Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
Eprints.nirt.res.in
Non-fermenting Gram Negative Bacilli Associated withAcute Respiratory Infections in Children in Madras
by C. N. Paramasivan, K. Sivadasan, Manjula Datta, R. S. Vallishayee and R. Prabhakar
Tuberculosis Research Centre, Indian Council of Medical Research, Madras 600031, IndiaNon-fermenting Gram negative bacilli (NFGNB) were isolated as the most predominant organism from children suffering from acute respiratory illness (ARI) and accounted for 40 out of 151 children reported in the study. Five of the NFGNB were isolated in pure culture and all of them were from children having lower respiratory infection. The isolation of NFGNB was higher when the duration of illness exceeded 7 days (44 per cent) as compared to 22 per cent with less than 7 days duration (P= 0.03). Detailed identifi- cation studies on 61 isolates of NFGNB showed that 56 (92 per cent) of them belonged to Pseudomonas pseudoalkaligenes alkaligenes group. Four strains were identified as Ps. pseudomallei group and one as Ps. stutzeri. The majority of the NFGNB isolates showed multidrug resistance. Introduction
blood agar, and Mac Conkey agar (MA) plates. Thenon-lactose fermenting colonies on MA were further
Till recently non-fermenting Gram negative bacilli
tested for fermentation of mannitol, lactose, sucrose,
(NFGNB) other than Pseudomonas aeruginosa have
and glucose in peptone water base. Those isolates
been considered as either saprophytes or commensals.
which failed to ferment any of the sugars were
The increasing frequency of isolation of these
regarded as NFGNB and taken for further identifica-
NFGNB1-4 in different clinical conditions has led to
tion. Only those clinical specimens which yielded
a re-evaluation of their role as probable human path-
moderate (21-79 colonies) or heavy ( > 80 colonies)
ogens, and necessitated their identification and classi-
growth of NFGNB were subjected for detailed identi-
fication. The following is a report on the incidence,
probable significance, and sensitivities to antibioticsof the NFGNB isolated from children suffering fromacute respiratory infections (ARI) in Madras. IdentificationThe NFGNB were identified by Gram stain, motility,growth at 4°C and 42°C pigment production, penicil-
Materials and Methods
lin susceptibility and other biochemical reac-
tions. 1, 2, 4-6 The biochemical reactions employed
Throat swabs, laryngeal swabs, nasal swabs, and
were hydrogen sulphide and indole production,
nasal secretions were obtained from children below 6
production of acid from 10 per cent solutions of glu-
years of age suffering from ARI and attending the
cose, lactose, and mannitol in ammonium salt solu-
outpatient department of the Institute of Child
tions; production of urease, arginine decarboxylase,
Health and Hospital for Children, Egmore, Madras.
gelatinase, phenylalanine deaminase, catalase, and
From October 1985 to March 1986, 151 children with
oxidase; utilization of citrate and malonate; oxi-
dation/fermentation (O/F) of glucose, lactose, malt-ose, and xylose; nitrate reduction, nitrite reduction
The specimens were inoculated on to chocolate agar,
Acknowledgements In vitro antibiotic susceptibility test was done on
The authors are grateful to the Director, Institute of Child
Muller-Hinton agar by the disc diffusion method.’
Health and Hospital for Children, Egmore, Madras, for pro-
The drugs used were penicillin (10 units), strepto-
viding facilities and help for conducting this study. The
mycin (10 µg), erythromycin (15 µg), chloramphenicol
authors also thank Mr P. G. Gopi for statistical assistance,
(30 µg), tetracycline (30 µg), cephalosporin (30 µg),
Mr G. K. Loganathan for technical assistance and Mr B.
kanamycin (30 µg), ampicillin (10 µg), gentamicin
(10 µg), colistin (10 µg), and cotrimoxazole (25 µg).
Correspondence: Dr C. N. Paramasivan.
All the drugs tested in this study were obtained from
tract. Five patients yielded NFGNB in pure culture
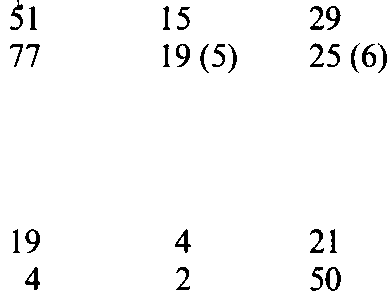
Isolation of NFGNB according to clinical diagnosis
and all of them were suffering from LRI. On fiveoccasions NFGNB were found associated with other
bacteria incriminated in ARI. In two patients it was
found mixed with Klebsiella pneumoniae, in another
two with Haemophilus influenzae, and in one with βhaemolytic streptococci and H. influenzae.
Of the 77 NFGNB isolated, complete characteriza-
tion was done for 61 isolates. All these were oxidase
positive, ruling out the genus Acinetobacter. Since all
these were resistant to penicillin, they may not belong
to the genus Moraxella either. As all of them were
non-pigment producers, pigment-producing organ-
isms such as Chromobacterium violaceum, Pseudo-monas aeruginosa, Ps. fluorescens and Ps. putida were
also ruled out. Based on the biochemical tests men-tioned earlier, 56 (92 per cent) strains of NFGNB
Figures in parenthesis indicate pure growth.
belonged to Pseudomonas pseudoalkaligenes alkali-genes group. Four strains were identified as Pseudo-monas pseudomallei group and one strain as Ps. stutzeri.
The pattern of sensitivity to antibiotics in these
NFGNB isolates is presented in Table 3. All of them
I s o l a t i o n o f N F G N B a c c o r d i n g t o
were resistant to penicillin and cephalosporin. A
majority of them showed resistance to streptomycin,erythromycin, and ampicillin followed by gentamicin.
Approximately 60 per cent of them were sensitive to
chloramphenicol and tetracycline and colistin. Of all
the drugs tested, cotrimoxazole was found to be mosteffective, 90 per cent of the isolates being sensitive fol-
lowed by Kanamycin (77 per cent). On the whole, the
NFGNB isolates showed lowest resistance to colistin(2 per cent), when the moderately sensitive strains (35
per cent) were considered as sensitive along with thehighly sensitive strains (63 per cent). Discussion
In all, 77 strains of NFGNB were isolated from 40 (26per cent) of the 151 children included in the study.
In the present study, out of 151 children with ARI, 40
The number of NFGNB isolated according to the
(26 per cent) yielded NFGNB. This is a significant
clinical diagnosis and duration of illness are shown in
finding considering the fact that other commonly
Tables 1 and 2, respectively. The isolation rates of
incriminated respiratory pathogens like Haemophilus
NFGNB in upper respiratory tract infection (URI)
influenzae and β -haemolytic streptococci were isolated
and lower respiratory tract infection (LRI) were simi-
from only 13 and 11 per cent of the children, respect-
lar, being 29 and 24 per cent, respectively. Also, it is
ively. NFGNB as pure culture was obtained from five
seen from Table 2 that the isolation was maximum
children, all with LRI. Only on five occasions
when the duration of illness exceeded 7 days. The age
NFGNB were found mixed with other potential path-
adjusted isolation rate was 44 per cent in children
like Klebsiella pneumoniae, Haemophilus
with a duration of illness of more than 7 days as com-
influenzae, and β -haemolytic streptococci.
pared to 22 per cent in children with a duration of ill-
A large number of species of NFGNB are known to
ness of 1-7 days (P=0.03). In this study, the other
exist and many of them have been isolated from clin-
organisms isolated according to the order of fre-
ical material3 In the study reported here, the great
quency were Haemophilus influenzae (13 per cent), β−
majority (92 per cent) of the NFGNB isolates
haemolytic streptococci (11 per cent), Klebsiella pneu-
belonged to Ps. pseudoalkaligenes alkaligenes groups. moniae (7 per cent), Pneumococcus (3 per cent), and
Four strains were identified as Ps. pseudomallei
coagulase positive Staphylococcus aureus (1 per cent).
group. As this is the first report from India describing
In most of the patients, the NFGNB were isolated
the isolation of NFGNB from children with ARI,
along with other commensal flora of the respiratory
comparison of the results from the present study with
Antibiotic susceptibility pattern of 60 isolates of NFGNB
Ery. Chl. Tet. Cep. Kan. Amp. Gen. Col. Cot.
that from other Indian reports is not possible. How-
References
ever, Pedersen8 in his review on NFGNB associated
Pickett MJ, Pedersen MM. Non-fermenting bacilli asso-
with man has mentioned that nearly 60 per cent of the
ciated with man II. Detection and identification. Am J
isolates of Ps. pseudoalkaligenes obtained from USA
were from sputum. Ps. pseudamallei group has
2. Bhujwala RA. Laboratory manual on non-fermentative
already been described as a possible respiratory path-
gram negative bacilli (Non-fermenters). A guide to iden-
ogen in a recent review by Levison and Kaye.9
tification. New Delhi: Indian Association of Medical
As regards the aetiopathogenic role of NGFNB in
ARI, it is at present of uncertain significance. So far it
Misra B, Bhujwala RA, Shrinivas. Non-fermenters in
has been believed that the NFGNB in general are
human infection. Ind J Med Res 1986; 83: 561-6.
either free-living saprophytes or commensals. How-
4. Snell JJS. The distribution and identification of non-
fermenting bacteria. PHLS monograph series No. 4.
ever, recently there have been reports about their
emergence as secondary or opportunistic pathogens
5. Parker MT. Pseudomonas. In Topley and Wilsons Prin-
in human disease process. 3, 10 When the NFGNB are
ciples of bacteriology, virology and immunity. In Wilson
present in large numbers, it is quite likely that their
G, Miles A, and Parker MT (eds), 7th edn., Vol. 2.
endotoxin content itself may have some deleterious
effect on the host.10 Even the established respiratory
6. Collins CH, Lyne PM. Microbiological methods, 5th
pathogens like Haemophilus influenzae, β -haemolyticstreptococci, pneumonococcus, and some members of
7. Bauer AW, Kirby WMM, Sherries JC, Turk M. Anti-
enterobacteriaceae, reside in the respiratory tract of
biotic susceptibility testing by a standardised single discmethod. Am J Clin Pathol 1966; 45: 493-6.
healthy individuals as commensals on occasions. The
8. Pedersen MM, Marso E, Pickett MJ. Non-fermentative
exact role of these potential pathogens in the primary
bacilli associated with man. III Pathogenicity and anti-
aetiology of ARI is not clear. Viruses probably act as
biotic susceptibility. Am J Clin Pathol 1970; 54: 178-92.
initiators of respiratory infections and predispose the
9. Levison ME, Kaye D. Pneumonia caused by gram-
bacteria to invade and establish themselves.11-12 The
negative bacilli: an overview. Rev Infect Dis 1985;
precise mechanism is still uncertain, but, transient
immunosuppression caused by viruses,13 destruction
10. Cruickshank R, Duguid JP, Manion BP, Swain RHA.
of the integrity of the respiratory epithelium,14 and
Medical microbiology, 12th edn, Vol. II. New York:
increased adherence of bacteria to the cells infected
11. Sellers TF, Schulman J, Bouvier C, Mccune R, Kil-
with viruses15 have been postulated. In this context,
bourne ED. The influence of influenza virus infection on
the isolation of NFGNB in an appreciable proportion
exogenous staphylococcal and endogenous murine bac-
of children with ARI gains importance.
terial infection of the bronchopulmonary tissues of mice.
The pattern of sensitivity to antibiotics show that a
very high proportion of the strains were sensitive to
12. Jakab CJ, Dick EC. Synergistic effect in viral-bacterial
colistin (98 per cent), cotrimoxazole (90 per cent), and
infection. Combined infection of the murine respiratory
kanamycin (77 per cent). Approximately 60 per cent
tract with sendai virus and Pasteurella pneumotropica.
of them were sensitive to chloramphenicol and tetra-
cyclin. Majority of the strains showed multidrug
13. Woodruff JE, Woodruff JJ. Viral immunology and
immunopathology. London: Academic Press, 1975.
resistance. This multidrug resistance will be of im-
14. Mims CA, White DO. Viral pathogenesis and immuno-
portance should these organisms be shown to have
logy. London: Blackwell Scientific Publication, 1984.
any role in the aetiopathogenesis of ARI in children.
15. Sanford BA, Skelokov A, Ramsay MA. Bacterial adher-
More studies pertaining to the biological properties of
ence to virus infected cells: a cell culture model of bacter-
NFGNB are necessary to elucidate this.
ial superinfection. J Infect Dis 1978; 137: 176-81.
Israeli women living in the UK - challenges to identity and Yasmin Fulder-Heyd and Dr Deborah Rafalin The recent rapid growth of immigration and mobility has elicited a wide discussion in the current psychological literature.1 Such situations often involve threats to identity,2 and raise some basic questions: what are the important dimensions of our identity which we attempt to preserve, and
Après 6 ans de procédure, on admet que l’accès aux soins n’est pas garanti au pays Cas 182 / 30.08.2012 « Louise », née en 1950, souffre du VIH et d’épilepsie. Elle essuie trois refus de l et voit ses deux recours au rejetés avant que celui-ci ne reconnaisse, après 6 ans de procédure, qu’elle n’aura pas accès aux soins nécessaires à sa survie en cas de renv

 tract. Five patients yielded NFGNB in pure culture
Isolation of NFGNB according to clinical diagnosis
and all of them were suffering from LRI. On fiveoccasions NFGNB were found associated with other
bacteria incriminated in ARI. In two patients it was
found mixed with Klebsiella pneumoniae, in another
two with Haemophilus influenzae, and in one with βhaemolytic streptococci and H. influenzae.
Of the 77 NFGNB isolated, complete characteriza-
tion was done for 61 isolates. All these were oxidase
positive, ruling out the genus Acinetobacter. Since all
these were resistant to penicillin, they may not belong
to the genus Moraxella either. As all of them were
non-pigment producers, pigment-producing organ-
isms such as Chromobacterium violaceum, Pseudo-monas aeruginosa, Ps. fluorescens and Ps. putida were
also ruled out. Based on the biochemical tests men-tioned earlier, 56 (92 per cent) strains of NFGNB
Figures in parenthesis indicate pure growth.
tract. Five patients yielded NFGNB in pure culture
Isolation of NFGNB according to clinical diagnosis
and all of them were suffering from LRI. On fiveoccasions NFGNB were found associated with other
bacteria incriminated in ARI. In two patients it was
found mixed with Klebsiella pneumoniae, in another
two with Haemophilus influenzae, and in one with βhaemolytic streptococci and H. influenzae.
Of the 77 NFGNB isolated, complete characteriza-
tion was done for 61 isolates. All these were oxidase
positive, ruling out the genus Acinetobacter. Since all
these were resistant to penicillin, they may not belong
to the genus Moraxella either. As all of them were
non-pigment producers, pigment-producing organ-
isms such as Chromobacterium violaceum, Pseudo-monas aeruginosa, Ps. fluorescens and Ps. putida were
also ruled out. Based on the biochemical tests men-tioned earlier, 56 (92 per cent) strains of NFGNB
Figures in parenthesis indicate pure growth.