Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
101096 effect of amlodipine on morbidity and
E F F E C T O F A M LO D I P I N E O N M O R B I D I T Y A N D M O RTA L I T Y I N S EV E R E C H RO N I C H E A RT FA I LU R E EFFECT OF AMLODIPINE ON MORBIDITY AND MORTALITY IN SEVERE CHRONIC HEART FAILURE
MILTON PACKER, M.D., CHRISTOPHER M. O’CONNOR, M.D., JALAL K. GHALI, M.D., MILTON L. PRESSLER, M.D.,
PETER E. CARSON, M.D., ROBERT N. BELKIN, M.D., ALAN B. MILLER, M.D., GERALD W. NEUBERG, M.D.,
DAVID FRID, M.D., JOHN H. WERTHEIMER, M.D., ANNE B. CROPP, PHARM.D., AND DAVID L. DEMETS, PH.D.,
FOR THE PROSPECTIVE RANDOMIZED AMLODIPINE SURVIVAL EVALUATION STUDY GROUP*
ABSTRACT
use.2,5,6 As a result, physicians have been advised to
Background
avoid the use of calcium-channel blockers in patients
cium-channel blockers increase morbidity and mor-
with heart failure, even if these drugs are being con-
tality in patients with chronic heart failure. We studied
sidered for the treatment of coexisting angina or hy-
the effect of a new calcium-channel blocker, amlo-
dipine, in patients with severe chronic heart failure.
It is not clear, however, whether all calcium-channel
Methods
blockers have deleterious effects in patients with heart
severe chronic heart failure and ejection fractions of
failure. In two controlled trials, amlodipine did not
less than 30 percent to double-blind treatment with
adversely affect the clinical status of patients; in fact,
either placebo (582 patients) or amlodipine (571 pa-
the drug reduced symptoms and improved exercise
tients) for 6 to 33 months, while their usual therapy
was continued. The randomization was stratified on
tolerance. These findings, however, did not allow
the basis of whether patients had ischemic or nonis-
definitive conclusions to be made about the safety of
chemic causes of heart failure. The primary end point
amlodipine in heart failure, since the trials enrolled
of the study was death from any cause and hospital-
fewer than 300 patients, who were treated for only
ization for major cardiovascular events.
8 to 12 weeks, and patients with severe symptoms —
Results
those most likely to have clinical deterioration after
percent of the placebo group and 39 percent of the
treatment with a calcium-channel blocker — were not
amlodipine group, representing a 9 percent reduc-
included.10 To address these limitations, we conduct-
tion in the combined risk of fatal and nonfatal events
ed the Prospective Randomized Amlodipine Survival
with amlodipine (95 percent confidence interval, 24
Evaluation (PRAISE). The primary objective of this
percent reduction to 10 percent increase; Pϭ0.31). A
trial was to assess the long-term effect of amlodipine
total of 38 percent of the patients in the placebogroup died, as compared with 33 percent of those in
on morbidity and mortality among patients with ad-
the amlodipine group, representing a 16 percent re-
duction in the risk of death with amlodipine (95 per-cent confidence interval, 31 percent reduction to
2 percent increase; Pϭ0.07). Among patients with
All patients had dyspnea or fatigue at rest or on minimal exer-
ischemic heart disease, there was no difference
tion (New York Heart Association class IIIB or IV) and a left ven-
between the amlodipine and placebo groups in the
tricular ejection fraction of less than 30 percent despite treatment
occurrence of either end point. In contrast, among pa-
with digoxin, diuretics, and an angiotensin-converting–enzymeinhibitor. Treatment with nitrates was allowed, but other vasodi-
tients with nonischemic cardiomyopathy, amlodipine
lator drugs (e.g., hydralazine) were not permitted. Patients were
reduced the combined risk of fatal and nonfatal
excluded if they had uncorrected primary valvular disease, active
events by 31 percent (Pϭ0.04) and decreased the
myocarditis, or constrictive pericarditis; if they had a history of
risk of death by 46 percent (PϽ0.001).
cardiac arrest or had had sustained ventricular tachycardia or fi-
Conclusions
brillation within the previous year, unstable angina or an acute
vascular morbidity or mortality in patients with se-
myocardial infarction within the previous month, or a cardiac-
vere heart failure. The possibility that amlodipine
revascularization procedure or stroke within the previous three
prolongs survival in patients with nonischemic dilat-ed cardiomyopathy requires further study. (N Engl JMed 1996;335:1107-14.)1996, Massachusetts Medical Society.
From the College of Physicians and Surgeons, Columbia University, New
York (M.P., G.W.N.); Duke University Medical Center, Durham, N.C. (C.M.O., D.F.); Louisiana State University, Shreveport (J.K.G.); KrannertInstitute of Cardiology, Indianapolis (M.L.P.); Washington Veterans Affairs
Medical Center, Washington, D.C. (P.E.C.); New York Medical College,Valhalla (R.N.B.); University of Florida College of Medicine, Jacksonville
calcium-channel blockers may worsen heart
(A.B.M.); Albert Einstein Medical Center, Philadelphia (J.H.W.); Pfizer
failure and increase the risk of death in pa-
Central Research, Groton, Conn. (A.B.C.); and the University of Wiscon-
sin, Madison (D.L.D.). Address reprint requests to Dr. Packer at the Divi-
tients with advanced left ventricular dysfunc-
sion of Circulatory Physiology, Columbia University College of Physicians
tion.1-4 The possibility of such effects has been noted
and Surgeons, 630 W. 168th St., New York, NY 10032.
with most drugs in this class, including many of the
*Members of the Prospective Randomized Amlodipine Survival Evalua-
newer agents that have become available for clinical
tion (PRAISE) study group are listed in the Appendix.
Downloaded from www.nejm.org at UW MADISON on December 04, 2003.
Copyright 1996 Massachusetts Medical Society. All rights reserved.
T h e New E n g l a n d Jo u r n a l o f Me d i c i n e
TABLE 1. PRETREATMENT CHARACTERISTICS OF 1153 PATIENTS WITH CHRONIC HEART FAILURE
ASSIGNED TO TREATMENT WITH AMLODIPINE OR PLACEBO.*
CHARACTERISTIC ALL PATIENTS ISCHEMIC STRATUM NONISCHEMIC STRATUM
*Plus–minus values are means ϮSE. NYHA denotes New York Heart Association, and ACE angiotensin-converting
months; or if they had severe pulmonary, renal, or hepatic disease. End Points
Other criteria for exclusion were systolic blood pressure lower
The primary end point of the study, as stated in the original
than 85 mm Hg or higher than 159 mm Hg; diastolic blood pres-
protocol, was the combined risk of mortality from all causes and
sure higher than 89 mm Hg; a serum creatinine concentration
cardiovascular morbidity. Cardiovascular morbidity was defined
higher than 3.0 mg per deciliter (270 mmol per liter) or a potas-
as hospitalization for at least 24 hours for any of the following
sium concentration lower than 3.5 or higher than 5.5 mmol per
reasons: acute pulmonary edema, severe hypoperfusion, acute my-
liter; or treatment with beta-blockers, calcium-channel blockers,
ocardial infarction, or sustained or hemodynamically destabilizing
or class IC antiarrhythmic agents. Eligible patients had not re-
ventricular tachycardia or fibrillation. The criteria used to evaluate
ceived intravenous diuretics or vasodilators within 24 hours be-
these end points were established at the start of the study, and all
fore enrollment or intravenous positive inotropic agents within 72
events were reviewed by an end-points committee without knowl-
edge of the treatment assignments. The principal secondary end
The protocol was approved by the institutional review boards
point of the study was mortality from all causes. The effect of am-
of all 105 participating institutions. Written informed consent
lodipine on survival was also assessed in subgroups of patients de-
fined on the basis of the following seven prerandomization vari-ables: age, sex, ejection fraction, New York Heart Association class,
Study Design
serum sodium concentration, and the presence or absence of a
After the initial evaluation, patients were randomly assigned (in
history of angina or a history of hypertension. All subgroup anal-
a double-blind fashion) to receive either oral amlodipine or
yses (except that involving age) were prospectively planned in the
matching placebo, in addition to their usual medications. Because
it was expected before the start of the study that amlodipinemight have different effects on patients with different causes of
Statistical Analysis
heart failure, the randomization was stratified according to whether
The sample size for the study was estimated on the basis of the
the cause of left ventricular dysfunction was coronary artery dis-
following assumptions: the event rate (morbidity and mortality
ease or nonischemic dilated cardiomyopathy. The presence of
combined) in the placebo group at one year would be 40 percent;
coronary artery disease was confirmed by coronary arteriography
the risk would be reduced by 25 percent in the amlodipine group;
or suspected on the basis of a history of angina or myocardial in-
10 percent of the patients would withdraw permanently from the
assigned treatment group; and the power to detect a difference
After randomization, patients received an initial dose of 5 mg
between the treatment groups would be 90 percent or higher (al-
of amlodipine or placebo once daily for two weeks; the dose was
pha level of 0.05 by a two-tailed test). Since we recognized that
then increased (if tolerated) to 10 mg of amlodipine or placebo
estimates of the event rate might be inaccurate, the trial was de-
once daily for the remainder of the study. If side effects occurred,
signed to continue until 190 fatal or nonfatal events had occurred
the dose of the study medication could be reduced or discontin-
in the placebo group, with all patients subsequently followed for
ued, but investigators were encouraged to reinstitute treatment at
an additional six months. To reduce the likelihood of false posi-
a later time. If the patient’s condition changed, the physician could
tive results due to repeated interim analyses, we used the Lan–
use any clinically indicated interventions, including adjustments of
DeMets procedure11 with an O’Brien–Fleming boundary,12 which
concomitant treatment with other drugs; however, patients could
requires only the expected number of events and the significance
level to be specified in advance. With this procedure, differences
Downloaded from www.nejm.org at UW MADISON on December 04, 2003.
Copyright 1996 Massachusetts Medical Society. All rights reserved. E F F E C T O F A M LO D I P I N E O N M O R B I D I T Y A N D M O RTA L I T Y I N S EV E R E C H RO N I C H E A RT FA I LU R E
between the two treatment groups at the scheduled end of thetrial were considered significant if the z score was higher than
2.06 (corresponding to nominal PϽ0.0424). The Data and Safe-
ty Monitoring Board periodically reviewed the unblinded resultsand was empowered to recommend early termination of the study
if the treatment effect exceeded the prespecified boundaries.
The base-line characteristics of the two treatment groups were
compared with use of the Wilcoxon test (for continuous and or-
dinal variables) or chi-square test (for categorical variables). Cu-
mulative survival curves for the two groups were constructed by
the Kaplan–Meier method,13 and differences between the curves
were tested for significance with both the log-rank test and a Coxproportional-hazards regression model.14 The survival analyses in-
cluded all patients randomly assigned to a treatment group, and
all deaths were analyzed on the basis of the original group assign-
ments (according to the intention-to-treat principle). Changes in
vital signs and differences in the frequency of adverse reactions
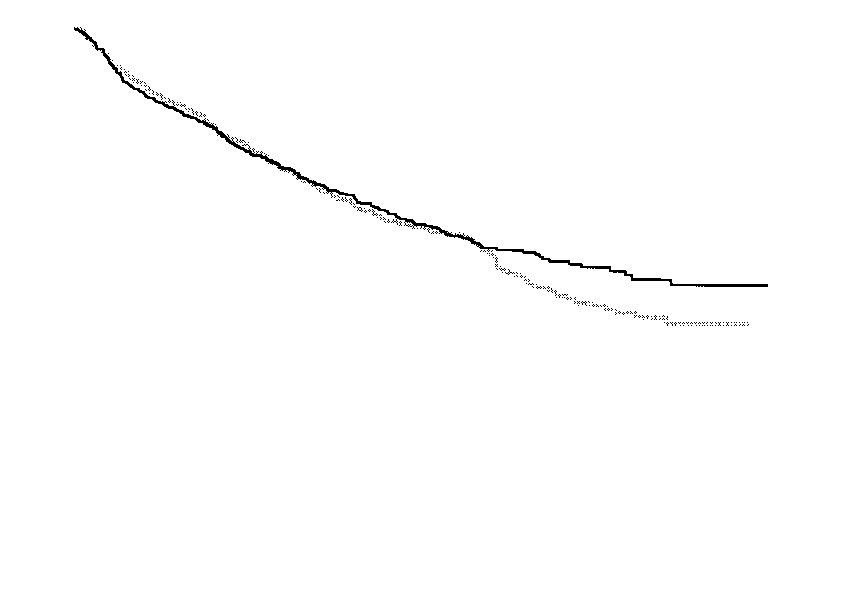
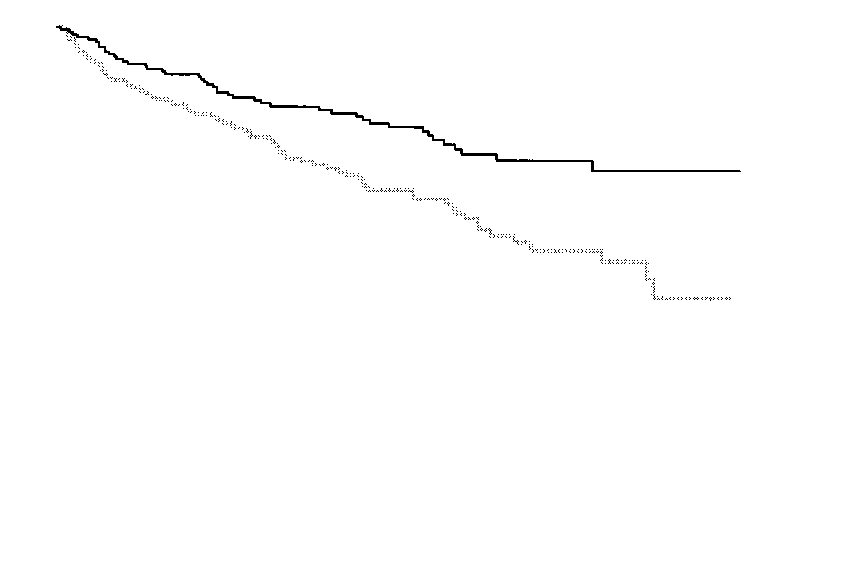
were analyzed by the Wilcoxon or chi-square test, as appropriate. Figure 1. Kaplan–Meier Plots of the Time to the First Primary
Event (Death or Cardiovascular Morbidity) among 571 Patientswith Chronic Heart Failure Receiving Amlodipine and 582 Re-
The PRAISE trial began on March 9, 1992; 1153
patients were enrolled, and follow-up was completed
As compared with the placebo group, the amlodipine group
on December 31, 1994. Of the 732 patients with is-
had a 9 percent lower risk of a primary event (95 percent con-
chemic heart disease, 370 were assigned to placebo
fidence interval, 24 percent lower to 10 percent higher;
and 362 to amlodipine. Of the 421 patients with
nonischemic cardiomyopathy, 212 were assigned toplacebo and 209 to amlodipine.
The two treatment groups were similar with re-
spect to all pretreatment characteristics (Table 1).
One month after randomization, patients were re-
ceiving an average daily dose of 8.8Ϯ0.6 mg of am-
lodipine or 8.9Ϯ0.6 mg of placebo; these doses
were maintained at similar levels throughout the fol-
low-up period. Compliance with the study regimen
(assessed by pill counts) averaged over 90 percent at
all visits. The duration of follow-up ranged from
6 to 33 months (median, 13.8); no patients were
Effect of Amlodipine in the Combined Strata
A primary fatal or nonfatal event occurred in 222
of the 571 patients in the amlodipine group (39
percent) and in 246 of the 582 patients in the pla-
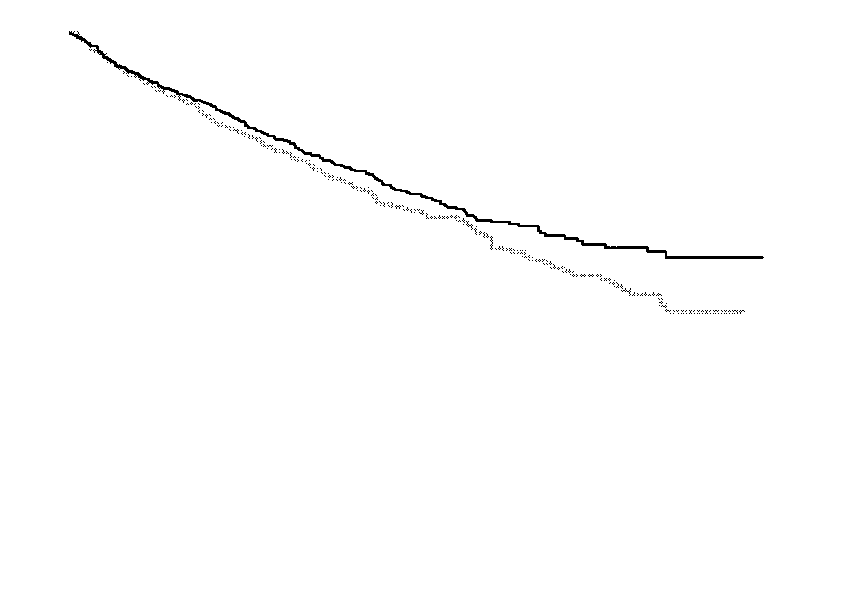
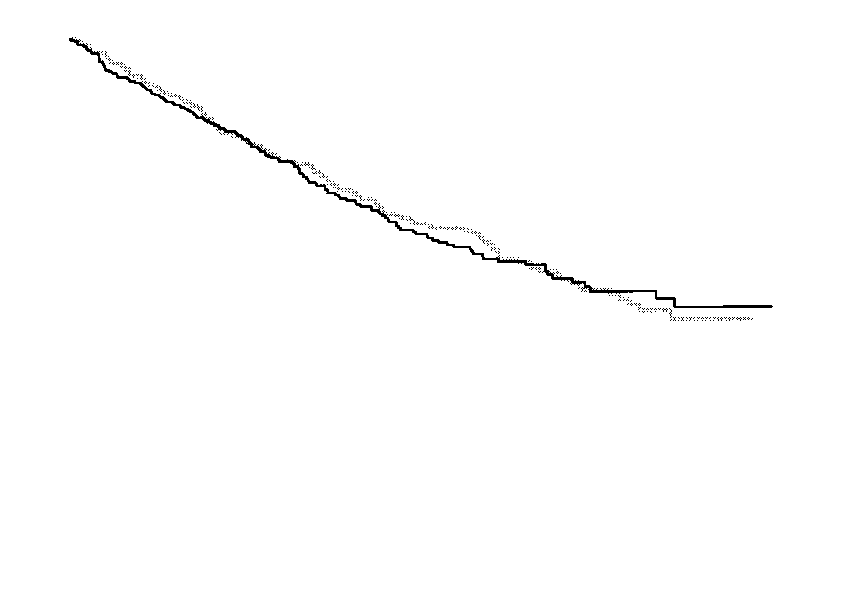
Figure 2. Kaplan–Meier Plots of Cumulative Survival in the Am-
cebo group (42 percent). Cumulative survival curves
are shown in Figure 1. Amlodipine therapy was as-
As compared with the placebo group, the amlodipine group
sociated with a 9 percent reduction in the risk of a
had a 16 percent lower risk of death (95 percent confidence in-
primary fatal or nonfatal event (95 percent confi-
terval, 31 percent lower to 2 percent higher; Pϭ0.07).
dence interval, 24 percent reduction to 10 percentincrease; Pϭ0.31 by the log-rank test). There were
190 deaths from all causes (33 percent) in the am-
effects in those with nonischemic cardiomyopathy,
lodipine group and 223 (38 percent) in the placebo
but this was not the case. There was a significant in-
group. This difference reflected a 16 percent reduc-
teraction between the effect of treatment and the
tion in the risk of death in the amlodipine group (95
cause of heart failure, both for mortality from all
percent confidence interval, 31 percent reduction to
causes (Pϭ0.004) and for the combined end point
2 percent increase; Pϭ0.07) (Fig. 2).
of fatal and nonfatal primary events (Pϭ0.04). As a
result, the effects of amlodipine were evaluated sep-
Effect of Amlodipine in Individual Strata
The results noted above were based on the as-
Among the patients with ischemic heart disease,
sumption that the effects of amlodipine in the pa-
treatment with amlodipine did not affect the com-
tients with ischemic heart disease were similar to the
bined risk of morbidity and mortality or the risk of
Downloaded from www.nejm.org at UW MADISON on December 04, 2003.
Copyright 1996 Massachusetts Medical Society. All rights reserved.
T h e New E n g l a n d Jo u r n a l o f Me d i c i n e
Figure 3. Kaplan–Meier Plots of the Time to the First Primary Event (Panel A) and the Time to Death (Panel B) among Patients with Ischemic Cardiomyopathy in the Amlodipine and Placebo Groups.
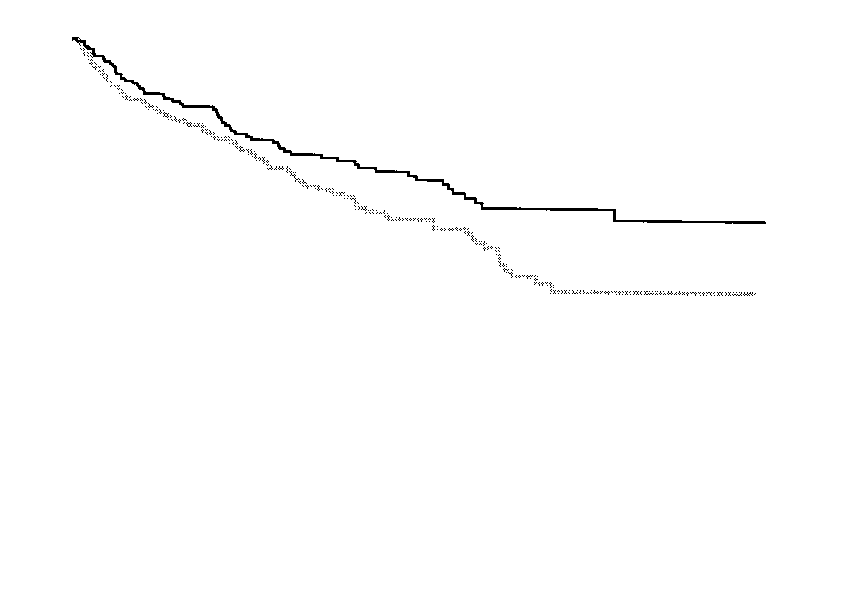
There was no significant difference between the two groups in the risk of primary or secondary events. Figure 4. Kaplan–Meier Plots of the Time to the First Primary Event (Panel A) and the Time to Death (Panel B) among Patients with Nonischemic Dilated Cardiomyopathy in the Amlodipine and Placebo Groups.
As compared with the placebo group, the amlodipine group had a 31 percent lower risk of a primary event (95 percent confidenceinterval, 2 percent to 51 percent lower; Pϭ0.03) and a 45 percent lower risk of death (95 percent confidence interval, 21 percent to63 percent lower; PϽ0.001).
mortality from any cause. Forty-five percent of the
tion; Pϭ0.04). There were 74 deaths from all causes
patients in both treatment groups had a fatal or non-
in the placebo group but only 45 in the amlodipine
fatal event (hazard ratio for the amlodipine group as
group, reflecting a 46 percent reduction in risk in the
compared with the placebo group, 1.04; 95 percent
amlodipine group (95 percent confidence interval, 21
confidence interval, 0.83 to 1.29), and 40 percent
to 63 percent reduction; PϽ0.001). Cumulative sur-
of the patients in both groups died (hazard ratio,
vival curves for the nonischemic stratum are shown in
1.02; 95 percent confidence interval, 0.81 to 1.29).
Cumulative survival curves for the ischemic stratum
The fatal and nonfatal primary events that oc-
curred in the two treatment groups are shown in Ta-
In contrast, treatment with amlodipine reduced the
ble 2 for all patients and for those in the two strata.
frequency of primary and secondary events in patientswith nonischemic dilated cardiomyopathy. There were
Effect of Amlodipine in Specific Subgroups
78 fatal or nonfatal events in the placebo group but
To determine whether amlodipine has an adverse
only 58 in the amlodipine group, reflecting a 31 per-
effect in some patients with heart failure, the influ-
cent reduction in risk in the amlodipine group (95
ence of treatment on mortality was examined in sub-
percent confidence interval, 2 to 51 percent reduc-
groups defined on the basis of pretreatment charac-
Downloaded from www.nejm.org at UW MADISON on December 04, 2003.
Copyright 1996 Massachusetts Medical Society. All rights reserved. E F F E C T O F A M LO D I P I N E O N M O R B I D I T Y A N D M O RTA L I T Y I N S EV E R E C H RO N I C H E A RT FA I LU R E TABLE 2. FREQUENCY OF FATAL AND NONFATAL PRIMARY EVENTS IN ALL PATIENTS
AND IN THE ISCHEMIC AND NONISCHEMIC STRATA.*
PRIMARY EVENT ALL PATIENTS ISCHEMIC STRATUM NONISCHEMIC STRATUM
*Fatal primary events include only the deaths considered by the end-points committee to be primary
end points and do not include the deaths that followed the occurrence of a nonfatal primary event.
teristics. The point estimates for the hazard ratios(with 95 percent confidence intervals) are shown in
TABLE 3. EFFECT OF TREATMENT ON MORTALITY, ACCORDING TO
Table 3. For all characteristics except the presence
or absence of angina, the point estimates for thetreatment effect within each subgroup were similar
AMLODIPINE HAZARD RATIO†
to those for the overall study group. Amlodipine
CHARACTERISTIC (N؍582) (N؍571)
did not have an adverse effect on survival in any of
the subgroups. The drug was associated with a fa-
vorable effect on survival in patients without angina
(Pϭ0.002 for the comparison with the patients
with angina). This finding is consistent with the risk
reduction noted among patients with nonischemic
Safety and Adverse Reactions
In both treatment groups, there were only minor
changes in vital signs. After three months, systolic
and diastolic blood pressure, measured with the pa-
tient standing, was slightly lower (by 2.0 mm Hg)
in the amlodipine group, as compared with base-line
values and the values in the placebo group (PϽ0.01
for both comparisons), but the heart rate did not
Adverse reactions are shown in Table 4, and those
requiring the discontinuation of double-blind ther-
apy are shown in Table 5. Two cardiovascular reac-tions occurred more frequently in the amlodipine
*All deaths were included in the analysis, whether they occurred as a fatal
primary event or after a nonfatal primary event. None of the interactions
group than in the placebo group: peripheral edema
between treatment and characteristic were statistically significant, except
(PϽ0.001) and pulmonary edema (Pϭ0.01). In con-
for the absence or presence of a history of angina. CI denotes confidenceinterval, and NYHA New York Heart Association. Data were not available
trast, two cardiovascular reactions occurred less fre-
on NYHA class for one patient in the amlodipine group and on serum so-
quently in the amlodipine group: uncontrolled hyper-
dium concentration for one patient in the placebo group.
tension (Pϭ0.03) and symptomatic cardiac ischemia
†The hazard ratio is for the risk of death in the amlodipine group as
(angina and chest pain). In the patients with ischemic
heart disease, the risk of angina or chest pain was low-er among those in the amlodipine group (25 percent)than among those in the placebo group (31 percent,Pϭ0.07). The frequency of myocardial infarction in
Downloaded from www.nejm.org at UW MADISON on December 04, 2003.
Copyright 1996 Massachusetts Medical Society. All rights reserved.
T h e New E n g l a n d Jo u r n a l o f Me d i c i n e
Although pulmonary edema occurred more fre-
TABLE 4. ADVERSE REACTIONS IN THE TWO TREATMENT GROUPS.
quently in the amlodipine group than in the placebogroup (Tables 2 and 4), other events reflecting the
AMLODIPINE
clinical progression of heart failure (e.g., life-threat-
ADVERSE REACTION (N؍582) (N؍571)
ening arrhythmias and death) occurred less fre-
quently in the amlodipine group (Table 2). The fre-quency of worsening heart failure was similar in the
two groups (Table 4), as was the frequency of hos-
pitalization for worsening heart failure (36 percent
in the amlodipine group and 39 percent in the pla-
With respect to noncardiovascular side effects, the
amlodipine group had a lower frequency of liver and
biliary disorders than the placebo group (Pϭ0.01)
but a higher frequency of worsening renal function
first six months, values for serum bilirubin and liver
enzymes were higher in the placebo group (PϽ0.05),
but the two groups had similar values for blood urea
DISCUSSION
The present study demonstrates that amlodipine
does not adversely affect the natural history of
chronic heart failure, even in patients with the most
advanced disease. Administration of the drug for
6 to 33 months in patients who had symptoms atrest or on minimal exertion and an average left ven-
*PϽ0.05 for the comparison with the placebo group.
tricular ejection fraction of only 21 percent was notassociated with an increased frequency of worseningheart failure, myocardial infarction, or life-threaten-ing arrhythmias or an increased risk of hospitaliza-tion for serious cardiovascular events. In addition,
TABLE 5. REASONS FOR DISCONTINUATION OF STUDY
unlike several other vasodilator drugs,15 amlodipinedid not increase the risk of death. In fact, the mor-tality rate was 16 percent lower in the amlodipine
PLACEBO AMLODIPINE
worsening angina and uncontrolled hypertension
were reported less frequently in the patients treated
with amlodipine. Taken together, these observations
indicate that amlodipine can be used with relative
safety in patients with severe heart failure — an im-
portant finding, since angina and hypertension can
be difficult to treat in patients with left ventricular
The results with amlodipine differ from those re-
ported in trials of other calcium-channel blockers in
patients with chronic heart failure. Short-term treat-
ment with verapamil, nifedipine, and diltiazem has
produced clinical deterioration,10,17-19 and long-term
therapy with these drugs has increased the risk of
worsening heart failure, myocardial infarction, and
death in patients with left ventricular dysfunction.1,3,4,20
These adverse reactions have been attributed to the
propensity of the drugs to depress cardiac contractil-
ity and activate endogenous neurohormonal sys-
tems,21 but the importance of these mechanisms re-
mains uncertain, since the deleterious actions may be
Downloaded from www.nejm.org at UW MADISON on December 04, 2003.
Copyright 1996 Massachusetts Medical Society. All rights reserved. E F F E C T O F A M LO D I P I N E O N M O R B I D I T Y A N D M O RTA L I T Y I N S EV E R E C H RO N I C H E A RT FA I LU R E
minimized by the use of sustained-release formula-
bidity and mortality in patients with severe chronic
tions or vasoselective agents (e.g., nicardipine, nisol-
dipine, or felodipine). Neither approach, however, has
In the present study, the cause of heart failure was
prevented the development of cardiovascular compli-
determined not by coronary arteriography but by the
cations. Immediate-release formulations of nicardi-
clinical judgment of the investigators. Hence, it is
pine22 and nisoldipine2 have resulted in worsening
possible that some patients with silent coronary artery
heart failure, as have sustained-release formulations of
disease were included in the nonischemic stratum and
some with angina but normal coronary arteries were
An intriguing finding of the present study was
included in the ischemic stratum. From a clinical
that amlodipine reduced both mortality from all caus-
viewpoint, such errors may raise doubts about our
es and the combined risk of fatal and nonfatal events
finding that amlodipine has a beneficial effect in pa-
in patients with nonischemic dilated cardiomyop-
tients with nonischemic cardiomyopathy. From a sta-
athy. Although this benefit was seen only in a sub-
tistical viewpoint, however, such misclassifications
group of patients, it is likely that it reflects a true
would be expected to weaken (rather than strength-
effect of amlodipine, since the randomization proce-
en) the ability to detect a stratum-specific treatment
dure was stratified according to the cause of heart
effect and are thus unlikely to account for the effect
failure and a significant difference between the is-
we observed. Furthermore, if the benefits of amlo-
chemic and nonischemic strata was noted for both
dipine in patients with nonischemic disease are con-
the primary and secondary end points of the study.
firmed by subsequent studies, our clinical (rather than
Yet, some caution is warranted, since our a priori ex-
angiographic) approach will make treatment recom-
pectation was that amlodipine would be more ben-
mendations readily applicable to most patients.
eficial in patients with ischemic heart disease — a
In conclusion, this trial establishes the safety of
hypothesis that was not confirmed. Furthermore, the
amlodipine for the treatment of angina or hyperten-
mechanism by which amlodipine may prolong sur-
sion in patients with advanced left ventricular dys-
vival remains unknown. Nevertheless, other trials of
function. Should the drug be used for the treatment
drugs in patients with heart failure have reported a
of heart failure in patients without these associated
treatment effect confined to those with nonischemic
cardiovascular conditions? Although amlodipine may
cardiomyopathy,24,25 suggesting that this condition
reduce the risk of death in patients with nonische-
may be uniquely responsive to pharmacologic inter-
mic dilated cardiomyopathy, we believe that such an
effect requires confirmation in a second trial. That
If amlodipine has favorable effects in patients with
study, known as PRAISE-2, is now in progress.
heart failure, why was the risk of pulmonary edemahigher with the drug than with placebo? Although
Supported by a grant from Pfizer Central Research.
this finding might suggest that amlodipine can exac-erbate heart failure, such a conclusion would be in-
APPENDIX
consistent with other observations. First, amlodipine
Data and Safety Monitoring Board: R.J. Cody (chair), G. Fran-
was associated with a decreased risk of most mani-
cis, F. Harrell, B. Massie, and M. Pfeffer. Statistical analysis:
festations of disease progression (life-threatening ar-
S. Anderson. Study operations and monitoring: D. Rendall,G. Wagner, and R. Califf. Clinical monitors: A. Fairbank, K. Fly,
rhythmias and death) (Table 2). Second, the risk of
D. Gardiner, J. Gill, J. Glaze, M. Lambert, K. Minor, L. Robin-
worsening heart failure was similar in the placebo
son, L. Russ, L. Sears, K. Soileau, and L. Vesce. Members of the
and amlodipine groups (Table 4). Third, pulmonary
PRAISE Study Group:Albuquerque, N.M.: B. Ramo and K. Heim-
edema occurred more frequently in the amlodipine
gartner; Anaheim, Calif.: M. Tonkon and C. Fox; Ann Arbor,Mich.: M. Starling and J. Petrusha; Aurora; Colo.: B. Molk and
group, even among the patients with nonischemic
M. Vogt; Beverly Hills, Calif.: R. Karlsberg and S. Maccioni;
cardiomyopathy, who had the most marked benefits
Biloxi, Miss.: M. Unks and K. Smith; Birmingham, Ala.: T. Paul
from the drug. These observations suggest that the
and T. Sanders; Boston: J. Smith, L. Kilcoyne, R. Goulah, and
occurrence of pulmonary edema in patients treated
K. Fallen; Charleston, W.V.: D. Lilly and D. Curtis; Charlotte,
with amlodipine may not reflect the progression of
N.C.: W. Bennett, K. Simmons, G. Collins, J. Hathaway, R. Stack,and L. Jackson; Chicago: J. Barron, K. Daly, D. Berkson, A. Mer-
heart failure. Calcium-channel blockers can cause
lo, M. Papp, and V. Just; Cincinnati: D. Kereiakes and N. Higby;
pulmonary edema by dilating pulmonary arterioles
Cleveland: R. Hobbs and M. Jarosz; Columbia, S.C.: C. Hassa-
rather than by adversely affecting the heart26-28; in
poyannes and M. Kline; Concord, N.C.: P. Campbell and J. Taylor;
doing so, these drugs interfere with the restraint that
Danbury, Conn.: B. Pollack and J. Kies; Danville, Va.: G. Millerand S. Davis; Dayton, Ohio: G. Collins and R. Mark; Denver:
pulmonary vasoconstriction normally exerts on blood
K. VanBenthuysen and L. Manne; Durham, N.C.: E. Hampton
flow into the lungs and the transudation of fluid
and K. Hansley; East Lansing, Mich.: P. Willis and H. Boichot;
into alveoli when pulmonary venous pressures are
Falls Church, Va.: J. O’Brien and M. Obeid; Florence, S.C.:
increased.29,30 Fortunately, the risk of pulmonary
J. Kmonicek and J. Shane; Fredericksburg, Va.: R. Vranian and
edema attributable to amlodipine is small (5 per-
D. Louder; Ft. Myers, Fla.: J. Conrad and P. Fowler; Gainesville,Fla.: S. Roark and N. Marquis; Galax, Va.: J. Puma and J. Hold-
cent) (Table 4), so that this risk does not alter our
away; Gilbert, Ariz.: R. Siegel and J. Corwin; Hershey, Pa.: J. Boeh-
finding that the drug has no overall effect on mor-
mer and B. Clemson; Hibbing, Minn.: R. Moyer and S. Walters;
Downloaded from www.nejm.org at UW MADISON on December 04, 2003.
Copyright 1996 Massachusetts Medical Society. All rights reserved.
T h e New E n g l a n d Jo u r n a l o f Me d i c i n e
Indianapolis: J. Moorman-Birt; Jacksonville, Fla.: T. Hilton,
tients with mild to moderate heart failure: UK Study Group. Br Heart J
P. Downing and M. Hudson; La Jolla, Calif.: D. Costello and
R. O’Beso; Lakeland, Fla.: K. Browne and S. Collins; Lancaster,7. Packer M, Kessler PD, Lee WH. Calcium-channel blockade in the man- Pa.: I. Smith and K. Knepper; Las Vegas: J. Bowers, K. Grado,
agement of severe chronic congestive heart failure: a bridge too far. Circu-lation 1987;75:Suppl V:V56-V64.
J. Kaufman, and J. Lysgaard; Lebanon, N.H.: B. Hettleman and
8. Packer M, Nicod P, Khandheria BR, et al. Randomized, multicenter,
C. Carlson; Long Beach, Calif.: D. DeCristofaro and R. Bright;
double-blind, placebo-controlled evaluation of amlodipine in patients with
Los Angeles: U. Elkayam, J. Johnson, R. Davidson, and K. dosRe-
mild-to-moderate heart failure. J Am Coll Cardiol 1991;17:Suppl A:274A.
medios; Louisville, Ky.: M. Denny and L. Gamble; Lynn, Mass.:
M. Motta and M. Criasia; Madison, Wis.: J. Morledge and
9. Smith WB, DeAbate AC, Gollub SB, et al. Beneficial long-term hemo-
C. Shanley; Marrero, La.: C. Unger and P. Ponti; Maywood, Ill.:
dynamic and clinical effects of amlodipine in chronic heart failure: results
M. Silver and C. Keeler; Memphis, Tenn.: F. McGrew and
of a multicenter randomized, double-blind, placebo-controlled, dose-rang-
B. Hamilton; Merritt Island, Fla.: K. Sheikh and T. Hengerer;
ing study. Circulation 1994;90:Suppl:I-603. abstract. 10. Packer M, Lee WH, Medina N, Yushak M, Bernstein JL, Kessler PD. Miami: R. Chahine and L. Laso; Minneapolis: I. Goldenberg and
Prognostic importance of the immediate hemodynamic response to nifed-
K. Scott; Nassau Bay, Tex.: R. Bhalla and T. Hicks; New Orleans:
ipine in patients with severe left ventricular dysfunction. J Am Coll Cardiol
W. Smith, T. McCormack, C. DeAbate, and J. Smith; New York:
C. Galvin; Newport Beach, Calif.: B. Kennelly and D. Mills; Nor-11. Lan KKG, DeMets DL. Discrete sequential boundaries of clinical tri- folk, Va.: W. Old and R. Bariciano; Oak Lawn, Ill.: B. Abramowitz
and D. Kirchbaum; Oklahoma City: C. Bethea, K. Andreatta,
12. O’Brien PC, Fleming TR. A multiple testing procedure for clinical tri-
U. Thadani, and B. Barnett; Omaha, Nebr.: L. DeBoer and
C. Reckling; Pensacola, Fla.: R. Aycock and T. Wilcox; Peoria,13. Kaplan EL, Meier P. Nonparametric estimation from incomplete ob- servations. J Am Stat Assoc 1958;53:457-81. Ill.: A. Chu, T. Ralser, P. Schmidt, and C. Ness; Philadelphia:14. Cox DR. Regression models and life-tables. J R Stat Soc [B] 1972;34:
E. Liedel; Pittsburgh: B. Uretsky, Y. Cannon, A. Ticzon, L. Pre-
dis, M. Geller, and M. Puskar; Portland, Oreg.: D. Dawley, C. Ry-
15. Packer M, Rouleau J-L, Swedberg K, et al. Effect of flosequinan on
erson, W. Ryan, and S. Pollard; Providence, R.I.: S. Sharma and
survival in chronic heart failure: preliminary results of the PROFILE Study.
L. Coulter; Rochester, Minn.: B. Khandheria and S. Eifert-Rain;
Circulation 1993;88:Suppl:I-301. abstract. Sacramento, Calif.: J. Chin and D. Aarons; Salem, Va.: N. Jarmuk-
16. Packer M, Kukin ML. Management of patients with heart failure and
li and T. Thompson; Salt Lake City: A. Barker and E. Doran; San
angina: do coexistent diseases alter the response to cardiovascular drugs?
Antonio, Tex.: B. Mittler and K. Warren; San Diego, Calif.:
J Am Coll Cardiol 1991;17:740-2. 17. Witchitz S, Haiat R, Tarrade T, Chiche P. Accidents cardio-vasculaires
H. Rockman and S. Ueland; Sanford, N.C.: G. O’Donnell and
au cours des traitements par le vérapamil: a propos de 6 observations. Nouv
S. McNamee; Shreveport, La.: B. Sims; South Bend, Ind.: F. Wefald
and D. Edwards; Spokane, Wash.: M. DeWood and J. Priggie;
18. Elkayam U, Weber L, McKay C, Rahimtoola S. Spectrum of acute he- Springfield, Mass.: A. Wiseman and R. Gianelly; St. Petersburg,
modynamic effects of nifedipine in severe congestive heart failure. Am J
Fla.: D. Bramlet and J. Reddinger; Tamarac, Fla.: R. Schneider
and K. Goetz; Tampa, Fla.: P. Alagona, C. Wise, D. Schocken,
19. Packer M, Lee WH, Medina N, Yushak M. Comparative negative ino-
and P. Douglass; Thousand Oaks, Calif.: I. Loh and C. Smith; To-
tropic effects of nifedipine and diltiazem in patients with severe left ven-
ledo, Ohio: T. Fraker and S. Hiris; Toronto: P. Liu and J. Walters;
tricular dysfunction. Circulation 1985;72:Suppl III:III-275. abstract. 20. Ferlinz J, Gallo CT. Responses of patients in heart failure to long-term Tulsa, Okla.: D. Brewer, S. Black, F. McNeer, and B. Smith; Tyler,
oral verapamil administration. Circulation 1984;70:Suppl II:II-305. ab-
Tex.: R. Meese and S. Crispin; Valhalla, N.Y.: A. Kanakaraj; Wash-ington, D.C.: C. Curry, C. Okeakpu, and E. Greenberg; Wichita,21. Packer M. Pathophysiological mechanisms underlying the adverse ef- Kans.: K. Goyle, P. Greuel, J. Galichia, and B. Gonsalves; Wil-
fects of calcium channel-blocking drugs in patients with chronic heart fail-
liamsport, Pa.: J. Burks and N. Kohler; Worcester, Mass.: S. Pezzel-
ure. Circulation 1989;80:Suppl IV:IV-59–IV-67.
la, M. Kirkpatrick, L. Heller, and S. Balcom. 22. Gheorghiade M, Hall V, Goldberg AD, Levine TB, Goldstein S. Long term clinical and neurohormonal effects of nicardipine in patients with se- REFERENCES
vere heart failure on maintenance therapy with angiotensin converting en-zyme inhibitors. J Am Coll Cardiol 1991;17:Suppl A:274A. abstract. 1. Elkayam U, Amin J, Mehra A, Vasquez J, Weber L, Rahimtoola SH. A 23. Mohindra SK, Udeani GO. Long-acting verapamil and heart failure.
prospective, randomized, double-blind, crossover study to compare the ef-
ficacy and safety of chronic nifedipine therapy with that of isosorbide dini-
24. Singh SN, Fletcher RD, Fisher SG, et al. Amiodarone in patients with
trate and their combination in the treatment of chronic congestive heart
congestive heart failure and asymptomatic ventricular arrhythmia. N Engl
failure. Circulation 1990;82:1954-61. 2. Barjon JN, Rouleau J-L, Bichet D, Juneau C, De Champlain J. Chron- 25. CIBIS Investigators and Committees. A randomized trial of b-block-
ic renal and neurohumoral effects of the calcium entry blocker nisol-
ade in heart failure: the Cardiac Insufficiency Bisoprolol Study (CIBIS).
dipine in patients with congestive heart failure. J Am Coll Cardiol 1987;
26. Gillmer DJ, Kark P. Pulmonary oedema precipitated by nifedipine. 3. Goldstein RE, Boccuzzi SJ, Cruess D, Nattel S, Adverse Experience
Committee, Multicenter Diltiazem Postinfarction Research Group. Diltia-
27. Batra AK, Segall PH, Ahmed T. Pulmonary edema with nifedipine in
zem increases late-onset congestive heart failure in postinfarction patients
primary pulmonary hypertension. Respiration 1985;47:161-3.
with early reduction in ejection fraction. Circulation 1991;83:52-60. 28. Yoran C, Glassman E. The paradoxic effect of tolazoline hydrochloride 4. The Multicenter Diltiazem Postinfarction Trial Research Group. The ef-
on pulmonary hypertension of mitral stenosis. Chest 1973;63:843-6.
fect of diltiazem on mortality and reinfarction after myocardial infarction.
29. Semigran MJ, Cockrill BA, Kacmarek R, et al. Hemodynamic effects
of inhaled nitric oxide in heart failure. J Am Coll Cardiol 1994;24:982-8. 5. Tan LB, Murray RG, Littler WA. Felodipine in patients with chronic 30. Haywood GA, Sneddon JF, Bashir Y, Jennison SH, Gray HH,
heart failure: discrepant haemodynamic and clinical effects. Br Heart J
McKenna WJ. Adenosine infusion for the reversal of pulmonary vasocon-
striction in biventricular failure: a good test but a poor therapy. Circulation
6. Littler WA, Sheridan DJ. Placebo controlled trial of felodipine in pa-
Downloaded from www.nejm.org at UW MADISON on December 04, 2003.
Copyright 1996 Massachusetts Medical Society. All rights reserved.
June 1, 2011 Compounded Horse mediCations: LegaL and etHiCaL issues TheHorse.com: Welcome to the webinar! We’ll be starting the live Q&A in just a few minutes. TheHorse.com: Hello everyone, and welcome to our Webinar, Compounded Medications for Horses: Le- gal/Ethical Issues! We’d like to introduce tonight’s presenter, Scott Stanley, PhD, Professor of Equine Analytical C
THE ANTIGUA AND BARBUDA SALES TAX (AMENDMENT) REGULATIONS, 2010 2010, No. The Antigua and Barbuda Sales Tax (Amendment) Regulations, 2010 THE ANTIGUA AND BARBUDA SALES TAX (AMENDMENT) REGULATIONS, 2010 ARRANGEMENT Regulations 1. Short 2. Interpretation 3. Amendment of Schedule 2 4. Amendment of Schedule 3 5. Amendment of Schedule 4 6. Amendment of Schedule 5 The
 E F F E C T O F A M LO D I P I N E O N M O R B I D I T Y A N D M O RTA L I T Y I N S EV E R E C H RO N I C H E A RT FA I LU R E
E F F E C T O F A M LO D I P I N E O N M O R B I D I T Y A N D M O RTA L I T Y I N S EV E R E C H RO N I C H E A RT FA I LU R E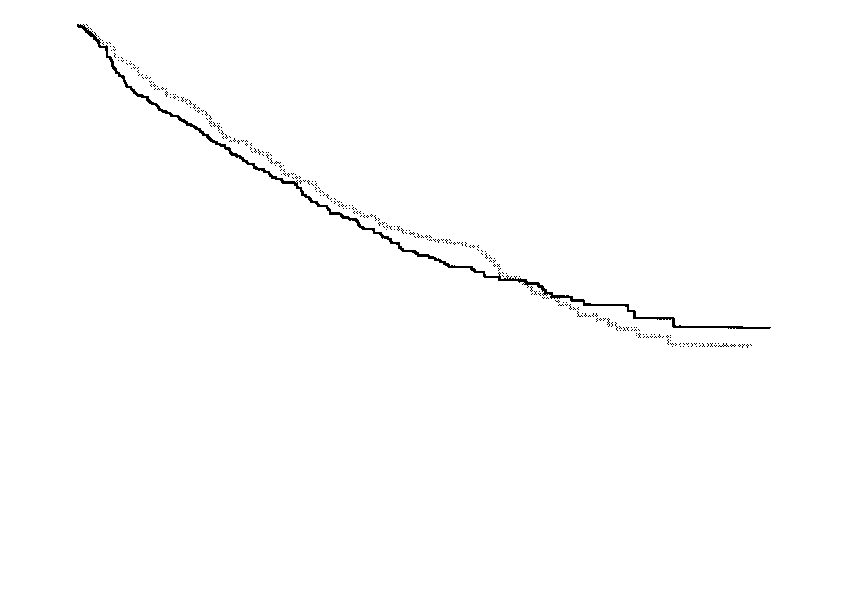
 T h e New E n g l a n d Jo u r n a l o f Me d i c i n e
Figure 3. Kaplan–Meier Plots of the Time to the First Primary Event (Panel A) and the Time to Death (Panel B) among Patients with
T h e New E n g l a n d Jo u r n a l o f Me d i c i n e
Figure 3. Kaplan–Meier Plots of the Time to the First Primary Event (Panel A) and the Time to Death (Panel B) among Patients with