Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
Acquired pelger–huët anomaly associated with ibuprofen therapy
Clinica Chimica Acta xxx (2009) xxx–xxx
j o u r n a l h o m e p a g e : w w w. e l s ev i e r. c o m / l o c a t e / c l i n c h i m
Acquired Pelger–Huët anomaly associated with ibuprofen therapy
and basophils carry chromatin hypercondensation The secondsuggests that pseudo PHA is not actually an abnormality in neutrophilmaturation but represents an apoptotic cell, since ultrastructurally
pseudo PHA neutrophils looked like mature cells undergoing apoptosis(compact chromatine moved toward the periphery of the nucleus and
Pelger–Huët anomaly (PHA) is a benign inherited condition
condensation of the cytoplasm with abnormally shaped organelles)
characterized by hyposegmentation of the neutrophils nucleus and
The third hypothesis suggests that pseudo PHA is related to 17p
excessive chromatin clumping An acquired neutrophils dysplasia
similar to PHA has been already described in hematological diseases
A careful review of the pertinent literature revealed that almost all
and in some clinical conditions, especially under certain drugs
reports of pseudo PHA associated to either drugs use or to several
effect It has been known as acquired or pseudo Pelger–Huët
diseases were described until middle of 1980. To date, almost all
anomaly. A previous report of our group showed that the incidence of
reported cases are associated to either myelodysplastic syndrome or
acquired PHA in kidney transplanted patients under immunosuppres-
other hematological diseases as well as to use of immunosuppressive
sive therapy in a local Brazilian Hospital was 5.3% (9 out of 170 patients)
Curiously, automated hematological procedures including differen-
In March 2008, a healthy 7-year old child was punctioned in a small
tial leukocytes counting were widely diffused from end of the 1980s.
laboratory in Mateus Leme/MG for a routine hemogram analysis. Her
This fact raises an important question “Can automatic cell blood
blood cells showed to be normal under quantitative and qualitative
counters reveal neutrophils' morphological changes consistent to PHA
points of view. Two months later, this child had fever, without other
such as abnormal bilobular or monolobular nuclear forms and excessive
symptoms and 17 drops of ibuprofen was given to her, from 4 to 4 h
chromatin clumping?” PHA whichever its cause, if it is not registered by
during 1 day and night. Next day, as the girl's condition became worse,
automated counters may constitute a serious problem considering that
she was conducted to the same laboratory for another routine blood
clinical laboratories do not examine most of stained blood films on the
analysis. This dose (510 mg/24 h) was >12 times higher than that
recommended (40 mg/24 h). The leukocytes count was 12,500/μL with
The contribution of this report is to alert laboratory professionals and
22% band form neutrophils, 50% segmented neutrophils, 20% lympho-
clinicians for pseudo PHA diagnosis. Considering previous reports and
cytes and 8% monocytes, erythrocyte sedimentation rate (60 min.) was
our own experience, in addition to the frequent use of drugs with no
6 mm and Reactive C Protein was negative. However, blood film
clinical prescription (automedication), one can admit that other cases
revealed that segmented neutrophils nucleus had a poor segmentation,
similar to that one reported here due to administration of ibuprofen (or
with only bilobular nuclear form or peanut shaped and the chromatin
other drugs) in high doses may be occurring frequently. Whether this
was excessively clumped a, b, c and d). Later on a more
phenomenon has clinical implication remains to be elucidated. At least,
experienced observer has diagnosed the child as a carrier of PHA. Since
however, when pseudo PHA is described, its possible cause must be
there was a normal blood analysis reported 2 months ago, the
hypothesis of benign inherited PHA was discharged. The apparent
Finally, considering that acquired PHA is a common finding in
neutrophils' shift left (22% band forms) was not coherent with the
myelodysplastic syndrome a doubt may be about a predisposition
child's symptoms, she only had fever once, with no infection symptoms.
for developing bone marrow diseases in individuals who showed these
Five days later, a new blood analysis was done and the total leukocytes
neutrophils under certain conditions. However, no report regarding this
were 5300/μL persisting 21% of band neutrophils. Six months later, the
issue was found in the literature and a follow up of these individuals is
child had fever again and other blood analysis was required. The
essential to elucidate this important question.
leukocytes count was 17,700/μL and 5% band neutrophils (withoutalterations), 54% segmented neutrophils, 32% lymphocytes, 2% mono-
cytes and 7% eosinophils ) was found, which confirm thetransitory character of neutrophil abnormalities observed when the
The authors thank FAPEMIG and CNPq/Brazil. LMSD and MGC are
child was under ibuprofen use. All data are shown in . It was not
grateful to CNPq Research Fellowship (PQ).
suspected that this case of transitory neutrophil abnormalities wascaused by ibuprofen, since it was the only drug that the child had
received. Only one report on ibuprofen use and pseudo PHA haspreviously been described
[1] Johnson CA, Cass DA, Trillo AA, Snyder MS, Dechatelet LR. Functional and metabolic
Although some hypotheses were raised to explain this phenomen,
studies of polymorphonuclear leukocytes in the congenital Pelger–Huët anomaly. Blood 1980;55:466–9.
the mechanism of nuclear change is still unclear. The first hyphothesis is
[2] Shetty VT, Mundle SD, Raza A. Pseudo anomalia de Pelger–Huët anomaly in
related to abnormalities in the sequence of lamin B receptor (LBR) gene
myelodysplastic syndrome: hyposegmented or apoptotic neutrophil? Blood
resulting in a lack of LBR protein. This protein is essential for chromatin
[3] Kuriyama K, Tomonaga M, Matsuo T. Diagnostic significance of detecting pseudo
binding to nuclear membrane. In the absence of LBR, neutrophils and
Pelger–Huët anomalies and micro-megakaryocytes in myelodysplastic syndrome.
also erythroblasts, monocytes, lymphocytes, plasma cells, eosinophils
0009-8981/$ – see front matter 2009 Elsevier B.V. All rights reserved. doi:
Please cite this article as: Moreira AMB, et al, Acquired Pelger–Huët anomaly associated with ibuprofen therapy, Clin Chim Acta (2009),doi:
Fig. 1. Neutrophils with chromatin excessively clumped. a) Segmented neutrophil b, c) band forms neutrophils d) neutrophil with rodlike nucleus. e) Segmented neutrophils with noabnormalities.
[11] Deutsch PH, Mandell GL. Reversible Pelger
ibuprofen therapy. Arch Intern Med 1985;145(1):166.
Laboratorial results at different occasions.
[12] Best S, Salvati F, Kallo J, Garner C, Height S, Thein SL, et al. Lamin B-receptor mutations
in Pelger–Huët anomaly. Br J Haematol 2003;123(3):542–4.
[13] Tomonaga M. Nuclear abnormalities in Pelger
cell morphology. Rinsho Byori 2005;52(1):54–60.
[14] Soenen V, Preudhomme C, Roumier C, Daudignon A, Laï JL, Fenaux P. 17p Deletion
in acute myeloid leukemia and myelodysplastic syndrome. Analysis of break-
points and deleted segments by fluorescence in situ. Blood 1998;91:1008–15.
[15] Cunningham JM, Patnaik MM, Hammerschmidt DE, Vercellotti GM. Historical
perspective and clinical implications of the Pelger–Huët cell. Am J Hematol2009;84:116
[4] Daliphard S, Accard F, Delattre C, Toupance D, Guyot C, Méchinaud F, et al. Reversible
Clinical and Toxicological Analysis Department, Faculty of Pharmacy,
abnormal chromatin clumping in granulocytes from six transplant patients treatedwith mycophenolate mofetil: a rare adverse effect mimicking abnormal chromatin
Federal University of Minas Gerais, Brazil
clumping syndrome. Br J Haematol 2002;116(3):726–7.
⁎Corresponding author. Faculdade de Farmácia,
[5] Gondo H, Okamura C, Osaki K, Asano Y, Okamura T. Acquired Pelger–Hüet anomaly in
Universidade Federal de Minas Gerais, Sala 4104-B3,
association with concomitant tacrolimus and fluconazol therapy following allogeneicbone marrow transplantation. Bone Marrow Transplant 2000;26:1255–7.
Av. Antônio Carlos, 6627, Campus Pampulha,
[6] Juneja SK, Matthews JP, Luzinat R, Fan Y, Michael M, Rischin D, et al. Association of
Belo Horizonte/Minas Gerais CEP: 31270-901, Brazil.
acquired Pelger–Huët anomaly with taxoid therapy. Br J Haematol 1996;93:139–41.
Tel.: +55 31 3409 6880; fax: +55 31 3409 6985.
[7] Kaplan JM, Barrett Jr O. Reversible pseudo anomalia de Pelger anomaly related to
sulfisoxazole therapy. N Engl J Med 1967;277:421–2.
[8] May RB, Sunder TR. Hematologic manifestations of long-term valproate therapy.
[9] Oka Y, Kameoka J, Hirabayashi Y, Takahashi R, Ishii T, Sasaki T, et al. Reversible
bone marrow dysplasia in patients with systemic lupus erythematosus. Inter Med2008;47:737–42.
[10] Dusse LM, Morais RMS, Freitas VM, Medeiros GM, Vieira LM, Carvalho MG. Pseudo
Pelger–Huët in transplanted patients. Acta Haematologica 2006;116:272–4.
Please cite this article as: Moreira AMB, et al, Acquired Pelger–Huët anomaly associated with ibuprofen therapy, Clin Chim Acta (2009),do
Afssa – Saisine n° 2008-SA-0047 de l’Agence française de sécurité sanitaire des aliments relatif à la contamination de céréales destinées à l'alimentation humaine par de L’Agence française de sécurité sanitaire des aliments (Afssa) a été saisie le 29 février 2008 par la Direction Générale de la concurrence, de la consommation et de la répression des f

 Clinica Chimica Acta xxx (2009) xxx–xxx
j o u r n a l h o m e p a g e : w w w. e l s ev i e r. c o m / l o c a t e / c l i n c h i m
Acquired Pelger–Huët anomaly associated with ibuprofen therapy
and basophils carry chromatin hypercondensation The secondsuggests that pseudo PHA is not actually an abnormality in neutrophilmaturation but represents an apoptotic cell, since ultrastructurally
pseudo PHA neutrophils looked like mature cells undergoing apoptosis(compact chromatine moved toward the periphery of the nucleus and
Pelger–Huët anomaly (PHA) is a benign inherited condition
condensation of the cytoplasm with abnormally shaped organelles)
characterized by hyposegmentation of the neutrophils nucleus and
The third hypothesis suggests that pseudo PHA is related to 17p
excessive chromatin clumping An acquired neutrophils dysplasia
similar to PHA has been already described in hematological diseases
A careful review of the pertinent literature revealed that almost all
and in some clinical conditions, especially under certain drugs
reports of pseudo PHA associated to either drugs use or to several
effect It has been known as acquired or pseudo Pelger–Huët
diseases were described until middle of 1980. To date, almost all
anomaly. A previous report of our group showed that the incidence of
reported cases are associated to either myelodysplastic syndrome or
acquired PHA in kidney transplanted patients under immunosuppres-
other hematological diseases as well as to use of immunosuppressive
sive therapy in a local Brazilian Hospital was 5.3% (9 out of 170 patients)
Curiously, automated hematological procedures including differen-
In March 2008, a healthy 7-year old child was punctioned in a small
tial leukocytes counting were widely diffused from end of the 1980s.
Clinica Chimica Acta xxx (2009) xxx–xxx
j o u r n a l h o m e p a g e : w w w. e l s ev i e r. c o m / l o c a t e / c l i n c h i m
Acquired Pelger–Huët anomaly associated with ibuprofen therapy
and basophils carry chromatin hypercondensation The secondsuggests that pseudo PHA is not actually an abnormality in neutrophilmaturation but represents an apoptotic cell, since ultrastructurally
pseudo PHA neutrophils looked like mature cells undergoing apoptosis(compact chromatine moved toward the periphery of the nucleus and
Pelger–Huët anomaly (PHA) is a benign inherited condition
condensation of the cytoplasm with abnormally shaped organelles)
characterized by hyposegmentation of the neutrophils nucleus and
The third hypothesis suggests that pseudo PHA is related to 17p
excessive chromatin clumping An acquired neutrophils dysplasia
similar to PHA has been already described in hematological diseases
A careful review of the pertinent literature revealed that almost all
and in some clinical conditions, especially under certain drugs
reports of pseudo PHA associated to either drugs use or to several
effect It has been known as acquired or pseudo Pelger–Huët
diseases were described until middle of 1980. To date, almost all
anomaly. A previous report of our group showed that the incidence of
reported cases are associated to either myelodysplastic syndrome or
acquired PHA in kidney transplanted patients under immunosuppres-
other hematological diseases as well as to use of immunosuppressive
sive therapy in a local Brazilian Hospital was 5.3% (9 out of 170 patients)
Curiously, automated hematological procedures including differen-
In March 2008, a healthy 7-year old child was punctioned in a small
tial leukocytes counting were widely diffused from end of the 1980s.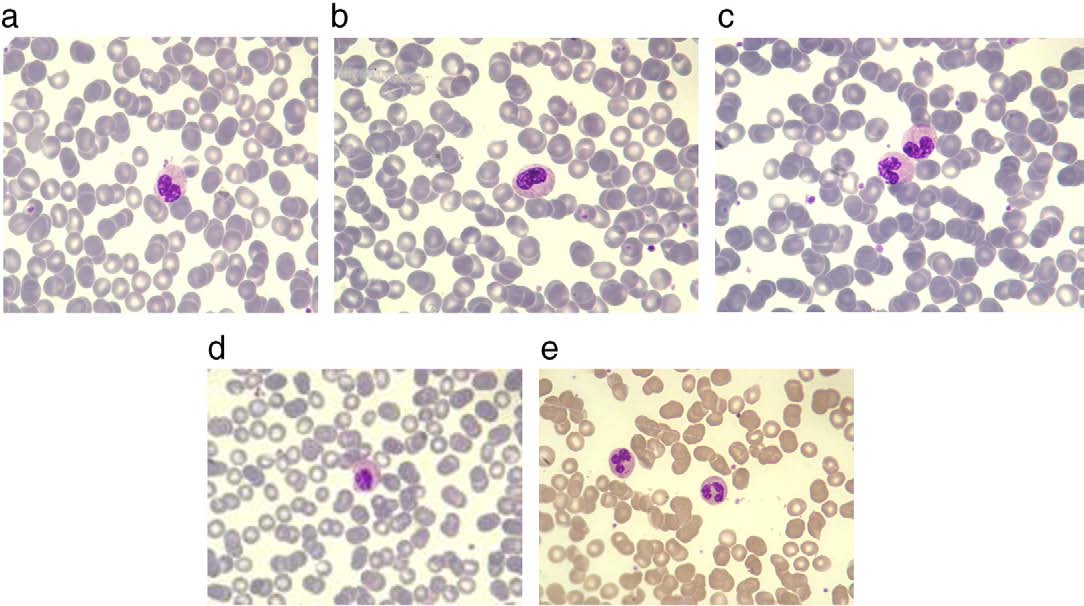 Fig. 1. Neutrophils with chromatin excessively clumped. a) Segmented neutrophil b, c) band forms neutrophils d) neutrophil with rodlike nucleus. e) Segmented neutrophils with noabnormalities.
Fig. 1. Neutrophils with chromatin excessively clumped. a) Segmented neutrophil b, c) band forms neutrophils d) neutrophil with rodlike nucleus. e) Segmented neutrophils with noabnormalities.