Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
Hc439901930p
Current Perspective Coronary Heart Disease: Reducing The Risk A Worldwide View
Gerd Assmann, FRCP; Rafael Carmena, MD; Paul Cullen, FRCPI; Jean-Charles Fruchart, PhD;
Fabrizio Jossa, MD; Barry Lewis, FRCP; Mario Mancini, MD; Rodolfo Paoletti, MD;
for the International Task Force for the Prevention of Coronary Heart Disease
Worldwide, cardiovascular diseases are now the most risk increases steeply, approaching that of men after the age
common cause of death and a substantial source of
chronic disability and health costs. In the light of new datafrom clinical trials and a fuller understanding of risk factors,
History of Cardiovascular Disease
the International Task Force for the Prevention of Coronary
The risk of further CHD events or stroke is much higher in
Heart Disease, in cooperation with the International Athero-
persons with a history of myocardial infarction, angina,
sclerosis Society, prepared a revised and comprehensive
stroke, or intermittent claudication and in those who have
statement regarding the scientific basis of the primary and
ischemic changes on resting or exercise ECG than in persons
secondary prevention of cardiovascular disease. The follow-
without such findings. Any of these features confers grade III
ing is a short account of the clinical implications of this
status (high risk; Table 1) and warrants vigorous reduction of
statement. It is best read in conjunction with the full docu-
ment, which can be found at http://www.chd-taskforce.com
Positive Family History of CHD, Stroke, or Peripheral Vascular Disease Assessing the Global Risk of
Note any reliable cardiovascular family history, and grade its
Cardiovascular Disease
severity on the basis of the following.
Assessing a patient’s overall or global risk of cardiovasculardisease is the first step in preventive care, for it enables the
● How early in life relatives were affected (discount events
physician to identify and provide the appropriate level of
treatment for risk factors. Much can be learned from measur-
● The closeness of the relationships (eg, CHD in a sibling or
ing even a few risk factors. The fuller the knowledge of the
parent confers greater risk than CHD in an uncle)
patient’s risk status, the sounder the treatment decisions.
● What proportion of adult relatives were affected
Initial costs may be offset by long-term rational treatment. The goals of treatment and, hence, the extent of dietary
Smoking
change and the need for (and choice and dosage of) drug
Note the duration and amount of current and former use of
treatment all depend on global risk assessment. Two methods
cigarettes and other tobacco products; these are potent but
potentially reversible causes of CHD. Psychosocial Risk Factors There is increasing evidence that stress, lack of social
Note and tabulate the following risk factors, including those
support, depression, and low socioeconomic status are asso-
laboratory investigations that are available.
ciated with an increased risk of CHD. Although specific
Age, Sex, and Menopausal Status
treatment for these factors is often difficult, assessing them is
Risk increases progressively with adult age, and coronary
still an important part of the work-up. The psychosocial
heart disease (CHD) is most common after the age of 60
profile of the patient also has a large influence on the patient’s
years. In premenopausal women, CHD is rare (except in those
ability to comply with measures such as lifestyle modifica-
who use oral contraceptives and smoke). After menopause,
From the Institute of Arteriosclerosis Research and Institute of Clinical Chemistry and Laboratory Medicine, University of Mu¨nster, Germany (G.A.,
P.C); Faculty of Medicine, University of Valencia, Spain (R.C.); Department for the Study of Lipids and Lipoproteins, Institut Pasteur de Lille, France(J.-C.P.); Department of Clinical and Experimental Medicine, University of Naples, Italy (F.J., M.M.); University of London, UK (B.L.); Faculty ofPharmacy, University of Milan, Italy (R.P.)
Correspondence to Gerd Assman, FRCP, Institut fuer Arterioskleroseforschung, Universitaet Muenster, Albert-Schweitzer-Strasse 33, 48149 Muenster,
The full version of this document, which was prepared in cooperation with the International Atherosclerosis Society, was published in Nutrition,Metabolism and Cardiovascular Disease 1998;8(3):205–271, and is also available on the Task Force Internet home page at http://www.chd-taskforce.com
A complete list of investigators can be found in the full version of this document. (Circulation. 1999;100:1930-1938.) 1999 American Heart Association, Inc. Circulation is available at http://www.circulationaha.org 1930 Assmann et al Reducing Coronary Heart Disease 1931 Clinical Risk Assessment
Presence of 1 risk factor of moderate degree in a
Presence of 1 risk factor of severe degree in a
History of myocardial infarction, angina, stroke, or
middle-aged man, eg, plasma cholesterol 200 –250
middle-aged man, eg, smokes 20 cigarettes per
peripheral vascular disease, ECG evidence of CHD,
mg/dL (5.2– 6.5 mmol/L), BP 170/100, or smokes
day, plasma cholesterol Ͼ250 mg/dL (Ͼ6.5
or evidence of coronary or carotid plaques
mmol/L), diabetes, or family history in a closerelative
Presence of 2 risk factors of moderate degree in a
Presence of 2 risk factors of severe degree, eg,
middle aged man, eg, plasma cholesterol 200–250
plasma cholesterol Ͼ250 mg/dL (Ͼ6.5 mmol/L)
mg/dL (5.2–6.5 mmol/L) and HDL cholesterol Ͻ35
and smokes 20 cigarettes a day, diabetes, or
Presence of 3 risk factors of moderate degree
Familial hypercholesterolemia or remnanthyperlipidemia
BP indicates blood pressure. *Ϸ3 CHD events per 1000 per year in middle-aged men; 3rd quintile of PROCAM algorithm. †Ϸ7 CHD events per 1000 per year in middle-aged men; 4th quintile of PROCAM algorithm. ‡Ϸ23 CHD events per 1000 per year in middle-aged men; 5th quintile of PROCAM algorithm. In PROCAM (1978 –1996), more than 30 000 individuals at work in Germany were assessed for Ͼ30 anthropometric and laboratory parameters. Based on PROCAM,
a formula for calculating CHD risk in middle-aged men was derived that takes into account age, systolic blood pressure, LDL cholesterol, HDL cholesterol, triglyceride,smoking behavior, presence of diabetes mellitus, positive family history of myocardial infarction, and presence of angina pectoris. It is available as an interactiveprogram at http://www.chd-taskforce.com. Examination Investigations Weight and Height Plasma Lipids and Lipoproteins
Derive the body mass index (BMI) by nomogram or calcu-
The preferred investigation for plasma lipids and lipoproteins
lation (BMIϭweight in kg/height in m2). Overweight is
is one that measures total cholesterol, triglycerides, HDL
defined as a BMIϾ25 and obesity as a BMIϾ30. Excess
cholesterol, and LDL cholesterol after a 14-hour fast (water
adipose tissue in the truncal region is an important cardio-
permitted). If the full profile is unavailable, plasma choles-
vascular disease risk factor, and it adversely affects blood
terol alone is useful in defining risk and diagnosing some
pressure, cholesterol (total, HDL, and LDL), and triglyceride
levels and glucose tolerance. Truncal obesity can be assessed
Lipid levels are continuously related to risk. Take particular
and treatment can be monitored by estimating the weight/hip
note of an LDL cholesterol level Ͼ135 mg/dL (Ͼ3.5 mmol/L),
ratio (circumference of waist at umbilicus/circumference of
a HDL cholesterol level Ͻ35 mg/dL (Ͻ0.9 mmol/L), and a
hips at widest part; it is normally Ͻ1.0 in men and Ͻ0.85 in
triglyceride level of 150 to 400 mg/dL (1.7 to 4.5 mmol/L).
women) or by measuring girth horizontally at the level of the
Lipids can be assessed in a blood sample taken within 24 hours
umbilicus (normally Ͻ94 cm in men and Ͻ80 cm in women).
Truncal obesity syndrome is often accompanied by some
of the onset of myocardial infarction; thereafter, LDL cholesterol
or all of the following features: high plasma triglycerides, low
levels often fall and only return to their previous level after Ϸ3
HDL cholesterol, type 2 diabetes, hypertension, and an
months. Lipid measurements can also be reduced for 3 months
increased risk of CHD. A key mechanism is insulin resis-
after a severe illness and for 2 weeks after a minor illness. Levels
tance. Reducing overweight is often highly effective against
of lipoprotein(s) exceeding 30 mg/dL confer increased risk. Blood Glucose Blood Pressure
Type 1 and type 2 diabetes confer a markedly increased risk
Blood pressure is continuously related to the risks of stroke
of CHD; even impaired glucose tolerance is often accompa-
and CHD over a wide range, although a systolic pressure of
nied by lipid risk factors and elevated blood pressure.
Ն160 mm Hg and/or a diastolic pressure Ն90 mm Hg is used
Diabetes should be suspected in persons with diabetic
to define hypertension. Isolated systolic hypertension
symptoms and random plasma glucose levels Ͼ200 mg/dL
(Ͼ160 mm Hg) is an important risk factor in the elderly.
(Ͼ11.1 mmol/L). Diabetes is now defined as a plasma
Blood pressure is best measured with the subject seated, after
glucose level Ͼ126 mg/dL (Ͼ7 mmol/L) after fasting for 8
hours and/or a plasma glucose level Ͼ200 mg/dL
Cardiovascular Examination
(Ͼ11.1 mmol/L) at 2 hours during an oral glucose tolerance
The cardiovascular examination may reveal a carotid bruit or
a missing peripheral pulse, denoting existing atherosclerotic
Other CHD risk factors that are now measured in many
disease and conferring grade III risk.
laboratories include fibrinogen and homocysteine. 1932 Circulation November 2, 1999 Management of CHD Risk Factors Smoking Simple counseling is the first approach in the management of smoking cessation, and it is often effective. Ask how con- cerned the smoker is with his or her habit and how much he or she wants to stop. Reinforce the patient’s desire (verbally and by providing written materials) to stop smoking by spelling out the following benefits of smoking cessation.
● How rapidly her or his well being will improve after
quitting (eg, food tastes better, effort tolerance improves,and morning cough subsides)
● The risks of continuing to smoke, including the high risk of
CHD (including sudden death, stroke, and peripheral vas-cular disease), the several smoking-related cancers, and
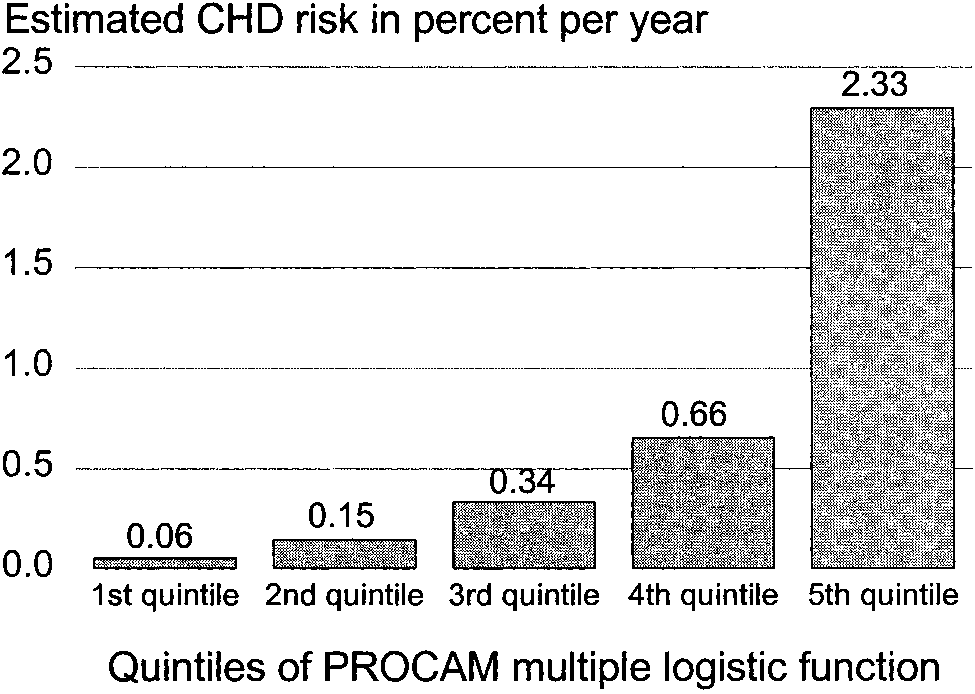
Estimated risk of a coronary event among men aged 40 to 65
years in the Mu¨nster Heart Study, expressed as quintiles of the
● The progressive decline of the above risks in ex-smokers
PROCAM multiple logistic function. Reproduced with permission
from Nutr Metab Cardiovasc Dis. 1998;8:205–271 (also availableat http://www.chd-taskforce.com).
Clearly and firmly counsel the patient to stop smoking with apositive, encouraging, and sympathetic attitude. Second or
On the basis of the presence, number, and severity of some
further attempts are often more successful than the first. Try
or all of these 11 groups of risk factors, increased risk is
to help arrange for support by others (eg, the patient’s
assigned to 1 of 3 grades: I, II, or III, as seen in Table 1.
spouse). Help the smoker identify trigger factors for smoking
Appropriate treatment decisions are based on this grading.
(eg, drinking alcohol or coffee, using the telephone, or
In asymptomatic patients at increased risk, the precision of
driving a car); awareness of the trigger lessens its impact. If
risk assessment may be enhanced by imaging methods.
possible, the trigger should be avoided.
Noninvasively, quantitative carotid Doppler ultrasound can
If the attempt to stop smoking fails, the next attempt may
be used. Increased interomedial thickness is predictive of a
be more successful if preceded by a period of “minimum
2-fold increase in CHD risk, and detection of carotid plaques
smoking:” when subjects feel the urge to smoke, they ask
themselves whether they really need to do so at that moment. Often, they realize that smoking can be postponed. Another
Method II
approach for the unsuccessful quitter is referral to a smoking
Quantitative Risk Assessment
cessation class run by a skilled counselor or psychologist.
On the basis of 9 risk factors, data from the Prospective
Nicotine dependence can be dealt with by coupling the
Cardiovascular Mu¨nster (PROCAM) Study are used to provide
above approach with nicotine replacement in patients without
a quantitative estimate of risk (Figure) using an algorithm that is
CHD. Use nicotine skin patches or nasal spray and progres-
currently applicable to men aged 40 to 65 years (Appendix 1).
This is available as an interactive program on the Task Forcewebsite (http://www.chd-taskforce.com). Treating Overweight and Obesity The physician’s attitude is important when treating patients Primary and Secondary Prevention
with weight problems. Encouragement, patience, and enthu-
Evidence of a myocardial infarction, stroke, or other athero-
siasm are needed. Encourage the patient to combine an
sclerotic disease confers a high risk of further cardiovascular
exercise program (see below) with changes in diet. Empha-
events and has a risk level of grade III. Patients in this
size that some elements of lifestyle change will need to be
category require vigorous intervention against risk factors,
life-long, and spell out the benefits of weight reduction. The
and clear evidence exists showing the benefits of such
immediate and expected future benefits of weight reduction
intervention. Reducing risk in such patients is termed second-
ary prevention, whereas risk reduction in persons without
such evidence is termed primary prevention. Evidence of
CHD is a special case within the high-risk group (ie, among
persons with grade III risk). Primary prevention in persons
with grade III risk requires equally vigorous intervention
against risk factors, and equally cogent evidence exists
showing its benefits. Because 30% of patients with a first
Lower LDL cholesterol and triglyceride levels and higher
manifestation of CHD (such as myocardial infarction) survive
for Ͻ3 months and because such first events may lead to
prolonged or permanent disability, the potential benefits of
Lesser risk of diabetes, certain cancers, accidents, and
primary prevention exceed those of secondary prevention. Assmann et al Reducing Coronary Heart Disease 1933 Choice of Foods in the Cholesterol-Lowering Diet
breakfast cereals with emphasis onlow-sugar, low-salt brands; porridge;muesli; pasta; rice; crispbread(crackers); matzo
All white and oily fish (grilled, poached,
oils, (eg, sunflower, corn, walnut,safflower); soft (unhydrogenated)margarines rich in monounsaturated orpolyunsaturated oils; low-fat spreads
biscuits (cookies), pies, snacks, andpuddings
malted drinks; boiled “Turkish” coffee*
Added salt; salad dressings; saladcream (ie, Miracle Whip); mayonnaise
*Coffee grounds contain a substance that may increase blood cholesterol; hence, filtered or instant coffee is preferable in patients with hyperlipidemia. Reproduced with permission for Nutr Metab Cardiovasc Dis. 1998;8:205–271 (also available at http://www.chd-taskforce.com).
Examples of suitable aerobic activities include walking (an
The reducing diet consists of a maintained or increased
excellent exercise), jogging, cycling, and calisthenics, such as
intake of low energy-density foods (which help control
aerobic classes and rowing; individual preference is impor-
appetite), such as green vegetables, salad vegetables, and
tant for long-term compliance. Before more strenuous exer-
clear soups and a decreased intake of high energy– density
cise, a warm-up period of 5 minutes of stretching and other
and nonsatiating foods, including alcohol, all fats and oils,
gentle activity is advised, as is a final cool-down period of
and sugar-containing foods. An example of such a diet is
Exercise dosage is determined by its duration, intensity,
and frequency. For persons who have been sedentary in
Physical Exercise
recent months, those with known cardiovascular disease or
A suitable exercise program is recommended for all sedentary
with grade III risk, and those aged Ͼ40 years, initial
persons; a clear and detailed prescription is needed for
training should be gentle (eg, 10 minutes of walking daily).
effectiveness, safety, and personal enjoyment.
As fitness and tolerance increase, the dose increases in
1934 Circulation November 2, 1999 Target Pulse Rate During Aerobic Exercise for Suggested Target Levels for LDL Persons not at High Cardiovascular Risk* Cholesterol Lowering*
*Until further information becomes available, a suggested target for triglyc-
*Rates listed are inappropriate for patients taking -blockers and other
eride lowering is 150 mg/dL (1.7 mmol/L).
Reproduced with permission from Nutr Metab Cardiovasc Dis. 1998;8:205–
Adapted from Nutr Metab Cardiovasc Dis. 1998;8:205–271 (also available at
271 (also available at http://www.chd-taskforce.com).
weekly increments, initially by extending the duration.
should know that current dietary guidelines fully maintain the
Later, intensity can be increased if suitable, eg, by brisk
pleasures of eating and are similar to the habitual diets of
walking or by alternating walking and jogging or gentle
countries in which mortality from CHD and many cancers is
swimming. Young persons and fit middle-aged subjects
far lower than in Western countries.
may ultimately undertake 20 to 30 minutes of aerobic
Lipid-lowering drugs should be introduced only after a
careful trial of conservative management, if indicated by the
Exercise intensity can be judged subjectively; persons
grade of risk, and always used together with ongoing dietary
should aim for a comfortable intensity, sufficient to extend
themselves slightly. Mild shortness of breath during exerciseshould abate within 4 minutes or less of resting. The subject
Target Levels for Lipid Lowering Table 4 shows suggested goals for lipid-lowering based on
should be told to stop and to report to a physician if recovery
the grade of global risk. Pending the results of further trials to
time is prolonged or if chest pain, syncope, or persistent
determine optimal goals, Table 4 is consistent with epidemi-
cough occur. Another way to judge intensity requires moni-
ological studies and with meta-analyses of trials. Treatment is
toring pulse rate during exercise; target pulse rates are shown
best monitored by LDL cholesterol levels.
in Table 3. A training effect is obtained at rates of 60% of the
History and physical examination may reveal the features
maximum rate for age, and this is the initial target rate. With
of major familial hyperlipidemias. Most are uncommon, but
increasing fitness, in persons at low cardiovascular risk, the
they require detection because they may confer a particularly
target may be increased gradually to 75% of maximum, for
high risk of CHD or pancreatitis. These disorders are tabu-
example, by increasing the speed of walking.
Exercise should be supervised, at least initially, and ECG
A determined effort should be made to reduce or correct
monitoring should be performed in patients at higher risk; this
even minor degrees of overweight using the means described
includes those with overt cardiovascular disease, such as
in the section on weight reduction together with those in the
angina or silent ischemia, and especially those with high-
section on exercise. These measures have a strong favorable
grade ventricular arrhythmias, low ejection fractions, hypo-
effect on most common plasma lipid disorders.
tension on exercise, and inappropriate exercise-induced
Causes of secondary hyperlipidemia should be treated or
tachycardia. The type and amount of exercise must also take
removed, if possible. Among these causes are medications,
into account respiratory or musculoskeletal disease and pe-
including corticosteroids, anabolic steroids, thiazides, and
retinoids; diabetes mellitus; hypothyroidism; alcohol abuse;
Treatment of Hyperlipidemia
chronic renal failure; nephrotic syndrome; and bulimia andanorexia nervosa.
Clinical trial evidence justifies placing a strong emphasis onplasma lipid-lowering as part of primary and secondary
Lipid-Lowering Diet
prevention. Accompanying risk factors are treated at the same
A lipid-lowering diet is shown in Appendix 2; it is designed
time. Past concerns about the safety of lowering plasma
for persons whose habitual diet is Western and requires
cholesterol are no longer tenable. The intensity of lipid-
adaptation. In the lipid-lowering diet, fat provides up to 30%
lowering treatment is determined by the patient’s global risk
of food energy; saturated plus hydrogenated fat contributes
and by his or her responsiveness to treatment.
no more than 7% to 10% of energy intake, monounsaturated
The value of conservative treatment, ie, diet (including the
fat 10% to 15%, and polyunsaturated fat up to 7% to 8%. The
extremely important element of reduction of overweight) and
diet has a high content of complex carbohydrates, and it
exercise, cannot be too strongly emphasized; under controlled
provides at least 25 g of fiber per day, with an emphasis on
conditions, diet even without weight reduction can lower
soluble fiber. It contains less than 300 mg of cholesterol per
plasma cholesterol by 10% to 25%. Hence, efforts should be
day. This is achieved with a generous intake of whole-grain
made to maximize skills in dietary counseling. The patient
cereal foods, fruit and vegetables, fat-free and low-fat dairy
Assmann et al Reducing Coronary Heart Disease 1935
products, fish, low-fat poultry, moderate amounts of low-fat
acid and several concomitantly administered drugs. In a
meats and of eggs, and unsaturated vegetable oils as the main
larger dose, resins can increase triglyceride levels.
source of fats. Preferred cooking methods include grilling,
Fibric acid derivatives are effective triglyceride-lowering
steaming, boiling, microwave cooking, and barbecue
drugs; they increase HDL cholesterol substantially and (par-
ticularly the more recent members of the class) also lower
Some patients whose response to this diet is incomplete will
plasma cholesterol. Abnormal liver function is a contraindi-
achieve satisfactory control when a diet is given that provides
cation. Side effects include dyspepsia, rashes, abnormal liver
25% to 27% of energy from fat (6% to 8% of which is from
function and (rarely) hepatitis (ALT should be monitored),
saturated fat) and 200 to 250 mg of cholesterol per day.
gallstones, impotence, myopathy and rhabdomyolysis, and
For patients with hypertriglyceridemia, the standard lipid-
sensitivity to warfarin. Great caution is needed in using
lowering diet is prescribed, with particular emphasis on
controlling overweight and specific advice on moderating or
Nicotinic acid in large doses lowers triglyceride and
avoiding alcohol consumption and increasing the intake of
cholesterol levels and increases HDL cholesterol. Flushing,
oily fish. Patients with severe hypertriglyceridemia caused by
pruritus, and dyspepsia are common and tend to limit com-
excess chylomicron particles need a minimal intake of long-
pliance; abnormal liver function may occur. A gradually
chain fatty acids but can substitute medium-chain
increasing dose schedule is needed. Liver disease, gout, and
diabetes are relative contraindications. Fish oil in large doses effectively lowers triglyceride
Lipid-Lowering Drugs
In patients at grade I risk, conservative treatment is usuallyeffective in achieving target lipid levels. In those at grade III
Management of Hypertension
risk, a short (eg, 2 month) trial of diet is warranted, during
The prevalence of hypertension is about 20% in most coun-
which at least 2 sets of lipid measurements should be made
tries, rising with age to about 50% by the age of 65 years. In
and averaged; if target values are not attained, a drug should
the US in 1988, the proportion of hypertensives who were
be introduced, with ongoing attention to diet. In those at
detected, treated, and achieved good control was 29%;
grade II risk, an extended trial of conservative treatment is
similarly limited success has been observed in Europe.1
required, with repeated counseling, for a period of at least 6
The usual goal of treatment is to achieve a systolic blood
months. Whenever possible, the use and choice of drug
pressure Ͻ140 mm Hg and a diastolic blood pressure
should be based on clinical trial data. A discussion of
Ͻ90 mm Hg. Particular care is directed to patients at highest
commonly used lipid-lowering drugs follows.
risk, including the elderly, those with target organ damage
Hepatic hydroxymethylglutaryl coenzyme A (HMG CoA)
(heart, brain, kidneys, and retina), diabetics, hyperlipidemics,
reductase inhibitors offer a major advance in CHD preven-
smokers, patients with left ventricular hypertrophy, and those
tion. They effectively lower LDL cholesterol, and they have
a moderate effect in lowering triglycerides, which may bemore marked with some newer statins. HMG CoA reductase
Nonpharmacological Treatment
inhibitors are now the drugs of first choice for familial
The following measures are appropriate in all hypertensives.
hypercholesterolemia, and they can be of value in combined
● Reduction of overweight; even a loss of 4 to 5 kg lowers
(mixed) hyperlipidemia. Treatment commences at a mini-
mum dosage, with dose titration at 6- to 8-week intervals.
● Reduction of alcohol intake, if excessive (ie, Ͼ30 mL/d),
Lipid levels and alanine transaminase (ALT) levels should be
lowers blood pressure in susceptible hypertensives
monitored. Severe hypercholesterolemia may require combi-
● Increase in aerobic physical activity
nation treatment with a resin. Most statins are not licensed for
● Reduction of salt intake to 4 g (70 mmol) per day
use in children, and they are not given to women of
● Increase intake of fruit and vegetables (which provides a
child-bearing age unless effective contraception is assured.
substantial intake of potassium) and lower intake of fat and
Headache, constipation, flatulence, and dyspepsia are recog-
saturated fat; these items are of proven value in lowering
nized side effects. Liver function can be impaired, and statins
are contraindicated in the presence of active liver disease or
● Deal with coexisting cardiovascular risk factors (eg, smok-
elevated ALT levels. Myopathy and potentially fatal rhabdo-
myolysis are rare side effects, the risk of which is increasedby drug interactions with erythromycin, fibrates, azole anti-
Drug Treatment
fungals, cyclosporin, tacrolimus, nicotinic acid, and some
Drug treatment commences with low doses followed by slow
dose titration to achieve 24-hour control with once-daily
Resins (bile acid sequestrants) are effective cholesterol-
medication at a minimum dosage. If systolic pressure
lowering drugs. Being nonabsorbable, they are largely free
Ͼ160 mm Hg and target organ damage are present, initiate
from systemic side effects. They are presented as a powder
drug treatment immediately; if diastolic pressure Ͼ90 mm Hg
and taken in water or fruit juice with meals. Patient accep-
and target organ damage are present, start drug treatment
tance is sometimes imperfect. Side effects include constipa-
within 1 to 2 weeks if a trial of nonpharmacological measures
tion, dyspepsia, abdominal pain, and malabsorption of folic
is not promptly effective. Conversely, if hypertension is mild
1936 Circulation November 2, 1999
and no target organ damage exists, a trial of nonpharmaco-
Suggested Target Lipid Levels in Diabetic Patients
logical management for up to 6 months is warranted. Avail-
able clinical trial data suggest that thiazides and -blockersare the preferred initial drugs for uncomplicated hyperten-
sives. Nonpharmacological measures are continued after the
Initial Drugs
Adapted from Nutr Metab Cardiovasc Dis. 1998;8:205–271 (also available at
Low-dose thiazides or -blockers should be the first drugs
used for pharmacological management of hypertension, un-less contraindicated. Angiotensin-converting enzyme (ACE)
trophy. They are generally well tolerated, but the first dose
inhibitors should be prescribed for patients with CHD and
may lower blood pressure excessively.
reduced ejection fraction, those with decreased left ventricu-
● Angiotensin II receptor (AT1) antagonists. These drugs
lar function due to other causes, diabetics with microalbu-
were introduced recently. They do not have adverse meta-
minuria or frank proteinuria, and those with impaired renal
bolic effects, do not cause cough or angioedema, and are
function and heavy proteinuria. For hypertensives who have
generally well tolerated. They can worsen renal function in
had an uncomplicated myocardial infarction, prescribe
patients with bilateral renal artery stenosis.
-blockers without intrinsic sympathomimetic activity. Forisolated systolic hypertension, prescribe a low dose of thia-
Cardiovascular Risk Reduction in Diabetes
zide, -blocker, ␣-blocker, or long-acting calcium-channel
In a trial of patients with type 1 diabetes (ie, insulin-
dependent diabetes), careful insulin therapy reduced micro-vascular complications, with a 60% (nonsignificant) reduc-
Subsequent Management
tion of macrovascular events. Although trial data in patients
If the blood pressure target is not achieved or if side effects
with type 2 diabetes are scanty, the consensus is that careful
occur, first try substituting a drug from another class. If
glycemic control is essential for minimizing diabetic compli-
unsuccessful, add a second drug from another class (eg, a
diuretic), if not already used, and, if problems still persist, add
are correcting overweight to improve control, particularly in
a third drug from another class or consider referral to a
type 2 diabetics; lowering blood pressure; and controlling
lipid abnormalities (Table 5). Frequent aerobic exercise
The following is a list of the most commonly used drugs.
facilitates glycemic control and weight control, as does a diet
similar to the lipid-lowering diet, but with no sugar other than
Thiazides. The use of thiazides is supported by controlled
that in fruit and saturated fat (Ͻ7%). Stopping smoking is
trial evidence. Low dosage (eg, hydrochlorothiazide 6.25
mg/d up to 12.5 mg/d) lessens the risk of metabolic side
Drug treatment may be commenced at the same time as the
effects such as potassium depletion, hyperlipidemia, hyper-
above measures in patients with severe metabolic abnormal-
uricemia, and worsening of glucose tolerance.
ities, CHD, or diabetic complications; in patients with mild
-blockers. Use of -blockers without intrinsic sympatho-
diabetes, it may be deferred pending the outcome of a 2- to
mimetic activity is supported by clinical trial data. Side
4-month trial of diet and exercise. Drug options include
effects include severe asthma in predisposed patients,
insulin, metformin, sulfonylureas, acarbose, and the new
worsening of intermittent claudication, aching of the legs,
cardiac failure, and an increased grade of heart block
Hypertriglyceridemia and low HDL cholesterol may be
(possibly less frequent with cardioselective and vasodilator
fully corrected by diabetic control and the measures listed
above. However, lipid-lowering drugs should be considered if
ACE inhibitors. The indications for the use of these drugs
hyperlipidemia persists; the main options are a statin if LDL
are listed above. Side effects include a cough. ACEinhibitors should be avoided in patients with bilateral renal
elevation predominates or a fibrate if triglycerides remain
artery stenosis (which should be suspected in patients with
elevated (the risk of fibrate myopathy is increased in the
peripheral vascular disease or abdominal aortic aneurysm),
presence of renal failure or diabetic nephropathy).
because renal failure may be precipitated. Management of Thrombogenic Risk Factors Calcium-channel blockers. Long-acting formulations of
To manage thrombogenic risk factors, health-related behavior
these drugs should be chosen because short-acting ones
is important. Such behavior includes the following.
have precipitated ischemic events. Evidence of reducedcardiovascular events was found in 1 trial using calcium-
channel blockers for systolic hypertension in the elderly.
These drugs do not have metabolic side effects, but other
untoward effects include headache and dependent edema.
● Increased intake of polyunsaturated fatty acids from the
● ␣-blockers. These drugs are useful in older patients with
omega-6 and omega-3 classes (from seed oils and oily fish)
systolic hypertension; they have a small favorable effect onplasma lipids and lipoproteins, do not worsen glucose
Drug therapy can also be used. The 3 main drugs used and
tolerance, and lessen symptoms of benign prostatic hyper-
their doses are as follows. Acetylsalicylic acid (75 to 160 mg
Assmann et al Reducing Coronary Heart Disease 1937
per day), preferably enteric-coated, is often used; the risk of
(HDL cholesterol in mg/dLϫϪ0.045)ϩ(log [triglyceride level in
gastrointestinal bleeding is least with lower dosages. Ticlo-
mg/dL]ϫ0.3346)ϩ(smoking behavior [noϭ0, yesϭ1]ϫ0.9266)ϩ
pidine (250 mg per day) is an alternative; it does carry a risk
(diabetes mellitus [noϭ0, yesϭ1]ϫ0.4015)ϩ(positive family historyof myocardial infarction [noϭ0, yesϭ1]ϫ0.4193)ϩ(angina pectoris
of neutropenia, so monitoring white cell count is important.
Clopidogrel (75 mg per day) may be more effective than
This algorithm was derived from a population of white men aged
acetylsalicylic acid, and warfarin dosage should be adjusted
35 to 65 years and, therefore, its applicability to women, men outside
to maintain an International Normalized Ratio (INR) in the
this age range, and other ethnic groups has yet to be established. The
output of the PROCAM algorithm is expressed as the risk of acoronary event (definite fatal myocardial infarction, definite nonfatalmyocardial infarction, or sudden coronary death) in percentage over
CHD Prevention in the Elderly
8 years. In the German population of middle-aged men, the output of
After the age of 60 years, risk factors such as plasma
the algorithm may be divided into quintiles with the following
cholesterol, systolic blood pressure, smoking, and low HDL
cut-off points: first quintile, Յ0.91% in 8 years (Յ0.11% per
cholesterol confer an increased absolute risk of CHD to at
annum); second quintile, 0.92% to 1.40% in 8 years (0.12% to 0.18%
least the same extent as in younger persons. Clinical trial data
per annum); third quintile, 1.41% to 3.65% in 8 years (0.18% to0.46% per annum); fourth quintile, 3.66% to 7.60% in 8 years
on risk factor reduction in older persons are few, but some
(0.46% to 0.95% per annum); and fifth quintile, Ͼ7.60% in 8 years
evidence exists that cholesterol lowering by diet or by statin
Risk factor reduction is appropriate in older persons in
Appendix 2
good general health who have reasonable life expectancy andthe capacity to enjoy life. Diets must take eating difficulties,
Recommended Foods
food preferences, and nutritional soundness into account.
The following foods may be given as generous helpings in meals
Drug interactions are of particular concern, and untoward
(preferably as a first course) or as snacks. Table 2 has a morecomplete list.
effects can be sources of difficulty.
Low-calorie vegetables (fresh or frozen, not canned); use cooked, in
salad, and as crudite´s. These include: artichokes, asparagus,
CHD Prevention in Postmenopausal Women
cabbage, cauliflower, carrot, celery, chicory, cress, cucumber,
Most CHD risk factors operate in both sexes. In women,
eggplant, endive, French (green) beans, green pepper, leek, let-
plasma cholesterol, low HDL cholesterol, and blood pressure
tuce, marrow, mushroom, onion (boiled), pumpkin (boiled), rad-
are related to risk; diabetes, triglyceride levels, and cigarette
Soup: broth, consomme´, and other clear soups.
smoking confer greater risks than in men. Limited data from
Beverages: coffee or tea with skim milk, sugar-free soft drinks, and
clinical trials in women suggest that cholesterol lowering
mineral water; use aspartame and saccharine as sweeteners.
lowers CHD incidence and promotes regression of coronaryartery disease. Foods Permitted in Controlled Quantities
Estrogen replacement therapy lowers LDL cholesterol and
The following foods are permitted in controlled quantities.
increases HDL cholesterol, effects that are attenuated by
those progestogens that have androgenic activity. Progesto-
Vegetables: 1 small boiled or baked potato. Cereal foods: 5 U per day. 1 Uϭ1 thin slice of wholemeal bread cut
gens such as medroxyprogesterone have only small effects in
from a large loaf, 1 cup of sugar-free breakfast cereal, 1⁄2-cup
reducing the favorable influence of estrogens. Many obser-
vational studies suggest that postmenopausal estrogen re-
Fish, chicken, turkey, very lean meat: 120 to 180 g per day.
placement may reduce CHD incidence,2 but such data are
Dairy foods: 2 U per day. 1 Uϭ1 cup skim milk, 1⁄2-cup low-fat milk,
inconclusive and controlled trial evidence is needed to clarify
1 cup very-low-fat yogurt without added sugar, 30 g of skim
milk– based cottage cheese, or 30 g of fat-free fromage frais; 2eggs per week are allowed.
Legumes (pulses): 1⁄2-cup serving, 3 to 4 times per week. These
Appendix 1
include boiled lentils, mung beans, chick peas, butter beans,
The multiple logistic function from PROCAM has the form:
Oils and fats: 10 g (2 to 3 teaspoons) per day. These include olive oil,
canola oil, corn oil, and sunflower oil, plus 10 g per day of
where yϭϪ12.3199ϩ(age in yearsϫ0.1001)ϩ(systolic blood pres-
sure in mm Hgϫ0.0118)ϩ(LDL cholesterol in mg/dLϫ0.0152)ϩ
1 cupϭ200 mLϭ7 fluid ounces; 30 gϭ1 ounce
1938 Circulation November 2, 1999 Appendix 3 Classification of the Primary Hyperlipidemias
CHD indicates coronary heart disease; HDL, high density lipoprotein; IDL, intermediate density lipoprotein; PVD, peripheral vascular disease; VLDL, very low density
lipoprotein; ϩ, slight to moderate increase; ϩϩ, moderate to marked increase; and ϩϩϩ, marked to extreme increase.
*Depending on which lipoprotein class is present in excess, the primary hyperlipidemias may manifest as predominantly elevated levels of cholesterol or of
triglyceride, or both lipids may be involved (see below).
†The prevalence of genetic hyperlipidemias varies from population due to
genetic drift, founder effects, and selection bias. The data shown in Appendix2 apply to most Caucasian populations.
Reproduced with permission from Nutr Metab Cardiovasc Dis. 1998;8:205–
271 (also available at http:///www.chd-taskforce.com). References
1. Brown MS, Goldstein JL. Drugs used in treatment of hyperlipopro-
teinemias. In: Gilman AG, Rall TW, Nies AS, Taylor P, eds. Goodmanand Gilman’s The Pharmacological Basis of Therapeutics. 8th ed. NewYork: McGraw-Hill; 1990:874.
2. Assmann G, Schulte H, von Eckardstein A. Hypertriglyceridemia and
elevated levels of lipoprotein (a) are risk factors for major coronaryevents in middle-aged men. Am J Cardiol. 1996;74:1179 –1184.
KEY WORDS: cardiovascular diseases Ⅲ risk factors Ⅲ hyperlipidemia
Overview of Treatments for Obsessive- Compulsive Disorder and Spectrum Conditions: Conceptualization, Theory, and Practice Nicholas Maltby, PhD David F. Tolin, PhD This paper presents an overview of obsessive-compulsive disorder (OCD) and theobsessive-compulsive spectrum disorders (OCSDs) by outlining the major arguments for and against the spectrum construct. Cognitive, behavioral, and
BSA Health and Medical Record 1. Complete Scout’s Last name/ Date of Birth/Allergies and emergency contact phone number (side of form). 2. Part A which includes general information (Social Security Number is Optional), Unit Leader (Ed Davey), Council name (HOAC), Health insurance company & policy number, emergency contact & alternate emergency contact information, medical history, allerg
 1932
1932