Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
Icr.eprints.org
This is an author produced version of an article that appears in:
Published text:
C Dearden, R Wade, M Else, S Richards, D Milligan, T Hamblin, D Catovsky, UK National Cancer Research Institute (NCRI), Haematological Oncology Clinical Studies Group, NCRI CLL Working Group (2008) The prognostic significance of a positive direct antiglobulin test in chronic lymphocytic leukemia: a beneficial effect of the combination of fludarabine and cyclophosphamide on the incidence of hemolytic anemia, Blood, Vol. 111(4), 1820-1826 Institute of Cancer Research Repository https://publications.icr.ac.uk
Please direct all emails to: publications@icr.ac.uk
The prognostic significance of a positive direct antiglobulin test in chronic lymphocytic leukemia – a beneficial effect of the combination of fludarabine and cyclophosphamide on the incidence of hemolytic anemia Running Title: DAT positivity and AHA in CLL Scientific Category: Clinical Trials and Observations Authors: Claire Dearden1, Rachel Wade2, Monica Else1, Sue Richards2,
Don Milligan3, Terry Hamblin4 and Daniel Catovsky1
From: Royal Marsden NHS Foundation Trust and Institute of Cancer Research, Downs
Road, Sutton, Surrey, SM2 5PT; Clinical Trial Service Unit, Richard Doll Building,
Roosevelt Drive, Oxford, OX3 7LF; Birmingham Heartlands Hospital, Bordesley Green
East, Birmingham, B9 5SS; and Royal Bournemouth Hospital, Castle Lane East,
For the UK National Cancer Research Institute (NCRI) Haematological Oncology
Clinical Studies Group and NCRI CLL Working Group
Corresponding author: Dr Claire Dearden, Royal Marsden NHS Foundation Trust,
Downs Road, Sutton, Surrey, SM2 5PT. Tel: 020 8661 3655, Fax: 020 8642 9634, e-
Abstract
Autoimmune hemolytic anemia (AHA) is a common complication in chronic
lymphocytic leukemia (CLL). The UK LRF CLL4 trial is the largest prospective trial in
CLL to examine the prognostic impact of both a positive direct antiglobulin test (DAT)
and AHA. 777 patients were randomized to receive chlorambucil or fludarabine, alone or
with cyclophosphamide (FC). The incidence pre-treatment of a positive DAT was 14%.
10% developed AHA. The DAT correctly predicted the development, or not, of AHA
after therapy in 83% of cases, however only 28% of DAT positive patients developed
AHA. Of 299 patients tested both pre- and post-treatment, those treated with single-agent
fludarabine were most likely to remain DAT positive and to change from negative to
positive. Patients treated with chlorambucil or fludarabine were more than twice as likely
to develop AHA as those receiving FC. In a multivariate analysis, stage C disease and
high beta-2 microglobulin were independent predictors of a positive DAT result. AHA, or
a positive DAT, with or without AHA, independently predicted for reduced overall
survival (OS). Four deaths, all on fludarabine monotherapy, were attributed to AHA. In
conclusion, DAT status at the time of initiation of therapy provides a new prognostic
indicator, although FC may protect against AHA. (204 words)Introduction
Autoimmune hemolytic anemia (AHA) is a common complication in chronic
lymphocytic leukemia (CLL), occurring in 10-25% of patients during the course of their
disease.1, 2 The direct antiglobulin test (DAT) may be positive at some time during the
disease course in up to 35% of cases, but overt AHA occurs less frequently. Although
AHA may occur in asymptomatic untreated CLL it is more common in patients with
advanced stage disease, 10.5% in Binet stage B and C, compared to only 2.9% in stable
stage A patients 1. A review of our data from MRC CLL Trials over the past 20 years
shows an incidence of AHA of 8.6% in 1273 patients, rising to 11% after treatment,
In 1966 a landmark paper first suggested that treatment with X-rays or alkylating agents
might trigger the onset of AHA in CLL.3 Following the advent of purine analog therapy
in the 1980s there have been a number of single case reports and small series, involving
over 100 patients, suggesting that AHA may occur more commonly following treatment
The main results of the LRF CLL4 trial conducted in the UK between 1999 and 2004
have been reported 10, including the incidence of AHA. The trial provided an opportunity
to study prospectively the incidence of a positive DAT and its relationship to the risk of
developing AHA in 777 previously untreated CLL patients who received therapy with
either chlorambucil or fludarabine given with or without cyclophosphamide. We present
Patients and trial design
LRF CLL4 was a prospective multi-center randomized controlled trial. The diagnosis of
CLL was confirmed by central review of morphology and immunophenotype. Patients
were eligible for trial entry if they had Binet stage C, B or A-progressive disease
requiring treatment and had not received any prior therapy. Treatment was allocated on a
2:1:1 ratio, to chlorambucil (10mg/m2/day for 7 days), or to fludarabine alone
(25mg/m2/day IV or 40mg/m2 oral, for 5 days), or to fludarabine plus cyclophosphamide
(FC) (F 25mg/m2/day plus C 250 mg/m2/day for 3 days IV or orally over 5 days with F
24 mg/m2/day plus C 150 mg/m2/day). Fludarabine was administered intravenously (IV)
until February 2001 when the oral formulation became available and the protocol was
modified to allow oral administration of the bio-equivalent dose. All treatment was given
every 4 weeks, F and FC for up to 6 cycles and chlorambucil up to 12 courses. The
response recorded was the best achieved at any time, following first line treatment.
Information regarding the result of the DAT test was requested at trial entry and at the
time of maximum response to first treatment. Patients with a positive DAT, but without
overt hemolysis, could be randomized in the trial with the recommendation that close
monitoring for onset of hemolysis should be followed.
AHA was defined by standard criteria: a drop in hemoglobin, associated with a positive
DAT and/or increased reticulocyte count and rise in indirect bilirubin with no other cause
for anemia identified. In some cases the diagnosis of AHA was supported by increased
levels of lactate dehydrogenase (LDH) and low haptoglobin. Patients with AHA were
eligible for the trial but received therapy for the hemolysis before initiating the allocated
treatment. Cases of AHA occurring during first line treatment were identified on the form
completed at the end of first line treatment. Pre-treatment AHA was not reported.
Treatment of patients with AHA followed conventional guidelines for idiopathic AHA;
namely prednisolone at 1mg/kg body weight per day for 2-4 weeks tapered off over
several weeks. Other therapies used included intravenous immunoglobulin, splenectomy,
cyclosporine A and rituximab. Details of treatment for AHA were not available.
Concomitant treatments for patients entered into the trial included: allopurinol for the
first 2-3 courses, cotrimoxazole throughout treatment and for 6 months after completion,
Other variables recorded at trial entry (either in all or in the majority of patients) and
included in analyses were: stage of disease, age, sex, ß2 microglobulin, LDH and
absolute lymphocyte count (ALC). A range of other prognostic markers were also
analysed for the majority of trial patients11: immunoglobulin heavy chain variable gene
mutation status, cytogenetics by florescence in situ hybridization (FISH), CD38 and
ZAP-70 expression. A full analysis of these will follow in a separate report and is not
Statistical methods
Overall survival was calculated from randomisation to death from any cause and
progression free survival (PFS) was time from randomisation to relapse needing further
therapy, progression or death from any cause. For non-responders and those with
progressive disease (NR/PD), the date of progression was when NR/PD was recorded.
Comparisons between categorical variables were made using the Chi squared test, and
between quantitative variables using the Wilcoxon rank sum test. Logistic regression
models were used to determine those factors that were independently associated with a
positive DAT result and with the development of AHA. Survival functions have been
estimated using the Kaplan-Meier method and groups compared with the log-rank test.
Multivariate Cox regression analysis was used to determine whether prognostic factors
were independently associated with outcome. A partial adjustment was made for missing
values of ß2 microglobulin, the variable with the largest proportion of missing data, using
the median value. All p-values are 2-sided.
The trial recruited 783 patients between February 1999 and October 2004, with follow-up
currently to 31st July 2006. Six patients were excluded for consent or diagnostic reasons,
387 (50%) were allocated to receive chlorambucil, 194 fludarabine alone and 196 FC.
Two patients were lost to follow-up. Thirty percent of patients were over 70 years of age.
DAT results
The DAT result in 637 patients (82%) was recorded at trial entry. In 107 patients the test
was not done and in 33 not recorded. After first treatment 333 patients (43%) had test
results, with 394 not done and 50 not recorded. At entry 89/637 patients (14%) tested
DAT positive and 44/333 (13%) after treatment. There were no significant differences
between the three treatment groups in either the percentage of patients with test results
available (range 80%-85% at entry and 39%-48% after treatment) or the percentage of
DAT positive results (14% chlorambucil, 13% fludarabine and 15% FC at entry, and
13%, 17% and 10% respectively after treatment). Of the 299 patients tested at both time
points, those treated with single-agent fludarabine were the most likely to remain DAT
positive (82% versus 52% chlorambucil, 42% FC) and the most likely to change from
negative to positive (9% versus 3%, 4%) (Table 1). Thus fludarabine increased the net
incidence of positivity in these patients by 4 cases (+5%), compared to 6 fewer cases after
chlorambucil (-4%) and 4 fewer after FC (-5%), but these differences were not
Incidence of AHA
Among 759 patients with information available, 77 (10%) developed AHA: 47 (12%)
receiving chlorambucil, 21 (11%) fludarabine alone and 9 (5%) FC (p=0.01). DAT
results on treatment were available for 331 of these. 20/39 (51%) with AHA were
positive compared with 23/292 (8%) of those without AHA. Information on AHA was
missing for 18 (2%) patients, of whom 10 died (4 within 40 days of entry) and none had a
The positive predictive value of the test (chance that a DAT positive patient will develop
AHA) was 28% (38%, 29% and 12% for chlorambucil, fludarabine and FC respectively).
The negative predictive value of the test (chance that a DAT negative patient will be
AHA-free) was 93% (92%, 90% and 96% respectively). Thus the DAT test at entry
correctly predicted the development of AHA or not after therapy in 83% of cases (84%,
82% and 83% respectively). Information was not recorded regarding either the time
elapsed from start of treatment until onset of AHA, or the incidence of AHA after
Outcomes of AHA
Patients who developed AHA were less likely than others to have responded to treatment
(43/65 (66% overall response rate) versus 530/654 (81%), p=0.004) and less likely to
have had a good (complete or nodular partial) response (12/65 (18%) versus 268/654
(41%), p=0.0004). Twelve AHA patients were not assessable for response (4 died less
than 6 months after entry). Those patients who developed AHA did receive less therapy:
41% only had 1-3 courses of chlorambucil compared to 14% without AHA, only 38%
completed 4-6 cycles of fludarabine compared to 73% of those without AHA and 56%
completed 4-6 cycles of FC compared to 74% non-AHA patients.
Four deaths were attributed to AHA during first-line treatment, all on fludarabine
monotherapy. These account for 1.5% of the total deaths in the trial to July 2006, or 2%
of deaths in which CLL was a cause. In patients treated with single-agent fludarabine
these accounted for 6% of total deaths and 7% of CLL deaths. Survival times from
randomisation for these four patients were 1, 3, 3 and 5 months. Three were DAT
positive, and one negative, at entry; 3 received oral and one iv fludarabine, for between
one and 3 courses. Of the 4 patients, 3 presented with Stage C disease and 1 with stage B,
1 patient had unmutated VH genes, 2 mutated and 1 not known and 1 patient had a p53
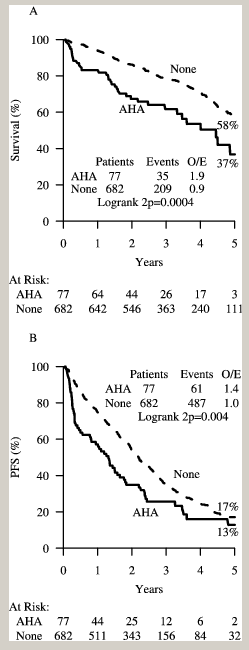
Survival at 5 years of patients without AHA was 58% (95% confidence interval (CI):
53%-63%) compared to 37% (95% CI: 20%-53%) for patients who developed AHA,
Odds Ratio (OR) = 0.40 (95% CI: 0.25-0.63) p=0.0004 (Figure 1a). PFS was
significantly better for those who did not develop AHA (18% (95% CI: 14%-22%) at 5
years) compared to patients with AHA (9% (95% CI: 0%-18%) at 5 years)); OR = 0.55
(95% CI: 0.40-0.75) p=0.0005) (Figure 1b). There was no statistically significant
difference in the impact of AHA by treatment group for either PFS or OS (however
numbers are small with only nine AHA cases in the FC group).
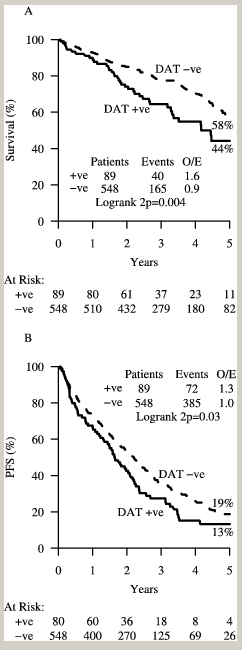
Predictive value of DAT at trial entry for other outcomes
Comparing DAT positive with DAT negative patients, the former were just as likely to
respond to treatment: 64/83 (77%) versus 404/512 (79%) (p=0.7); but they had fewer
good (complete or nodular partial) responses: 22/83 (27%) versus 198/512 (39%)
(p=0.03). Overall survival was significantly better for DAT negative patients (58% (95%
CI: 52%-63%) at 5 years) compared with DAT positive patients (44% (95% CI: 31%-
57%); OR = 0.53 (95% CI: 0.35-0.79) p=0.004) (Figure 2a). Similarly, when considering
PFS, the DAT negative patients fared significantly better (19% (95% CI: 15%-24%) at 5
years) compared to the DAT positive patients (13% (95% CI: 5%-21%); OR = 0.72 (95%
After exclusion of patients who developed AHA, DAT negative patients still had better
survival than DAT positive patients (p=0.01) (Figure 3). Thus the difference in survival
between DAT positive and negative patients is not accounted for by those who developed
AHA. A similar trend is seen for PFS but is not statistically significant. For patients
where the DAT result has been recorded, multivariate Cox regression analysis of
variables including treatment allocation, AHA, DAT and conventional risk criteria (i.e.
stage of disease, age, sex), showed both the DAT result and AHA independently and
significantly associated with overall survival (both p=0.03) and the DAT result, but not
AHA, significantly associated with progression free survival (p=0.005). A multivariate
analysis of all available covariates (which includes additionally ß2 microglobulin, LDH,
ALC, and % bone marrow lymphocytes) confirmed that the DAT result retained its
independent prognostic value for PFS (Hazard Ratio (HR) for DAT positive=1.35, 95%
CI: 1.03-1.78, p=0.03), although ß2 microglobulin could only be partially allowed for as
the result was only available for 484 (76%) of patients. Moreover, both AHA and the
DAT result retained their independent prognostic value for overall survival (HR for AHA
= 1.52, 95% CI: 1.02-2.26, p= 0.04. HR for DAT positive= 1.46, 95% CI: 1.02-2.10, p=
Factors predicting DAT results at trial entry and AHA development
Univariate analysis considered the following variables and their association with AHA
status and with DAT result at entry: stage of disease, age, sex, treatment allocation, ß2
microglobulin, absolute lymphocyte count (ALC), LDH and percentage of bone marrow
A DAT-positive test result at entry was associated with more advanced stage of disease,
higher ß2 microglobulin and higher ALC (Table 2). Multivariate analysis showed that
stage of disease and ß2 microglobulin were the only clear independent predictors of DAT
result, with stage C patients more likely to be DAT positive than stage A progressive or B
patients (HR for stage C= 2.23, 95% CI: 1.3-3.82, p=0.004; HR for unit increase in ß2
microglobulin =1.11, 95% CI: 1.01-1.23, p=0.03). A further analysis including genetic
markers showed that immunoglobulin heavy chain mutation and FISH results (deletion at
11q23) were only of borderline significance (p=0.05). However these results require
careful interpretation because laboratory data are not available for all patients. A detailed
Table 3 shows that the development of AHA is associated with stage C disease, positive
DAT result, higher ß2 microglobulin, treatment with chlorambucil or fludarabine
monotherapy and older age. Multivariate analysis (Table 4) highlighted DAT test result,
age, stage of disease and treatment as independent predictors of AHA. Genetic markers
were not significant in multivariate analysis. In the 621 patients for whom the DAT result
at trial entry and AHA were recorded, those treated with chlorambucil or fludarabine
monotherapy were roughly three times more likely to develop AHA compared to FC
patients. Those with a negative DAT result at trial entry had a 77% reduced odds of
developing AHA. The odds of developing AHA increased with age and were greater for
patients with stage C disease than for earlier stage patients.
Discussion
The UK LRF CLL4 trial is the largest prospective trial in CLL to examine the incidence
and prognostic impact of a positive DAT and AHA in patients requiring therapy. We
report an incidence of a positive DAT of 14% and AHA of 10%, levels which are
consistent with previous studies in patients with active CLL.1, 12, 13
The number of patients with a positive DAT at trial entry was well balanced across all
three treatment arms. Less than half of the patients were tested after completion of
treatment, but of those tested at both time points 5% became DAT positive after therapy
with the greatest risk (9%) occurring in the fludarabine monotherapy arm. For patients
receiving the combination of fludarabine and cyclophosphamide the percentage of DAT
positive individuals fell after treatment whilst it increased in the fludarabine
monotherapy arm. This suggests a tendency for FC treatment to reduce the rate of DAT
positivity. In multivariate analysis of pre-treatment parameters a DAT positive result was
associated with more advanced stage of disease, as previously reported.1 In addition a
strong link was shown between increased ß2 microglobulin levels and a positive DAT.
This observation has also been reported by Borthakur et al.14
The DAT result had an important independent association with the development of AHA.
The approximate risk of a patient with a positive DAT developing AHA was 1 in 3. DAT
negativity was a strong predictor (>90%) for not developing AHA after therapy. Only
49% of reported AHA cases were DAT negative in this trial, in contrast with 82% in the
results recently reported by Borthakur et al 14 for CLL patients treated with FC plus
rituximab. This finding may be related to the use of rituximab in the treatment regimen as
they suggest, or may be related to the diagnostic definitions of AHA used.
The mechanism of AHA in CLL is still poorly understood. It usually results from
production of high affinity polyclonal IgG auto-antibodies by the non-malignant B-
lymphocytes. Possible mechanisms include: aberrant antigen presentation by CLL B-
cells, defective T-cell function, and loss of regulatory T-cells, with subsequent failure of
control of auto-reactive T-cells. 15-18 The latter may result from initiation of therapy and
explain the frequent reports of AHA occurring in association with treatment for CLL. In
LRF CLL4 the lowest incidence of AHA (5%) was seen in the FC arm. This level
compares with that reported by Borthakur et al for the FCR regimen of 6.5%, 14
suggesting that the combination of cyclophosphamide with fludarabine may have a
protective effect against the development of AHA. Patients receiving chlorambucil or
fludarabine monotherapy were three times more likely to develop AHA than those
There were four deaths from autoimmune hemolysis after first-line therapy, accounting
for 2% of all deaths in the trial. All these cases occurred in patients receiving fludarabine
monotherapy. This study therefore agrees with the observation that AHA occurring in
association with fludarabine treatment may be more severe 4, 5. In contrast, both the
incidence and the severity of AHA were lower for those patients receiving FC. There are
a number of possible explanations for this. Patients achieving good remissions may be at
less risk of developing AHA and therefore the most effective treatment is likely to be
associated with reduction in the incidence of AHA. The treatment responses in LRF
CLL4, which have been reported elsewhere 10, showed that, although there was no
significant difference in survival, the overall and complete response (CR) rates and the
PFS were significantly better with FC than with either fludarabine alone or chlorambucil.
The CR rate was 38% for FC, 15% for fludarabine and 7% for chlorambucil. The German
CLL and US Intergroup study groups have also reported superior response rates and PFS
for FC compared to F alone. 19, 20 In the German study there was a reduction in incidence
of AHA in the FC arm whilst in the US trial there was no difference in AHA between the
two treatment arms. A second possibility is the total dose of fludarabine administered. In
fludarabine monotherapy the total dose was 200mg/m2 compared to 120mg/m2 when
fludarabine was administered in combination with cyclophosphamide. If, as previously
postulated by some 7, fludarabine is directly implicated in the development of AHA, there
may be a dose relationship. Finally, one might propose that cyclophosphamide, an agent
which is commonly used to treat autoimmune disease because of its immunosuppressive
properties, could provide a protective effect when administered in combination with
The development of AHA was associated not only with a positive DAT and treatment
modality, but also with more advanced disease stage and older age. Mauro et al 12 and
Barcellini et al 13 have also reported age above 65 years as a predictor of AHA although
this was not confirmed by Borthakur et al 14. The relationship between AHA and
advanced stage has been a consistent finding across all studies. In our study, development
of autoimmune hemolysis was associated with a poorer response to treatment and with
both shorter PFS (9% versus 18%) and overall survival (37% versus 58%) at 5 years. In
multivariate analysis AHA retained independent prognostic value for OS but not for PFS.
Three other studies have failed to show any independent effect of AHA on survival
Perhaps the most interesting, and somewhat surprising, observation in this study was the
prognostic significance of a positive DAT, with or without associated AHA. Although
overall response to treatment was the same regardless of DAT status, this did influence
quality of remissions, with good (complete or nodular partial) response rates of 27% for
DAT positive patients versus 39% for DAT negative patients (p=0.03). PFS and overall
survival were better for DAT negative patients, even after exclusion of those who
developed AHA. Multivariate analysis showed this to be a significant independent
prognostic variable. This is the first report of the prognostic significance of the DAT test
in CLL. The reason why a positive DAT should be a risk factor in CLL is not clear. It
may be a surrogate marker for other poor prognostic features such as immunoglobulin
heavy chain gene mutation status and further studies will be needed to elucidate this.
In conclusion, the FC combination has a beneficial effect on both the DAT expression
and on the development of AHA during treatment of CLL. In addition, the DAT status at
the time of initiation of therapy provides a new prognostic indicator for both PFS and OS.
The DAT test remains, therefore, an important pre-treatment assessment for all patients.
Patients who are DAT positive may benefit from FC or FC plus rituximab rather than
fludarabine or chlorambucil monotherapy.
Acknowledgments:
LRF CLL4 was funded by a core grant from Leukaemia Research UK. Laboratory
studies were funded by an educational grant from Schering Health Care (UK) and
Schering AG (Germany). We are grateful to all physicians and research staff who
Author contributions: Claire Dearden, wrote the paper;
Rachel Wade, performed statistical analysis;
Monica Else, wrote part of paper (results section);
Sue Richards, performed statistical analysis;
Daniel Catovsky, edited the manuscript and was trial co-ordinator
Potential Conflicts of Interest: Claire Dearden:consulting and lecture fees from
Schering AG; Daniel Catovsky:consulting and lecture fees from Schering AG, Roche and
Genmab; the other authors have no competing financial interests to declare.
References
1. Hamblin TJ, Oscier DG and Young BJ. Autoimmunity in chronic lymphocytic leukaemia. J Clin.Pathol. 1986;39:713-716. 2. Diehl LF, Ketchum LH. Autoimmune disease and chronic lymphocytic leukemia: autoimmune hemolytic anemia, pure red cell aplasia, and autoimmune thrombocytopenia. Semin.Oncol. 1998; 25: 80-97.
3. Lewis FB, Schwartz RS, Damashek W. X-irradiation and alkylating agents as possible trigger mechanisms in autoimmune complications of malignant lymphoproliferative diseases. Clin Exper Immunol. 1966; 1:3-11. 4. Bastion Y, Coiffier B, Dumontet C, Espinouse D, Bryon PA. Severe autoimmune hemolytic anemia in two patients treated with fludarabine for chronic lymphocytic leukemia. Ann Oncol 1992;3:171-172. 5. Byrd JC, Hertler AA, Weiss RB, Freiman J, Kweder SL, Diehl LF. Fatal recurrence of autoimmune hemolytic anemia following pentostatin therapy in a patient with a history of fludarabine-associated hemolytic anemia. Ann Oncol. 1995;6:300-301. 6. Robak T, Blasinska-Morawiec M, Krykowski E, Hellmann A, Konopka L. Autoimmune haemolytic anaemia in patients with chronic lymphocytic leukaemia treated with 2-chlorodeoxyadenosine (cladribine). Eur J Haematol .1997;58:109-113. 7. Myint H, Copplestone JA, Orchard J, et al. Fludarabine-related autoimmune haemolytic anaemia in patients with chronic lymphocytic leukaemia. Br J Haematol. 1995;91:341-344. 8. Gonzalez H, Leblond V, Azar N, et al. Severe autoimmune hemolytic anemia in eight patients treated with fludarabine. Hematol.Cell Ther. 1998:40:113-118.
9. Weiss RB, Freiman J, Kweder SL, Diehl LF, Byrd JC. Hemolytic anemia after fludarabine therapy for chronic lymphocytic leukemia. J.Clin.Oncol. 1998;16:1885-1889. 10. Catovsky D, Richards S, Matutes E, et al. Assessment of fludarabine plus cyclophosphamide for patients with chronic lymphocytic leukemia (the LRF CLL4 Trial): A randomized controlled trial. Lancet. 2007; 370: 230-39.
11. Oscier DG, Wade R, Orchard J, et al. Prognostic Factors in the UK LRF CLL4 Trial. Blood (ASH Annual Meeting Abstracts) 2006;108:299.
12. Mauro FR, Foa R, Cerretti R, et al. Autoimmune hemolytic anemia in chronic lymphocytic leukemia: clinical, therapeutic, and prognostic features. Blood. 2000;95:2786-2792.
13. Barcellini W, Capalbo S, Agostinelli RM, et al. Relationship between autoimmune phenomena and disease stage and therapy in B-cell chronic lymphocytic leukemia. Haematologica. 2006;91:1689-1692.
14. Borthakur G, O'Brien S, Wierda WG, et al. Immune anaemias in patients with chronic lymphocytic leukaemia treated with fludarabine, cyclophosphamide and rituximab - incidence and predictors. Br.J.Haematol. 2007;136:800-805. 15. Pritsch O, Maloum K, Dighiero G. Basic biology of autoimmune phenomena in chronic lymphocytic leukemia. Semin.Oncol. 1998;25:34-41.
16. Hall AM, Vickers MA, McLeod E, Barker RN. Rh autoantigen presentation to helper T cells in chronic lymphocytic leukemia by malignant B cells. Blood. 2005:105: 2007-2015.
17. Kyasa, M J, Parrish RS, Schichman SA, Zent CS. Autoimmune cytopenia does not predict poor prognosis in chronic lymphocytic leukemia/small lymphocytic lymphoma. Am.J.Hematol. 2003;74:1-8.
18. Hamblin TJ. Autoimmune complications of chronic lymphocytic leukaemia. Semin Oncol. 2006;33:230-239.
19. Eichhorst BF, Busch R, Hopfinger G, et al. Fludarabine plus cyclophosphamide versus fludarabine alone in first-line therapy of younger patients with chronic lymphocytic leukemia. Blood. 2006;107:885-891.
20. Flinn IW, Neuberg DS, Grever MR, et al. Phase III trial of fludarabine plus cyclophosphamide compared with fludarabine for patients with previously untreated chronic lymphocytic leukemia: US Intergroup Trial E2997. J Clin Oncol. 2007;25:793-798.
Table 1. DAT Results in 299 patients with results available both at entry and after treatment Table 2. Association between patient characteristics and DAT result at entry
DAT –ve Age <60 178 (86%) progressive B 245 (89%) C 157 (77%) Sex Female Treatment Chlorambucil Fludarabine p-value** B2M (mg/l) ALC (x109/l) (n=619) LDH (U/l)
recorded on n=637 patients unless otherwise stated
Table 3. Association between patient characteristics and AHA
Age <60 60-69 256 (90%) 70+ 195 (86%) progressive Sex Female 180 (90%) Male 502 (90%) Treatment Chlorambucil Fludarabine DAT Positive Negative Unknown/Missing B2M (mg/l) ALC (x109/l) (n=734) LDH (U/l)
recorded on n=759 patients unless otherwise stated
test does not include DAT unknown/missing patients
Table 4 – Multivariate logistic regression: independent factors associated with AHA (621 patients)
Odds Ratio after adjustment for other 3 independent predictors
Figure Legends Figure 1: a) Survival and b) PFS by AHA or not, as recorded on end of first line treatment form Figure 2: a) Survival and b) PFS by DAT test result at trial entry
Figure 3: Survival and PFS: differences in event rates by entry DAT result within AHA subgroup. The squares and lines show the estimated odds ratios and their 95% confidence intervals. The size of each square is proportional to the amount of information available in the subgroup. Overall estimates are shown by a diamond, with the width representing the 95% confidence interval.
Combustible Gas and Vapors Combustible Gas Detector 0-100% LEL Continuous LCD shows real-time gas concentration with backlight in low light (auto); in alarm (auto) and on demand Compact (1.5 x 2.0 x 3.75 in / 38.5 x 50 x 95 mm) and Provides 90 dB tone and bright LED indication on alarm Peak value displayed on command in % LEL LOW and HIGH alarms with adjustable setpoints

 This is an author produced version of an article that appears in:
Published text:
This is an author produced version of an article that appears in:
Published text: