Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
We will further develop the use of organoid epithelial cultures to “read out” microbiome status
Research Portfolio Neuro-immune group Tytgat Institute for Liver and Intestinal Research Contact: GutResearch Academic Medical Center (Room S2-180) Meibergdreef 69-71 1105 BK Amsterdam The Netherlands T: + 31 (0)20 5668163 Pre-clinical models for human diseases 1-models for visceral hyper-perception; (Irritable Bowel Syndrome) 2-models for functional bowel and motility disorders (Postoperative Ileus) 3-models for experimental Colitis; diverse models 4-primary epithelial cultures and epithelial cells lines 5-further relevant assays 1-models for visceral hyper-perception; Irritable Bowel Syndrome (IBS)
Background.
IBS is a functional bowel disorder characterized by abdominal pain or discomfort
associated with changes in bowel habit. Although increased sensitivity to rectal distension (so called visceral hypersensitivity) is considered a possible pathophysiological mechanism1, the exact aetiology of IBS is not known.
The model. Impaired parent-child interactions are considered a possible environmental trigger for
IBS2 and animal models reflecting this trigger may, although they can never fully reflect complex human parent-child interactions, contribute to a better understanding of this disorder. For this reason we use the maternal separation model in rats in which pups are separated from their mothers for 3 hours daily from postnatal days 2 to 14.3 In contrast to nonhandled (NH)-rats, adult maternal separated (MS) rats display an IBS-like phenotype (intestinal barrier dysfunction and visceral hypersensitivity). Importantly, onset depends on rat strain; Long Evans rats only show hypersensitivity after an additional acute stress at adult age while this is not required in Wistar rats. In our group we prefer to work with Long Evans because also in IBS-patients acute stress is an important trigger for symptom generation.4 Results with this model. Using this rat model we were able to show that stress-induced visceral hypersensitivity
depends on the degranulation of mast cells.5, 6 In a translational follow up study with the mast cell stabilizer and histamine-1-receptor (H1R) antagonist ketotifen we confirmed the possible relevance of these cells.7 Ketotifen not only decreased abdominal pain and other IBS symptoms but also improved health related quality of life and increased the threshold of discomfort in hypersensitive patients. Investigations comparing pre- and post-therapy mediator release by submerged rectal biopsies suggested that H1R antagonism was the main molecular mode of action in this trial. Because ketotifen crosses the blood brain barrier we subsequently tested two highly selective and peripherally restricted H1R antagonists in our rat model. Results (unpublished) showed reversal of post stress hypersensitivity by both antagonists and we are now evaluating one of these antagonists in a new clinical trial.
Potential use for research partner. We used the maternal separation model to evaluate pharmacological interventions
capable of reversing post-stress visceral hypersensitivity.5, 6, 8 Importantly, as shown by our mast cell data, results obtained in this model can be translated to IBS.7 Others used it to examine the effect of probiotic interventions9-12 and our own most recent data (unpublished) indicated that other dietary interventions might also proof beneficial. Further, we recently demonstrated that the enhanced susceptibility to stress-induced hypersensitivity observed in maternally separated (F1) rats can be transferred to next generation (F2) animals without further separation protocols (submitted for publication). This is highly relevant because IBS was shown to cluster in families in the absence of clear genetic components. Our data open up possibilities to investigate treatment strategies that may interfere with transfer across generations (e.g. treatment of mothers or children). 2-models for functional bowel and motility disorders; Postoperative Ileus (POI) Background.
POI is characterized by dysmotility of the gastrointestinal tract that occurs after
essentially every abdominal procedure and results in increased patient morbidity and prolonged hospitalisation.13 The costs related to POI have been estimated to amount 1.47 billion dollars annually in the USA, illustrating its large socio-economical impact. Recent evidence obtained in mouse POI models indicated that ileus following bowel manipulation is a biphasic process.13 An acute phase of generalized enteric hypomotility is due to activation of inhibitory neural reflexes.
The model. Specific surgical intestinal manipulations are performed in a routine fashion. Graded
severity of the manipulation is optimized (inspection, severe handling). In vivo motility is measured in life mice in real time.
Results with this model. Preclinical investigations from our own group significantly demonstrated that a
subsequent prolonged phase is mediated by mechanical manipulation-induced inflammation of the intestinal muscularis externa.14-19 This inflammation results in hypomotility of the entire gastrointestinal tract. In our mouse model we showed that manipulation induced mast cell degranulation is an essential step in the induction of this inflammatory process20, 21 and we were able to subsequently translate these results to the human setting.22, 23 Recent results have demonstrated IL-1 activation and receptor triggering is a crucial contributor to inflammation-induced motility disturbance (Stoffels et al, Gastroenterology, under review 2012)
As demonstrated by our translational research in POI, this mouse model provides
1) mechanisms relevant to this iatrogenic condition and 2)pharmacological interventions that may benefit patients. Potential use for Research partner.
The demonstration of dietary components, or pre, or probiotics to relieve post-
operative motility disturbances and enhance post-operative recovery in a clinically relevant model. Recently, the successful tests of dietary polyunsaturated fatty acids (PUFA) in this models model for mouse POI suggesting that dietary intervention strategies can also be evaluated in this model system.24 3-models for experimental Colitis and in vitro approaches on patient intestinal resection material
Background.
The Department of Gastroenterology and Hepatology of the Academic Medical Center in Amsterdam is an expert and referral centre for IBD and has a longstanding tradition of excellent patient care combined with both clinical and fundamental research activities. Since several years now its fundamental IBD-research is bundled in the Tytgat Institute where it is part of the research theme of 3 different principle investigators (GR van den Brink, AA te Velde and WJ de Jonge). The close collaboration between the Tytgat Institute and clinicians of the Gastroenterology department is an important strength of our approach. The models. Routinely used models in our lab are: -DSS colitis -TNBS colitis -CD45RBhigh Tcell transfer colitis (Powrie model) Results with this model
In the Netherlands, but also internationally, the AMC fulfils a leading role in the treatment of IBD. In the past we introduced the concept to treat patients with Crohn’s disease with antibodies against tumor necrosis factor (anti-TNF),25 a breakthrough in the therapy of this disabling disease. Over the years, other novel insights in the pathogenesis and genetics of IBD have been introduced, including the importance of IL-10 as potential treatment. The latter has led to the generation of genetically manipulated lactobacillae producing IL-10 (tested in patients with Crohn´s disease26). At present the clinical IBD group is headed by Prof G. D’Haens who plays a crucial and coordinating role in phase I and II clinical trials evaluating the therapeutic potential of new biologicals. His internationally acclaimed expertise ensures timely ‘bench to bedside’ translation of results obtained in the Tytgat Institute.
At the Tytgat Institute stateof the art in vitro assays and in vivo models (used on a
routine basis) allow us to investigate the role of pathways relevant to the development of IBD. In a large number of publications we not only used conventional mouse models like DSS- and TNBS-colitis but also the CD45RB T cell transfer model that most closely reflects human IBD. These models were used to establish basic mechanisms in IBD as well as pharmacological and dietary intervention strategies (example publications27-32).
Since we have broad access to patient tissues and isolated cells we also validate our
experimental data by immunological phenotyping and activation of mucosal lymphocytes, dendritic cells and macrophages. Data obtained in these in vitro investigations can be correlated with clinical phenotype and genetic profile. Potential use for Research partner.
These models are optimized for testing of pharmaca, biological, or nutritional interventions to relieve the severity of colitis. An in vivo mouse endoscope has been recently set up to be able to perform life imaging of the colitic lesions, and the recovery due to experimental treatment. Human resection material can be processed in MLII environments. All ethical approval is in place for the use of human material in test setting in our lab.
4-primary epithelial cultures and epithelial cells lines Background.
A clear disadvantage of the use of clonal epithelial cell cultures (such as the
commonly used Caco-2 or HT29 cell lines) is the fact that those are usually tumor cell derived and may not represent the full spectrum of specialized epithelial cells. In order to assay the true impact of shifts in metabolic activity of bacteria we have adapted the crypt-organoid culture as described earlier.33-35
The model. To allow study of the relevance of for instance Paneth cell function and antimicrobial
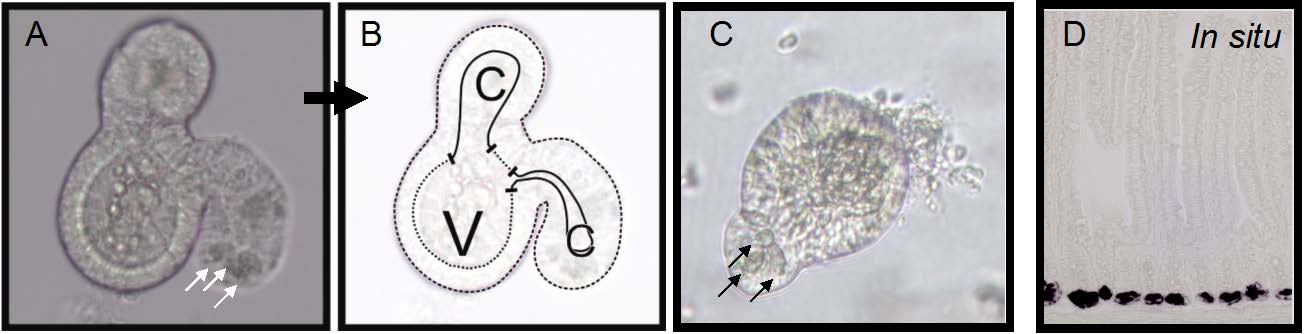
peptide secretion, as well as epithelial responses to a changed probiotic or prebiotic influence and the metabolic consequences thereof, we have set up the matrigel-based culture system for intestinal crypts in our laboratory (see Fig 1). In this culture system containing EGF, the Wnt agonist R-spondin 1 and the BMP inhibitor noggin, single crypt stem cells autonomously grow into crypt-like structures with de novo generated stem cells and Paneth cells at their bottom.
Results with this model
The Paneth cells amount up to 10% of the epithelial culture-all other relevant
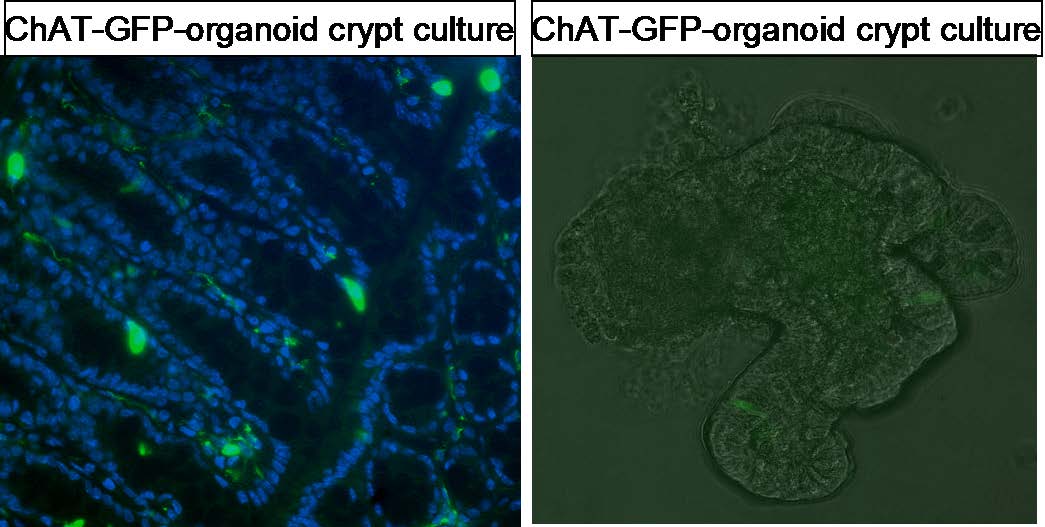
specialized epithelial cell types are represented such as neuroendocrine cells (marked by their expression of ChAT in vivo (A) as well as in organoid culture (B). An example of such an organoid culture is given in Fig. 1. As described earlier, Paneth cells are clearly distinguishable in these cultures (indicated by arrows in the figure). We have confirmed the presence of transcript and protein expression of relevant anti-microbial peptides in these organoid-derived cells in our own lab. Next to in situ hybridization studies (Fig1D), we have also interesting RNA-sequencing and microarray data available on the cytokine induced changes in epithelial retinoic acid metabolism that directly relate to the role of microbial influences on mucosal immune tolerance.
Clearly, these crypt cell based organoid cultures have as advantage that all relevant epithelial cell types (i.e. Paneth cells) are fully represented in the culture. Our group at AMC, in collaboration with the Gastroenterology Department, is further exploring the possibility to adapt the human crypt cell cultures as described earlier(2011l) at different levels and there is a clear opportunity for Research partner probiotic products to be tested in this system. Fig 1. An example of a 5-day organoid culture of crypt cells grown in matrigel. Panel A an B show clearly distinguishable Paneth cells in the crypt areas (arrows (A), in the crypt area (indicated by C)), and the villus dome (V). On the right panel C an earlier stage organoid is shown with autonomously proliferating crypt cells giving rise to Paneth cells indicated with arrows. Panel D shows tissue Paneth cells in the villus crypt using in situ hybridization for lysozyme transcript. WJ de Jonge and GR van der Brink; Unpublished, Tytgat Institute 2011. Fig.2 epithelial cells express enzymes for the production of acetylcholine (ChAT-shown as green signal in left) that can be found back in organoid systems (right). Potential use for Research partner. This culture setup allows us to study the direct effects of pre- and probiotics but also
microbial metabolic factors that regulate epithelial and Paneth cell peptide expression and secretion of antimicrobial peptides in an easily manipulated ex vivo setting. Further, we can study the effect of inflammatory cytokines that intervene in transcriptional regulation of antimicrobial peptide expression and secretion.
Parameter measured include protein analyses but also transcriptome analyses and Q-
PCR of epithelial cells. Antimicrobial peptide secretion (b-defensin A1-4, Lysozyme) can be analyzed by IHC and in situ hybridization that we do routinely in the laboratory (see for instance Fig 1D). furthermore human organoid systems are currently set up and will be operational shortly. Lentiviral shRNA strategies are in place to study specific gene regulation of epithelial responses.
5-further relevant assays for collaboration. -Next to routine lab analyses we run multiple assays in our lab including a wide
variety of ELISAs, Multiplex analyses, and state-of-the art FACS-sorting facility.
-The AMC houses an image suite with 2 confocal (new generation R8), life imaging
and multiple fluorescence microscopy options
-RNA-seq and ChIP Sequencing is done in house at the laboratory of Genome
-Human material is routinely processed and banked in a Biobank (being part of the
“string of pearls” the AMC has large biobanking availability). Importantly, we run state of the art isolations of specific cell types from human intestinal tissue.
Reference List
1. Posserud I, Syrous A, Lindstrom L, Tack J, Abrahamsson H, Simren M. Altered rectal
perception in irritable bowel syndrome is associated with symptom severity. Gastroenterology 2007;133:1113-1123.
2. Chitkara DK, van Tilburg MA, Blois-Martin N, Whitehead WE. Early life risk factors
that contribute to irritable bowel syndrome in adults: a systematic review. Am J Gastroenterol 2008;103:765-774.
3. Barreau F, Ferrier L, Fioramonti J, Bueno L. New insights in the etiology and
pathophysiology of irritable bowel syndrome: contribution of neonatal stress models. Pediatr Res 2007;62:240-245.
4. Posserud I, Agerforz P, Ekman R, Bjornsson ES, Abrahamsson H, Simren M. Altered
visceral perceptual and neuroendocrine response in patients with irritable bowel syndrome during mental stress. Gut 2004;53:1102-1108.
5. Van Den Wijngaard RM, Klooker TK, Welting O, Stanisor OI, Wouters MM, van der
CD, Bulmer DC, Peeters PJ, Aerssens J, de HR, Lee K, De Jonge WJ, Boeckxstaens GE. Essential role for TRPV1 in stress-induced (mast cell-dependent) colonic hypersensitivity in maternally separated rats. Neurogastroenterol Motil 2009;21:1107-1e94.
6. Van Den Wijngaard RM, Stanisor OI, van Diest SA, Welting O, Wouters MM, De
Jonge WJ, Boeckxstaens GE. Peripheral alpha-helical CRF (9-41) does not reverse stress-induced mast cell dependent visceral hypersensitivity in maternally separated rats. Neurogastroenterol Motil 2012;24:274-82, e111.
7. Klooker TK, Braak B, Koopman KE, Welting O, Wouters MM, van der HS, Schemann
M, Bischoff SC, Van Den Wijngaard RM, Boeckxstaens GE. The mast cell stabiliser ketotifen decreases visceral hypersensitivity and improves intestinal symptoms in patients with irritable bowel syndrome. Gut 2010;59:1213-1221.
8. Van Den Wijngaard RM, Welting O, Bulmer DC, Wouters MM, Lee K, De Jonge WJ,
Boeckxstaens GE. Possible role for TRPV1 in neomycin-induced inhibition of visceral hypersensitivity in rat. Neurogastroenterol Motil 2009;21:863-e60.
9. Barouei J, Moussavi M, Hodgson DM. Effect of Maternal Probiotic Intervention on
HPA Axis, Immunity and Gut Microbiota in a Rat Model of Irritable Bowel Syndrome. PLoS One 2012;7:e46051.
10. Eutamene H, Lamine F, Chabo C, Theodorou V, Rochat F, Bergonzelli GE, Corthesy-
Theulaz I, Fioramonti J, Bueno L. Synergy between Lactobacillus paracasei and its bacterial products to counteract stress-induced gut permeability and sensitivity increase in rats. J Nutr 2007;137:1901-1907.
11. Garcia-Rodenas CL, Bergonzelli GE, Nutten S, Schumann A, Cherbut C, Turini M,
Ornstein K, Rochat F, Corthesy-Theulaz I. Nutritional approach to restore impaired intestinal barrier function and growth after neonatal stress in rats. J Pediatr Gastroenterol Nutr 2006;43:16-24.
12. Gareau MG, Jury J, MacQueen G, Sherman PM, Perdue MH. Probiotic treatment of rat
pups normalises corticosterone release and ameliorates colonic dysfunction induced by maternal separation. Gut 2007;56:1522-1528.
13. Boeckxstaens GE, De Jonge WJ. Neuroimmune mechanisms in postoperative ileus. Gut
14. De Jonge WJ, Van Den Wijngaard RM, The FO, ter Beek ML, Bennink RJ, Tytgat GN,
Buijs RM, Reitsma PH, van Deventer SJ, Boeckxstaens GE. Postoperative ileus is maintained by intestinal immune infiltrates that activate inhibitory neural pathways in mice. Gastroenterology 2003;125:1137-1147.
15. De Jonge WJ, van der Zanden EP, The FO, Bijlsma MF, van Westerloo DJ, Bennink RJ,
Berthoud HR, Uematsu S, Akira S, Van Den Wijngaard RM, Boeckxstaens GE. Stimulation of the vagus nerve attenuates macrophage activation by activating the Jak2-STAT3 signaling pathway. Nat Immunol 2005;6:844-851.
16. De Jonge WJ, The FO, Lowenberg M, Boeckxstaens GE. P38 MAPK inhibitor
semapimod reduces postoperative ileus via peripheral and central mechanisms. Gastroenterology 2009;136:1841-1842.
17. The F, Cailotto C, van d, V, De Jonge WJ, Bennink RJ, Buijs RM, Boeckxstaens GE.
Central activation of the cholinergic anti-inflammatory pathway reduces surgical inflammation in experimental post-operative ileus. Br J Pharmacol 2011;163:1007-1016.
18. The FO, De Jonge WJ, Bennink RJ, Van Den Wijngaard RM, Boeckxstaens GE. The
ICAM-1 antisense oligonucleotide ISIS-3082 prevents the development of postoperative ileus in mice. Br J Pharmacol 2005;146:252-258.
19. The FO, Boeckxstaens GE, Snoek SA, Cash JL, Bennink R, Larosa GJ, Van Den
Wijngaard RM, Greaves DR, De Jonge WJ. Activation of the cholinergic anti-inflammatory pathway ameliorates postoperative ileus in mice. Gastroenterology 2007;133:1219-1228.
20. De Jonge WJ, The FO, van der Coelen D, Bennink RJ, Reitsma PH, van Deventer SJ,
Van Den Wijngaard RM, Boeckxstaens GE. Mast cell degranulation during abdominal surgery initiates postoperative ileus in mice. Gastroenterology 2004;127:535-545.
21. Snoek SA, Dhawan S, van Bree SH, Cailotto C, van Diest SA, Duarte JM, Stanisor OI,
Hilbers FW, Nijhuis L, Koeman A, Van Den Wijngaard RM, Zuurbier CJ, Boeckxstaens GE, De Jonge WJ. Mast cells trigger epithelial barrier dysfunction, bacterial translocation and postoperative ileus in a mouse model. Neurogastroenterol Motil 2012;24:172-84, e91.
22. The FO, Bennink RJ, Ankum WM, Buist MR, Busch OR, Gouma DJ, van der Heide S,
Van Den Wijngaard RM, De Jonge WJ, Boeckxstaens GE. Intestinal handling-induced mast cell activation and inflammation in human postoperative ileus. Gut 2008;57:33-40.
23. The FO, Buist MR, Lei A, Bennink RJ, Hofland J, Van Den Wijngaard RM, De Jonge
WJ, Boeckxstaens GE. The role of mast cell stabilization in treatment of postoperative ileus: a pilot study. Am J Gastroenterol 2009;104:2257-2266.
24. Wehner S, Meder K, Vilz TO, Alteheld B, Stehle P, Pech T, Kalff JC. Preoperative
short-term parenteral administration of polyunsaturated fatty acids ameliorates intestinal inflammation and postoperative ileus in rodents. Langenbecks Arch Surg 2012;397:307-315.
25. van Dullemen HM, van Deventer SJ, Hommes DW, Bijl HA, Jansen J, Tytgat GN,
Woody J. Treatment of Crohn's disease with anti-tumor necrosis factor chimeric monoclonal antibody (cA2). Gastroenterology 1995;109:129-135.
26. Braat H, Rottiers P, Hommes DW, Huyghebaert N, Remaut E, Remon JP, van Deventer
SJ, Neirynck S, Peppelenbosch MP, Steidler L. A phase I trial with transgenic bacteria expressing interleukin-10 in Crohn's disease. Clin Gastroenterol Hepatol 2006;4:754-759.
27. Heinsbroek SE, Oei A, Roelofs JJ, Dhawan S, te VA, Gordon S, De Jonge WJ. Genetic
deletion of dectin-1 does not affect the course of murine experimental colitis. BMC Gastroenterol 2012;12:33.
28. Ramakers JD, Mensink RP, Verstege MI, te Velde AA, Plat J. An arachidonic acid-
enriched diet does not result in more colonic inflammation as compared with fish oil- or oleic acid-enriched diets in mice with experimental colitis. Br J Nutr 2008;100:347-354.
29. Snoek SA, Verstege MI, van der Zanden EP, Deeks N, Bulmer DC, Skynner M, Lee K,
te Velde AA, Boeckxstaens GE, De Jonge WJ. Selective alpha7 nicotinic acetylcholine receptor agonists worsen disease in experimental colitis. Br J Pharmacol 2010;160:322-333.
30. te Velde AA, Pronk I, de KF, Stokkers PC. Glutathione peroxidase 2 and aquaporin 8 as
new markers for colonic inflammation in experimental colitis and inflammatory bowel diseases: an important role for H2O2? Eur J Gastroenterol Hepatol 2008;20:555-560.
31. Ten HT, Corbaz A, Amitai H, Aloni S, Belzer I, Graber P, Drillenburg P, van Deventer
SJ, Chvatchko Y, te Velde AA. Blockade of endogenous IL-18 ameliorates TNBS-induced colitis by decreasing local TNF-alpha production in mice. Gastroenterology 2001;121:1372-1379.
32. Wildenberg ME, Vos AC, Wolfkamp SC, Duijvestein M, Verhaar AP, te Velde AA, van
den Brink GR, Hommes DW. Autophagy attenuates the adaptive immune response by destabilizing the immunologic synapse. Gastroenterology 2012;142:1493-1503.
33. Jung P, Sato T, Merlos-Suarez A, Barriga FM, Iglesias M, Rossell D, Auer H, Gallardo
M, Blasco MA, Sancho E, Clevers H, Batlle E. Isolation and in vitro expansion of human colonic stem cells. Nat Med 2011;17:1225-1227.
34. Sato T, Vries RG, Snippert HJ, van de Wetering M, Barker N, Stange DE, van Es JH,
Abo A, Kujala P, Peters PJ, Clevers H. Single Lgr5 stem cells build crypt-villus structures in vitro without a mesenchymal niche. Nature 2009;459:262-265.
35. Sato T, van Es JH, Snippert HJ, Stange DE, Vries RG, van den Born M, Barker N,
Shroyer NF, van de Wetering M, Clevers H. Paneth cells constitute the niche for Lgr5 stem cells in intestinal crypts. Nature 2011;469:415-418.
a. some color improvement, some chest rise, and an oxygen saturation (per pulse oximetry) b. auscultation of breath sounds over the lateral chest bilaterally and presence of inspiratory sounds over the abdomen during assisted manual ventilation c. presence of mist in the tracheal tube d. presence of exhaled CO2 after delivery of 6 positive-pressure breaths 33. You are assisting at a statewide
Test Procedure for §170.302.d Maintain Active Medication List APPROVED Version 1.1 September 24, 2010 Test Procedure for §170.302 (d) Maintain Active Medication List This document describes the test procedure for evaluating conformance of complete EHRs or EHR modules1 to the certification criteria defined in 45 CFR Part 170 Subpart C of the Final Rule for Health Info