highest switchback rates, followed by 12.9% for
dose of Lamictal was 255.3 mg at baseline, with a
Lamictal patients. In the case of Lamictal, the switchback
significant dose increase to 271.1 mg (6.2% increase;
FIG. 2. Switchback rates: Kaplan–Meier estimations. SSRI, selective serotonin re- uptake inhibitor. TABLE 3. Dosing patterns of branded Lamictal and generic lamotrigine
Mean, Paired t test testing whether the dose change when switching from brand to generic is significantly different from zero; median, signed rank
p < 0.0001) during the generic period. The corresponding
−4.6%; p = 0.125; non-AEDs, −8.8%; p = 0.042). In
median dose also increased from a baseline of 200 mg to
the generic group, both numbers of entities increased and
232.5 mg after the generic switch (16.3%; p < 0.0001).
were statistically significant (AED, 13.4%; p < 0.0001;
To further characterize the dosage pattern for the generic
non-AED, +19.3%; p < 0.0001).
group, a regression analysis was performed. The regres-sion coefficient suggested that the dose increase was at15.4mg/day (p < 0.0001) at generic entry, with an aver-
DISCUSSION
age trend increase of 0.43 mg/day (p < 0.0001) during the
We addressed an important and often underrated issue
regarding generic prescribing. The findings illustrate howand why AEDs are different from other medications when
Use of concomitant medications
it comes to the desirability of switching to generic equiva-
Table 4 presents the impact of generic entry on the use of
lents. To the best of our knowledge, the present study is the
AED and non-AED medications, both of which increased
first to assess the switchback rates from generic to branded
significantly for all patients (AED, 11.0%; p < 0.0001;
AEDs compared with switchback rates for non-AEDs. The
non-AED, +15.6%; p < 0.0001). The number of codis-
high rate of switchback to branded AEDs (12.9 to 20.9%)
pensed entities decreased in the switchback group (AEDs,
compared with non-AEDs (1.5 to 2.9%) observed in thisstudy is particularly impressive in light of the strict Ontariorules favoring generics and the fact that the switchback to
TABLE 4. Use of concomitant medications: branded Lamictal
branded medications is not allowed without a physicianletter of medical necessity.
The ODB imposes a steep hurdle to prevent patients
from switching back to a brand-name drug without doc-umented medical necessity from the attending physician.
Taking LTG as an example: since generic LTG was avail-
able in the ODB formulary in January 2003, all branded
Lamictal prescriptions had to be switched to generic LTG
at the pharmacy level, even if the prescription mentioned
“do not substitute.” Doctors would have to petition to let
a patient continue to take Lamictal by filing an adversedrug reaction form to Health Canada with all the required
Paired t-test testing indicated whether the change in the number of
entities when switching from brand to generic is significantly different
documentation, for the plan to pay for the brand medica-
tion. Therefore the fact that such a significant proportion
ADVERSE OUTCOMES WITH GENERIC SWITCHING TO LAMOTRIGINE
of patients and physicians would go to these extents to
der or neuropathic pain may also have been included in the
switch back to the original branded AED reflects both their
study population, which may explain the relatively large
experience and their sentiments toward generic AEDs.
share of polytherapy users in this study (Sander, 2004).
These high switchback rates may reflect a common at-
Second, the motive for drug selection cannot be deter-
titude among patients with epilepsy who are anxious to
mined from claims data. It is possible that the decision
avoid having a recurrence, actual loss of seizure control,
process to switch to generic or back to brand was driven
by nontherapeutic factors, such as inability to afford the
Our findings add to the literature surrounding generic
branded drug, provincial rules governing generic substi-
switching of AEDs and support prior studies demonstrat-
tution, or absence of a particular drug in the pharmacy
ing that generic AEDs could be less effective or tolerable
stock. Finally, our study is subject to limitations inherent
compared with their branded counterparts (MacDonald,
to claims data, including potential inaccuracies in billing,
1987; Welty, 1992; Jain, 1993; Wyllie, 2004; Crawford et
dispensing dates, drug doses, and drug codes.
The high switchback rates and dosing changes found in
Although results based on claims data must be in-
this study may be associated with adverse clinical conse-
terpreted with caution, this significant increase in AED
quences due to compulsory switching of branded AEDs to
and non-AED drug dispensing after the generic switch
generic. These findings further abet the guidelines set by
is nonetheless intriguing and could potentially reflect ad-
the American Academy of Neurology to avoid switching
verse effects associated with generic LTG. Regardless of
between proprietary and generic formulations of AEDs
the pharmacokinetic data for generic versus brand-name
preparations of AEDs, this study shows that patients with
Acknowledgment: This research was funded by Glaxo-
epilepsy are less likely to be satisfied with generic switches
than are patients with other long-term medical conditions. The reasons for this phenomenon are beyond the dataavailable in this article, but on this issue, the motivation is
REFERENCES
less important than the fact that, when it comes to AEDs,forced generic substitution is less likely to be well toler-
American Academy of Neurology. (1990) Assessment: generic substi-
tution for antiepileptic medication. Neurology 40:1641–1643.
ated and may lead therefore to more medical and social
Besag FM. (2000) Is generic prescribing acceptable in epilepsy? Drug
The statistically significant increase in dosage from
Borgherini G. (2003) The bioequivalence and therapeutic efficacy of
generic versus brand-name psychoactive drugs. Clinical Therapeu-
baseline to the generic period observed in LTG is also
noteworthy. In patients who stayed with the generic, an
Crawford P, Hall WW, Chappell B, Collings J, Stewart A. (1996) Generic
absolute dosage increase of +6.2% (p < 0.0001) was ob-
prescribing for epilepsy: is it safe? Seizure 5:1–5.
Crawford P, Feely M, Guberman A, Kramer G. (2006) Are there potential
served. This suggests that bioavailability of the generic
problems with generic substitution of antiepileptic drugs? A review
product may be decreased relative to the branded formu-
of issues. Seizure 15:165–176.
lation, and a higher dose of the generic compound may
Feely M, Crawford P, Kramer G, Guberman A. (2005) Risk manage-
ment in epilepsy: generic substitution and continuity of supply. The
be needed to maintain therapeutic efficacy. In a regression
European Journal of Hospital Pharmacy Science 11:83–87.
analysis, we found a significant initial dose increment of
Gilman JT, Alvarez LA, Duchowny M. (1993) Carbamazepine toxicity
15.4 mg/day and a trend increase of 0.43 mg/day for ev-
resulting from generic substitution. Neurology 43:2696–2697.
Guberman A, Corman C. (200) Generic substitution for brand name
ery month during the following 3 years. In other words,
antiepileptic drugs: a survey. The Canadian Journal of Neurological
an increase in generic LTG dosage was observed from the
moment of generic entry, and this dose escalation persisted
Jain KK. (1993) Investigation and management of loss of efficacy of an
antiepileptic medication using carbamazepine as an example. Jour-
through the end of the study period. This increased dosage
nal of the Royal Society of Medicine 86:133–136.
requirement in patients receiving generic LTG, based on
Jobst BC, Holmes GL. (2004) Prescribing antiepileptic drugs: should
our regression results, could also factor into significant
patients be switched on the basis of cost? CNS Drugs 18:617–628.
MacDonald JT. (1987) Breakthrough seizure following substitution
of Depakene capsules (Abbott) with a generic product. Neurology
As a study based on a drug-claims database, the extent to
which firm conclusions can be drawn is limited by several
Sander JW. (2004) The use of antiepileptic drugs: principles and practice. Epilepsia 45(suppl 6):28–34.
factors. First, we did not have access to information on pa-
Tyrer JH, Eadie MJ, Sutherland JM, Hooper WD. (1970) Outbreak of
tient diagnosis or medical history, which prevented further
anticonvulsant intoxication in an Australian city. British Medical
investigation into the factors that could have influenced
Welty TE, Pickering PR, Hale BC, Arazi R. (1992) Loss of seizure control
switchback activity, both overall and within categories of
associated with generic substitution of carbamazepine. Annals of
mono- and polytherapy patients. Although the second part
Pharmacotherapeutics 26:775–777.
of this study aimed to investigate the clinical effects of
Wilner AN. (2004) Therapeutic equivalency of generic antiepileptic
drugs: results of a survey. Epilepsy & Behavior 5:995–998.
generic substitution of Lamictal with epilepsy patients,
Wyllie E, Pippenger CE, Rothner AD. (1987) Increased seizure fre-
other users of AEDs for conditions such as bipolar disor-
quency with generic primidone. JAMA 258:1216–1217.
PrEoPErativE PatiEnt instructions For skin surgEry You are scheduled to have excision of a skin lesion in our office using local anesthesia – the same type used in a dental office. You will be able to drive to and from our office unless you have taken sedative medications around the time of the procedure. The following instruc-tions will help to answer any other questions you may h
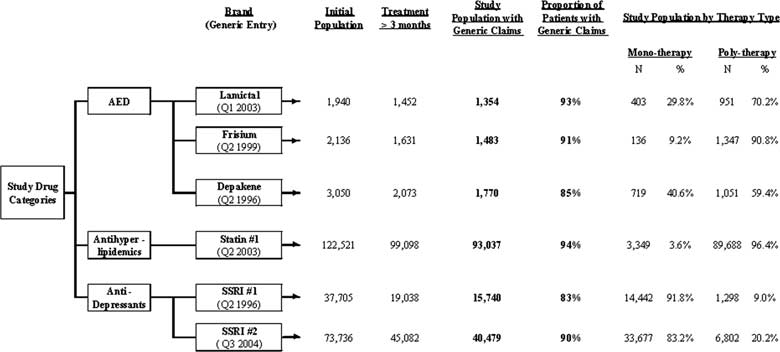 FIG. 1. Patient disposition. SSRI, selective serotonin reuptake inhibitor.
FIG. 1. Patient disposition. SSRI, selective serotonin reuptake inhibitor.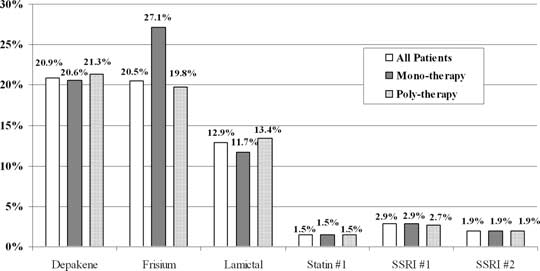 ADVERSE OUTCOMES WITH GENERIC SWITCHING TO LAMOTRIGINE
TABLE 1. Baseline characteristics of study populations
ADVERSE OUTCOMES WITH GENERIC SWITCHING TO LAMOTRIGINE
TABLE 1. Baseline characteristics of study populations