Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
Links.cenegenics.com
Low Serum Testosterone and Estradiol Predict Mortality in Elderly Men
Åsa Tivesten, Liesbeth Vandenput, Fernand Labrie, Magnus K. Karlsson, O¨sten Ljunggren,Dan Mellstro¨m, and Claes Ohlsson
The Wallenberg Laboratory for Cardiovascular Research (A.T.), Institute of Medicine, Sahlgrenska Academy, and Center forBone Research at the Sahlgrenska Academy (L.V., D.M., C.O.), Departments of Internal Medicine and Geriatrics,University of Gothenburg, S-413 45 Gothenburg, Sweden; Laboratory of Molecular Endocrinology and Oncology (F.L.),Laval University Hospital Research Center and Laval University, Que´bec, Canada G5Y 0H1; Clinical and MolecularOsteoporosis Research Unit (M.K.K.), Department of Clinical Sciences, Lund University, S-221 00 Lund, Sweden;Department of Orthopaedics (M.K.K.), Malmo¨ University Hospital, SE-205 02 Malmo¨, Sweden; and Department ofMedical Sciences (O.L.), University of Uppsala, SE-751 05 Uppsala, Sweden
Context: Age-related reduction of serum testosterone may contribute to the signs and symptoms of aging, but previous studies report conflicting evidence about testosterone levels and male mortality. No large prospective cohort study has determined a possible association between serum estradiol and mortality in men. Objective: The main objective was to examine the association between serum testosterone and estradiol and all-cause mortality in elderly men. Design, Setting, and Participants: We used specific gas chromatography-mass spectrometry to analyze serum sex steroids at baseline in older men who participated in the prospective population- based MrOS Sweden cohort (n ϭ 3014; mean age, 75 yr; range, 69 – 80 yr). Main Outcome Measure: All-cause mortality by serum testosterone and estradiol levels. Results: During a mean follow-up period of 4.5 yr, 383 deaths occurred. In multivariate hazards regression models, low levels (within quartile 1 vs. quartiles 2– 4) of both testosterone [hazard ratio (HR), 1.65; 95% confidence interval (CI), 1.29 –2.12] and estradiol (HR, 1.54; 95% CI, 1.22–1.95) associated with mortality. A model including both hormones showed that both low testosterone (HR, 1.46; 95% CI, 1.11–1.92) and estradiol (HR, 1.33; 95% CI, 1.02–1.73) predicted mortality. Risk of death nearly doubled (HR, 1.96; 95% CI, 1.46 –2.62) in subjects with low levels of both testos- terone and estradiol compared with subjects within quartiles 2– 4 of both hormones. Conclusions: Elderly men with low serum testosterone and estradiol have increased risk of mor- tality, and subjects with low values of both testosterone and estradiol have the highest risk of mortality. (J Clin Endocrinol Metab 94: 2482–2488, 2009) Testosteronegraduallydeclinesasmenage(1).Astestoster- tosterone associates with increased fat mass, an adverse meta-
one has important physiological effects on, for example,
bolic risk profile, and atherosclerosis (1, 5).
muscle, bone, fat mass, and brain in men, decreased testosterone
Recently, much interest has focused on testosterone supple-
levels may contribute to the symptoms and signs of aging, e.g.
mentation in elderly men (1), as evidenced by a 20-fold increase
decreased muscle mass and strength, impaired physical perfor-
in testosterone sales in the United States during the 1990s (6).
mance and cognitive function, and lack of energy (1). Men with
However, few large controlled studies demonstrate the efficacy
low serum testosterone are at increased risk of falls, low bone
and long-term safety of testosterone therapy (1, 7). Furthermore,
mineral density, and fractures (2– 4). Moreover, low serum tes-
testosterone supplementation has increased, despite relatively
Abbreviations: BMI, Body mass index; CI, confidence interval; CV, coefficient of variation;
CVD, cardiovascular disease; GC-MS, gas chromatography-mass spectrometry; HR, hazard
Copyright 2009 by The Endocrine Society
doi: 10.1210/jc.2008-2650 Received December 4, 2008. Accepted April 21, 2009. First Published Online April 28, 2009
J Clin Endocrinol Metab, July 2009, 94(7):2482–2488
J Clin Endocrinol Metab, July 2009, 94(7):2482–2488
few studies linking androgen deficiency in the elderly to health-
ical diagnosis (diabetes, cancer, stroke, myocardial infarction, or angina
related outcomes, including mortality.
pectoris) by a doctor. This study defined prevalent cardiovascular disease
Circulating estradiol levels in men are low but measurable,
(CVD) as a history of stroke, myocardial infarction, and/or angina pec-
exceeding the levels found in postmenopausal women. Because
toris. Physical activity was the subject’s estimation of average total dailywalking distance, including walking both as a means of exercise and leisure
approximately 80% of circulating estradiol in men derives from
and as a means of outdoor transportation in activities of daily life. We used
androgens (1), serum levels of estradiol and testosterone are sig-
standard equipment to measure height and weight (2), and calculated body
nificantly associated (2). Studies investigating aromatase or es-
mass index (BMI) as weight (in kilograms)/ height (meters)2.
trogen receptor deficiency in males demonstrated that estradiolhas important physiological effects on bone maturation and peak
Serum analyses
bone mass in younger men (8, 9). The role of estradiol in elderlymen remains more unclear, and few studies have explored the
We used a validated GC-MS system (21, 22) to analyze testosterone
[detection limit, 0.05 ng/ml; intraassay coefficient of variation (CV),
relationship between estradiol levels in elderly men and health-
2.9%; interassay CV, 3.4%] and estradiol (detection limit, 2.00 pg/ml;
related outcomes. However, our earlier study in the Swedish
intraassay CV, 1.5%; interassay CV, 2.7%) in baseline serum samples
Osteoporotic Fractures in Men (MrOS) cohort showed that low
(2). The blood specimens from the Go¨teborg cohort and the major part
serum estradiol associates with an increased risk of fractures (2).
of the Uppsala and Malmo¨ cohorts were obtained between 0800 and
Among the investigations that assessed the relationship be-
0830 h, but some of the specimens from the Uppsala and Malmo¨ cohorts
tween serum testosterone and mortality in men (6, 10 –15), only
were obtained between 1230 and 1330 h (approximately 31% of the
three were large prospective population-based cohort studies (6,
total number of serum samples included in the present analysis wereobtained between 1230 and 1330 h). An HP5973 quadrupole mass spec-
12, 13). One study showed an association between low serum
trometer equipped with a chemical ionization source detected analytes
testosterone and mortality in older men (6), whereas two studies
and internal standards. Twenty-six subjects had serum estradiol levels
in middle-aged men reported no similar association (12, 13).
that were below the lower limit of detection. We used immunoradio-
Currently, no large prospective study has determined a possible
metric assay (Orion Diagnostics, Espoo, Finland; detection limit, 1.3
association between serum estradiol and mortality in men.
nmol/liter; intraassay CV, 3%; interassay CV, 7%) to measure serum
Immunoassay-based techniques provide questionable speci-
SHBG. We calculated free testosterone and free estradiol according to the
ficity for measuring sex steroids, especially at low hormone con-
method described by Vermeulen et al. (23) and van den Beld et al. (24),taking concentrations of total testosterone, total estradiol, and SHBG
centrations (16, 17). Indeed, the use of such techniques may
into account and assuming a fixed albumin concentration (43 g/liter). All
contribute to the disparate results of previous studies and also to
samples were analyzed in one laboratory.
the paucity of studies on estradiol and clinical outcomes in men. No previous mortality study has used the reference method massspectrometry to assess sex steroids (18). Assessment of mortality
This prospective study investigated a possible link between
We collected mortality data from the population statistics at Statistics
serum testosterone and estradiol levels, assessed by gas chroma-
Sweden and recorded follow-up time as the period between baseline visit(in 2004) and date of death or mortality data collection (March 1, 2008).
tography-mass spectrometry (GC-MS), and all-cause mortality
Cause of death data were collected from the Swedish Cause of Death
in the MrOS Study in Sweden, a large population-based cohort
Register, held by the National Board of Health and Welfare in Sweden,
in which all deaths in Sweden are registered with International Classi-fication of Diseases (ICD) codes, based on the information from deathcertificates. The data were collected from this register from the study startuntil the last update of the register on December 31, 2005 and from eval-
Subjects and Methods
uation of copies of death certificates for deaths occurring after this date. Based on the information from the register/death certificate, the underlying
Study population
death cause was determined for each subject. The death causes were then
The multicenter MrOS Study includes older men in Sweden, Hong
classified as CVD (ICD-10 codes I00 to I99) or other (non-CVD).
Kong, and the United States. In Sweden, MrOS (n ϭ 3014) comprisesthree subcohorts in three different cities: Malmo¨ (n ϭ 1,005), Go¨teborg(n ϭ 1,010), and Uppsala (n ϭ 999). Study subjects (men aged 69 – 80 yr)
Statistical analysis
were selected randomly from national population registers (19). Eligi-bility for study participation required the ability to walk unassisted,
We used Cox proportional hazards regression to analyze the associ-
provide self-reported data, and understand and sign an informed con-
ations between serum sex steroids and mortality outcomes. Sex steroid
sent; 45% of those contacted participated in the study. The MrOS Study
levels were examined as quartiles based on the entire population or as
in Sweden was approved by the ethics committees at Go¨teborg, Lund,
dichotomous variables comparing quartile 1 to quartiles 2– 4. We also
show the effect estimate for a 1 SD increase (z score) of log-transformed
We investigated here the associations between serum sex steroids and
sex steroid levels. We adjusted all estimates for age and MrOS site and
mortality in the Swedish MrOS cohort. Levels of SHBG were available
made further adjustments for BMI (log-transformed), current smoking
for 97% of the entire cohort, and serum samples for sex steroid levels
(yes/no), and physical activity (kilometers walked per day, entered as
assessed by GC-MS (1 ml required) were available from 99% of the
quartiles because of a nonnormal distribution).
subjects in the Go¨teborg cohort, 96% in the Malmo¨ cohort, and 68% in
Unadjusted Kaplan-Meier survival curves illustrated the association
between testosterone and estradiol status (quartile 1 vs. quartiles 2– 4)and all-cause mortality, and the log-rank test assessed statistical signif-
Assessment of covariates
icance. Spearman rank correlation assessed the univariate association
We used a standardized questionnaire (20) to gather information
between serum testosterone and estradiol. We performed statistical anal-
about smoking habits and physical activity as well as self-reported med-
yses with SPSS for Windows, version 13.0 (SPSS, Chicago, IL).
Testosterone, Estradiol, and Male Mortality
J Clin Endocrinol Metab, July 2009, 94(7):2482–2488
spectively (Table 2, model 1, adjusted for age). Further adjust-
TABLE 1. Characteristics of study subjects
ment for age and BMI (model 2) as well as age, BMI, physical
Variable
activity, and smoking (model 3) showed no major influence on
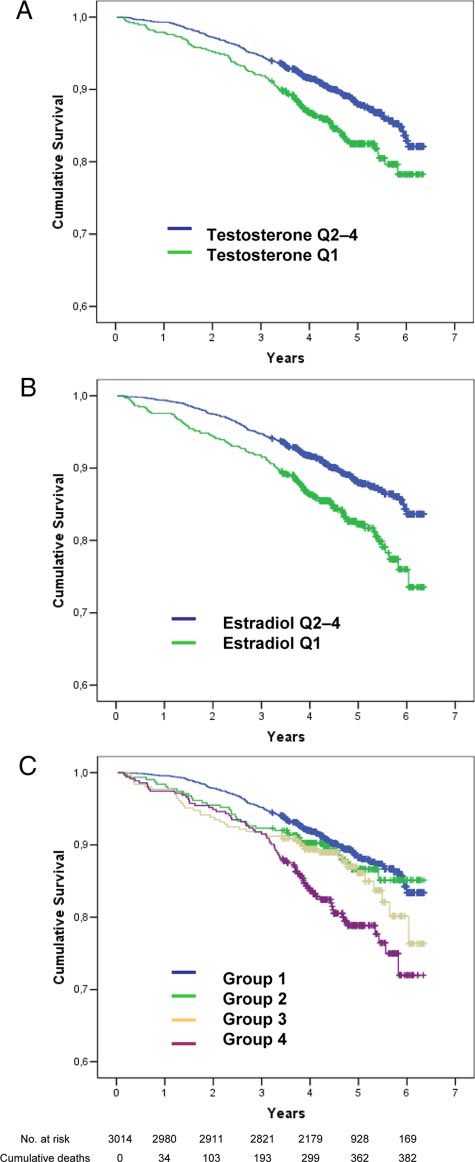
mortality risk at low sex steroid levels (Table 2). Cumulative
survival curves (Fig. 1) illustrate that subjects in the lowest quar-
tile of testosterone (Fig. 1A) and estradiol (Fig. 1B) levels had
higher all-cause mortality compared with subjects in quartiles
Serum levels of total estradiol and testosterone were associated
with each other (Spearman rank correlation coefficient 0.54; P Ͻ
0.001), as were the corresponding free hormone levels (0.62; P Ͻ
0.001). To study whether low testosterone and estradiol levels in-
dependently predict total mortality, we entered both low estradiol
(quartile 1 vs. quartiles 2– 4) and low testosterone (quartile 1 vs.
quartiles 2– 4) in the same hazards regression analyses (Table 2,models 1–3). Low levels of both testosterone and estradiol inde-
Values are given as mean (SD) unless otherwise indicated.
pendently predicted all-cause mortality in these models (Table 2).
To illustrate further the impact of low estradiol and/or testos-
terone levels, we divided subjects into four groups according to both
Table 1 shows the baseline characteristics of the MrOS Sweden
estradiol and testosterone status: group 1 (referent), with medium/
cohort (n ϭ 3014). SHBG data (assessed by RIA) and serum sex
high (ϭ within quartiles 2– 4) testosterone and estradiol levels
steroids (assessed by GC-MS) were available for 2925 and 2639
(n ϭ 1667); group 2, with low (ϭ within quartile 1) testosterone
subjects, respectively. The mean follow-up period was 4.5 yr,
but medium/high estradiol levels (n ϭ 312); group 3, with low
and the study included 13,527 person-years of follow-up. Dur-
estradiol but medium/high testosterone levels (n ϭ 307); and
ing the follow-up period, 383 persons (12.7%) died, yielding a
group 4, with low levels of both testosterone and estradiol (n ϭ
mortality rate of 28.3 per 1000 person-years at risk. Because
353). Risk of death approximately doubled [HR, 1.96 (95% CI,
cause of death certificates were missing for 20 of the men who
1.46 –2.62); model 3, adjusted for age, BMI, physical activity,
died during the follow-up, death cause was determined for 363
and smoking] in subjects with low levels of both testosterone and
men; 144 (39.7%) of these deaths were due to CVD.
estradiol (group 4) compared with subjects within group 1. In
Low physical activity [hazard ratio (HR), 0.88; 95% confi-
contrast, neither low testosterone [HR, 1.27 (95% CI, 0.87–
dence interval (CI), 0.80 – 0.96, per quartile increase] and smok-
1.86)] nor low estradiol [HR, 1.23 (95% CI, 0.87–1.74)], with
ing (HR, 1.39; 95% CI, 1.00 –1.91; yes vs. no) at baseline pre-
medium/high levels of the other sex hormone, associated with a
dicted mortality. There was a nonlinear inverse relation between
statistically significant increase in mortality risk. These results
BMI and mortality [quartile 1 ϭ referent; quartile 2, HR, 0.72
were similar in models 1 and 2 (age or age plus BMI adjustment
(95% CI, 0.55– 0.96); quartile 3, HR, 0.79 (95% CI, 0.60 –1.03);
only). Figure 1C shows the survival plots of groups 1– 4 (log-rank
and quartile 4, HR, 0.79 (95% CI, 0.60 –1.05); quartile 1 vs.
test P Ͻ 0.001 for group 4 and nonsignificant for groups 2–3
pooled quartiles 2– 4, HR, 0.76 (95% CI, 0.61– 0.94)].
Age-adjusted (model 1) proportional hazards regression anal-
To examine the possible influence of prevalent diseases at
yses revealed an association between total and free testosterone
baseline on the relationship between sex steroids and mortality,
levels, total and free estradiol levels, and mortality when sex
we calculated HRs for mortality after excluding subjects with
steroids were entered as quartiles (P for trend Ͻ0.05) or as con-
prevalent cancer, CVD, or diabetes (Table 3). Excluding preva-
tinuous variables (Table 2). Further analyses using quartile 1 as
lent diseases showed no major impact on the association between
reference to allow direct comparison against quartiles 2, 3, and
low total or free testosterone levels and all-cause mortality, and
4 showed that risk of death increased in men within quartile 1 of
there was little impact on the association between low estradiol
total and free testosterone levels and total and free estradiol levels
levels and mortality after exclusion for prevalent CVD or dia-
compared with quartiles 2, 3, and 4 of each respective hormone,
betes. Excluding subjects with prevalent cancer attenuated the
thus revealing a nonlinear association. Results were similar for
association between total estradiol and mortality but had less
total and free sex steroid levels. The associations remained after
impact on the association between free estradiol and mortality.
further adjustment for age and BMI (model 2) as well as age, BMI,
To study how follow-up time impacts the association between
physical activity, and smoking (model 3). We observed no associ-
sex steroids and mortality, we performed analyses that excluded
ation between SHBG levels and all-cause mortality (Table 2).
subjects with a follow-up time of 3 yr or less (i.e. death within the
Because subjects within the lowest quartile of estradiol and
first 3 yr of follow-up; n ϭ 195 among 383 deaths). However,
testosterone levels showed increased risk of mortality, we inves-
this exclusion had no major influence on the results [HR (95%
tigated increased mortality risk in the lowest quartile vs. the
CI) for quartile 1 of total testosterone vs. quartiles 2– 4, 1.72
pooled quartiles 2– 4 (Table 2). Compared with subjects within
(1.21–2.43), adjusted for age, BMI, physical activity, and smok-
quartiles 2– 4, testosterone and estradiol levels within quartile 1
ing; corresponding analysis for total estradiol, HR, 1.47 (95%
associated with an increased mortality risk of 50 and 60%, re-
J Clin Endocrinol Metab, July 2009, 94(7):2482–2488
TABLE 2. HRs of sex steroids in quartiles for mortality
Risk for 1 SD increase in total testosterone
Risk for 1 SD increase in free testosterone
Risk for 1 SD increase in total estradiol
Total testosterone (Q1 vs. Q2– 4)
Model including both testosterone and estradiol
Total testosterone (Q1 vs. Q2– 4)
Data are expressed as HR (95% CI). Model 1, adjusted for age, MrOS site; model 2, adjusted for age, MrOS site, and BMI; model 3, adjusted for age, MrOS site, BMI,physical activity, and current smoking. Q, Quartile.
To analyze further the impact of BMI on the relation between
low hormone levels. In contrast, although there was a tendency,
sex hormones and mortality, we calculated the age-adjusted HR of
the risk of death from cardiovascular causes was not significantly
low testosterone or low estradiol (quartile 1 vs. pooled quartiles
increased [age-adjusted HR (95% CI) for quartile 1 of total tes-
2– 4) for mortality within each quartile of BMI. Within BMI quartile
tosterone vs. quartiles 2– 4 was 1.21 (0.81–1.79); corresponding
1, the HR (95% CI) was 1.79 (1.12–2.87) for low testosterone and
analysis for total estradiol, 1.22 (0.82–1.81)].
1.62(1.09–2.41)forlowestradiol;thecorrespondingHRswithinBMIquartile 2 were 1.89 (1.14–3.11) and 1.61 (1.00 –2.60); withinBMI quartile 3, 1.34 (0.82–2.20) and 1.40 (0.83–2.35); and within
Discussion
BMI quartile 4, 1.52 (0.97–2.39) and 1.68 (1.04 –2.71).
To study whether there was an increased incidence of car-
This prospective study investigated a possible link between se-
diovascular deaths, we analyzed the risk of CVD and non-CVD
rum testosterone and estradiol levels, assessed by GC-MS, and
death at low hormone levels. The risk of death from noncardio-
mortality in a large population-based cohort of elderly men. Our
vascular causes [age-adjusted HR (95% CI) for quartile 1 of total
results show that risk of death increased for elderly men in the
testosterone vs. quartiles 2– 4, 1.75 (1.30 –2.37); corresponding
lowest quartile of both testosterone and estradiol levels. Testos-
analysis for total estradiol, 2.00 (1.49 –2.69)] was increased at
terone and estradiol predicted death independently of each other,
Testosterone, Estradiol, and Male Mortality
J Clin Endocrinol Metab, July 2009, 94(7):2482–2488
TABLE 3. HRs of low levels of sex steroids (quartile 1 vs. quartiles 2– 4) for mortality, excluding subjects with prevalent disease
HR of low total testosterone for mortality
HR of low free testosterone for mortality
Data are expressed as HR (95% CI). Model 3, Adjusted for age, MrOS site, BMI,physical activity, and current smoking. Q, Quartile. Italics indicate reference data fromTable 2.
and risk of death nearly doubled (96% increase) in subjects withboth low testosterone and low estradiol compared with subjectswithin quartiles 2– 4 of both hormones.
To our knowledge, ours is the first study that shows estradiol as
a predictor of mortality in elderly men. Furthermore, the presentstudy is the first large study to report on the association betweenestradiol and testosterone, assessed by the reference methodGC-MS (16, 17), and mortality (18). The absence of previous stud-ies demonstrating an association between low estradiol levels andmortality may result partly from the use of immunoassay-basedtechniques, which may provide questionable specificity at low es-tradiol levels (17). Moreover, such technical restraints may explainthe paucity of studies on serum estradiol levels and other health-related outcomes in men. However, our recent study on this co-hort reported that older men with low serum estradiol, assessedby GC-MS, have increased risk of fractures (2). Therefore, it isreasonable to believe that more sensitive and reliable techniques,such as GC-MS, will help unravel important physiological effectsof estradiol in men.
Three previous prospective population-based cohort studies
investigated the relationship between serum testosterone and to-tal mortality (6, 12, 13). Although two studies observed no as-
FIG. 1. Unadjusted Kaplan-Meier survival curves according to serum sex steroid levels. A, Cumulative survival of subjects within the lowest Q of serum total
sociation between testosterone and survival (12, 13), Laughlin et
testosterone compared with Q2– 4. B, Cumulative survival of subjects within the
al. (6) showed that low testosterone associated with increased
lowest Q of serum total estradiol compared with Q2– 4. C, Cumulative survival of
mortality in men in the Rancho Bernado Study. The two negative
subjects within the lowest quartile of both serum total testosterone and estradiol. Group 1, Medium/high testosterone and medium/high estradiol; group 2, low
studies investigated middle-aged men (mean age, 52 and 55 yr,
testosterone and medium/high estradiol; group 3, low estradiol and medium/
respectively), whereas Laughlin et al. (6) studied elderly men
high testosterone; group 4, low testosterone and low estradiol. Low estradiol,
with a mean age comparable to that of the present study, possibly
Subjects within the lowest Q of estradiol (Յ16 pg/ml); medium/high estradiol,subjects within Q2– 4 of estradiol (Ͼ16 pg/ml); low testosterone, subjects within
accounting for the different results. In the study by Laughlin et al.
the lowest Q of testosterone (Յ3.36 ng/ml); medium/high testosterone, subjects
(6), 68% of the cohort (mean age, 71 yr; range, 50 –91) died during
within Q2– 4 of testosterone (Ͼ3.36 ng/ml). Q, Quartile.
an average 11.8 yr of follow-up, yielding a mortality rate of 57.5 per
J Clin Endocrinol Metab, July 2009, 94(7):2482–2488
1000 person-years at risk. In the present study, 13% of subjects
Because androgen deprivation therapy (chemical or surgical)
(mean age, 75 yr; range, 69 – 80 yr) died during an average 4.5 yr of
during treatment of prostate cancer lowers serum testosterone
follow-up, yielding a mortality rate of 28.5 per 1000 person-years
levels, such treatment may affect the association between low
at risk. Thus, our studied subjects are a few years older at baseline
testosterone levels and mortality. However, our result that ex-
and have a smaller age span, a shorter follow-up time, and a lower
cluding subjects with self-reported cancer at baseline did not
mortality rate compared with the Laughlin study. Furthermore,
significantly influence the association between low testosterone
whereas Laughlin et al. (6) used an immunoassay-based method to
and mortality does not support androgen deprivation therapy as
assess testosterone, we used GC-MS (16, 17). Despite these differ-
a pivotal factor for the results of this study.
ences, both studies found that testosterone levels within the lowest
Although there was a tendency, we did not find a statistically
quartile associated with increased risk of all-cause death (38% for
significant association between low testosterone (HR, 1.21) or es-
Laughlin et al. vs. 65% in the present study). Nested case-control,
tradiol levels (HR, 1.22) and CVD mortality risk in this cohort of
retrospective, and smaller studies also support a link between low
older men. Several previous prospective studies show no significant
testosterone and all-cause mortality in elderly men (10, 11, 14, 15).
association between testosterone levels and CVD mortality in men
We observed no relationship between SHBG levels and all-cause
(12, 13, 28 –30), whereas an association between testosterone levels
mortality, supporting an earlier prospective study (25).
and CVD death was found in the prospective cohort study of Laugh-
Interestingly, low estradiol and low testosterone predicted death
lin et al. (6) (HR, 1.36) as well as in a recent nested case-control
independently of each other, and subjects with low levels of both
study of Khaw et al. (15). To our knowledge, there are only two
testosterone and estradiol showed the highest risk of mortality in the
previous, smaller prospective studies on estradiol and CVD death in
present study. These results suggest that both hormones contribute
men, and these studies showed no significant association (28, 31).
additively to risk of death and that both low testosterone and low
In this study, the HRs for mortality were similar for total and free
estradiol may serve as markers of mortality risk in elderly men.
hormone levels. Because obesity is associated with low SHBG (30),
We propose two major hypotheses regarding the association
somewhat more diverging results for free and total hormone levels
between low sex steroid levels and mortality: 1) low sex steroid
could be expected. On the other hand, this population of men is only
levels cause or worsen disease and thereby cause death; or 2) low sex
mildly overweight (average BMI, 26.4 kg/m2). In accordance with
steroid levels are a result of disease and therefore associate with
the present data, the HRs of free and total testosterone/estradiol
death. The second hypothesis, i.e. low testosterone/estradiol is an
levels for incident fractures in this cohort were also similar (2).
epiphenomenon of preexisting diseases, is supported by evidence
We found that subjects with low BMI (within quartile 1) had
that both acute and chronic illnesses reduce testosterone production
an increased risk of death compared with subjects within quar-
(1, 26). In acute illness, testosterone is often profoundly depressed
tiles 2– 4, in accordance with most studies reporting either no
through mechanisms that act both directly at the testicular level and
relation, an inverse or a U-shaped relation between BMI and
indirectly through gonadotropin suppression (1, 26). Furthermore,
all-cause mortality in the elderly (32). The relation between low
hypogonadism due to primary testicular failure (e.g. cytokines act-
testosterone and estradiol and mortality was rather consistent
ing directly upon the testes) accompanies many chronic diseases
across BMI quartiles, but with a slight tendency to be U-shaped with
such as renal disease, alcoholic liver disease, and rheumatic diseases
the lowest HR of both hormones for mortality within BMI quartile
(1, 26). Therefore, low serum sex steroids might represent a general
3, indicating that the sex hormone status is somewhat more pre-
marker of poor health and thereby associate with increased mor-
dictive of survival in subjects with low or high BMI. Importantly,
tality risk. In our study, the association between testosterone/estra-
BMI does not distinguish fat mass from lean mass, and BMI in the
diol and mortality remained significant even after we excluded
lower range is a less valid indicator of body fatness in the elderly in
deaths that occurred during the first 3 yr of follow-up, thus arguing
which low BMI rather may indicate low lean mass (33).
against a substantial role of prevalent diseases for our observations.
Our study has limitations. The fact that only a total of 45%
Furthermore, excluding subjects with prevalent diseases (cancer,
of the subjects who were contacted participated in the study may
CVD, or diabetes) had no major impact on the association between
restrict the generalizability of our findings. The results are based
low sex steroid levels and mortality, although excluding subjects
on single measurements of sex steroids and may underestimate
with prevalent cancer slightly attenuated the association between
the true associations between the markers we studied and the risk
total estradiol and mortality. The hypothesis that low sex steroid
of death. Although most of the blood specimens in this study
levels worsen disease and thereby may cause death is supported by
were obtained between 0800 and 0830 h, some samples were
the fact that testosterone has important physiological effects on, for
obtained between 1230 and 1330 h, and given the well-docu-
example, muscle, bone, fat mass, and brain in men (1). Thus, low
mented diurnal variation in serum testosterone levels (34), this
testosterone levels may contribute to frailty that affects the individ-
may contribute to increased variability and underestimation of
ual’s capability to recover after any disease event and thereby affects
serum testosterone levels in the present study. However, a recent
survival. Furthermore, men with low serum testosterone are at in-
study showed that the diurnal variation of serum testosterone is less
creased risk of falls, low bone mineral density, and fractures (2– 4).
in older men (70 yr), with 10% lower levels at 1600 h than at
In addition, a pathogenic role of low testosterone in the develop-
0800 h, compared with a 20 –25% difference in men 30 – 40 yr old
ment of the metabolic syndrome has been suggested (18, 27). Thus,
(34). A population-based study such as ours could imply inclusion
there are several putative mechanisms by which low testosterone
of subjects treated with compounds that affect mortality risk and/or
could contribute to increased mortality, but additional studies are
sex steroid levels, thus affecting interpretation of our results. In
addition, our results are limited to elderly Caucasian men. A large
Testosterone, Estradiol, and Male Mortality
J Clin Endocrinol Metab, July 2009, 94(7):2482–2488
number of analyses have been performed in the present study, and
12. Smith GD, Ben-Shlomo Y, Beswick A, Yarnell J, Lightman S, Elwood P 2005
problems associated with multiple testing may complicate the in-
Cortisol, testosterone, and coronary heart disease: prospective evidence fromthe Caerphilly study. Circulation 112:332–340
terpretation of results. However, our main hypothesis, i.e. that low
13. Araujo AB, Kupelian V, Page ST, Handelsman DJ, Bremner WJ, McKinlay JB
serum testosterone and estradiol predict all-cause mortality, was
2007 Sex steroids and all-cause and cause-specific mortality in men. Arch
directly assessed by only a small number of analyses, and the other
14. Shores MM, Moceri VM, Gruenewald DA, Brodkin KI, Matsumoto AM,
analyses should be considered as exploratory subanalyses. Kivlahan DR 2004 Low testosterone is associated with decreased function and
In conclusion, low serum testosterone and estradiol, assessed by
increased mortality risk: a preliminary study of men in a geriatric rehabilitation
specific GC-MS, associate with risk of death in older Swedish men,
and subjects with low values of both testosterone and estradiol have
15. Khaw KT, Dowsett M, Folkerd E, Bingham S, Wareham N, Luben R, Welch A, Day N 2007 Endogenous testosterone and mortality due to all causes, cardiovas-
the highest risk of mortality. Thus, both low testosterone and low
cular disease, and cancer in men: European prospective investigation into cancer in
estradiol may serve as markers of mortality risk in elderly men.
Norfolk (EPIC-Norfolk) Prospective Population Study. Circulation 116:2694–2701
16. Wang C, Catlin DH, Demers LM, Starcevic B, Swerdloff RS 2004 Measure-
ment of total serum testosterone in adult men: comparison of current labora-tory methods versus liquid chromatography-tandem mass spectrometry. J Clin
Acknowledgments
17. Lee JS, Ettinger B, Stanczyk FZ, Vittinghoff E, Hanes V, Cauley JA, Chandler
We thank Maud Peterson and the MrOS study personnel for excellent
W, Settlage J, Beattie MS, Folkerd E, Dowsett M, Grady D, Cummings SR 2006 Comparison of methods to measure low serum estradiol levels in post-
menopausal women. J Clin Endocrinol Metab 91:3791–3797
18. Snyder PJ 2008 Might testosterone actually reduce mortality? J Clin Endocri-
Address all correspondence and requests for reprints to: Åsa Tivesten,
Wallenberg Laboratory for Cardiovascular Research, Bruna Stråket 16,
19. Mellstro¨m D, Johnell O, Ljunggren O, Eriksson AL, Lorentzon M, Mallmin H,
Sahlgrenska University Hospital, S-413 45 Go¨teborg, Sweden. E-mail:
Holmberg A, Redlund-Johnell I, Orwoll E, Ohlsson C 2006 Free testosterone
is an independent predictor of BMD and prevalent fractures in elderly men:
This work was supported by the Swedish Research Council, the
MrOS Sweden. J Bone Miner Res 21:529 –535
Swedish Foundation for Strategic Research, the ALF/LUA research grant
20. Orwoll E, Blank JB, Barrett-Connor E, Cauley J, Cummings S, Ensrud K,
in Gothenburg, the Swedish Heart-Lung Foundation, the Marianne and
Lewis C, Cawthon PM, Marcus R, Marshall LM, McGowan J, Phipps K, Sherman S, Stefanick ML, Stone K 2005 Design and baseline characteristics of
Marcus Wallenberg Foundation, the Lundberg Foundation, the Torsten
the osteoporotic fractures in men (MrOS) study–a large observational study of
and Ragnar So¨derberg’s Foundation, Petrus and Augusta Hedlunds
the determinants of fracture in older men. Contemp Clin Trials 26:569 –585
Foundation, Endorecherche, and the Novo Nordisk Foundation.
21. Labrie F, Be´langer A, Be´langer P, Be´rube´ R, Martel C, Cusan L, Gomez J,
Disclosure Summary: Å.T., L.V., M.K.K., O
Candas B, Castiel I, Chaussade V, Deloche C, Leclaire J 2006 Androgen glu-
nothing to declare. F.L. has received research grants from Endorecherche.
curonides, instead of testosterone, as the new markers of androgenic activityin women. J Steroid Biochem Mol Biol 99:182–188
22. Vandenput L, Labrie F, Mellstro¨m D, Swanson C, Knutsson T, Peeker R, Ljunggren O, Orwoll E, Eriksson AL, Damber JE, Ohlsson C 2007 Serum References
levels of specific glucuronidated androgen metabolites predict BMD and pros-tate volume in elderly men. J Bone Miner Res 22:220 –227
1. Kaufman JM, Vermeulen A 2005 The decline of androgen levels in elderly men
23. Vermeulen A, Verdonck L, Kaufman JM 1999 A critical evaluation of simple
and its clinical and therapeutic implications. Endocr Rev 26:833– 876
methods for the estimation of free testosterone in serum. J Clin Endocrinol
2. Mellstro¨m D, Vandenput L, Mallmin H, Holmberg AH, Lorentzon M, Ode´n A, Johansson H, Orwoll ES, Labrie F, Karlsson MK, Ljunggren O, Ohlsson C
24. van den Beld AW, de Jong FH, Grobbee DE, Pols HA, Lamberts SW 2000
2008 Older men with low serum estradiol and high serum SHBG have an
Measures of bioavailable serum testosterone and estradiol and their relation-
increased risk of fractures. J Bone Miner Res 23:1552–1560
ships with muscle strength, bone density, and body composition in elderly men.
3. Orwoll E, Lambert LC, Marshall LM, Blank J, Barrett-Connor E, Cauley J, Ensrud K, Cummings SR 2006 Endogenous testosterone levels, physical per-
25. Kalme T, Seppa¨la¨ M, Qiao Q, Koistinen R, Nissinen A, Harrela M, Loukovaara
formance, and fall risk in older men. Arch Intern Med 166:2124 –2131
M, Leinonen P, Tuomilehto J 2005 Sex hormone-binding globulin and insulin-like
4. Meier C, Nguyen TV, Handelsman DJ, Schindler C, Kushnir MM, Rockwood
growth factor-binding protein-1 as indicators of metabolic syndrome, cardiovas-
AL, Meikle AW, Center JR, Eisman JA, Seibel MJ 2008 Endogenous sex hor-
cular risk, and mortality in elderly men. J Clin Endocrinol Metab 90:1550 –1556
mones and incident fracture risk in older men: the Dubbo Osteoporosis Epi-
26. Karagiannis A, Harsoulis F 2005 Gonadal dysfunction in systemic diseases.
demiology Study. Arch Intern Med 168:47–54
5. Vandenput L, Mellstro¨m D, Lorentzon M, Swanson C, Karlsson MK, Brandberg
27. Basaria S, Dobs AS 2007 Testosterone making an entry into the cardiometa- J, Lo¨nn L, Orwoll E, Smith U, Labrie F, Ljunggren O, Tivesten A, Ohlsson C 2007
bolic world. Circulation 116:2658 –2661
Androgens and glucuronidated androgen metabolites are associated with meta-
28. Barrett-Connor E, Khaw KT 1988 Endogenous sex hormones and cardiovascular
bolic risk factors in men. J Clin Endocrinol Metab 92:4130 – 4137
disease in men. A prospective population-based study. Circulation 78:539 –545
6. Laughlin GA, Barrett-Connor E, Bergstrom J 2008 Low serum testosterone
29. Liu PY, Death AK, Handelsman DJ 2003 Androgens and cardiovascular dis-
and mortality in older men. J Clin Endocrinol Metab 93:68 –75
7. Emmelot-Vonk MH, Verhaar HJ, Nakhai Pour HR, Aleman A, Lock TM, Bosch JL, Grobbee DE, van der Schouw YT 2008 Effect of testosterone sup-
30. Wu FC, von Eckardstein A 2003 Androgens and coronary artery disease.
plementation on functional mobility, cognition, and other parameters in older
men: a randomized controlled trial. JAMA 299:39 –52
31. Haffner SM, Moss SE, Klein BE, Klein R 1996 Sex hormones and DHEA-SO4 in
8. Smith EP, Boyd J, Frank GR, Takahashi H, Cohen RM, Specker B, Williams
relation to ischemic heart disease mortality in diabetic subjects. The Wisconsin
TC, Lubahn DB, Korach KS 1994 Estrogen resistance caused by a mutation in
Epidemiologic Study of Diabetic Retinopathy. Diabetes Care 19:1045–1050
the estrogen-receptor gene in a man. N Engl J Med 331:1056 –1061
32. Heiat A, Vaccarino V, Krumholz HM 2001 An evidence-based assessment of
9. Gennari L, Nuti R, Bilezikian JP 2004 Aromatase activity and bone homeosta-
federal guidelines for overweight and obesity as they apply to elderly persons.
sis in men. J Clin Endocrinol Metab 89:5898 –5907
10. Shores MM, Matsumoto AM, Sloan KL, Kivlahan DR 2006 Low serum tes-
33. Willett WC, Dietz WH, Colditz GA 1999 Guidelines for healthy weight.
tosterone and mortality in male veterans. Arch Intern Med 166:1660 –1665
11. Lehtonen A, Huupponen R, Tuomilehto J, Lavonius S, Arve S, Isoaho H,
34. Brambilla DJ, Matsumoto AM, Araujo AB, McKinlay JB 2009 The effect of Huhtaniemi I, Tilvis R 2008 Serum testosterone but not leptin predicts mor-
diurnal variation on clinical measurement of serum testosterone and other sex
tality in elderly men. Age Ageing 37:461– 464
hormone levels in men. J Clin Endocrinol Metab 94:907–913
CLASSIFIEDS AD SEARCH YELLOW PAGES TRAVEL DEALS SEARCH SITE FOR: BUSINESS ENTERTAINMENT RECREATION LIFESTYLES PRINT THIS STORY | E-MAIL THIS STORY Stock show honors Anschutz-Rodgers Philanthropist and rancher named 2006 Citizen of the West By Mark Wolf, Rocky Mountain News September 27, 2005 BUSINESS Technology Western lifestyle since childhood, is the
Innovator duty of care in the pharmaceutical industryDoes the inventor or “innovator” of a brand-name drug have a duty of care to the consumers of that drug’s generic equivalent manufactured by a competitor? The Ontario Superior Court of Justice considered this question in the recent case of Goodridge v Pfizer Canada1 and determined that, for now, no such duty exists. In that decision, th
 Testosterone, Estradiol, and Male Mortality
J Clin Endocrinol Metab, July 2009, 94(7):2482–2488
TABLE 3. HRs of low levels of sex steroids (quartile 1 vs.
Testosterone, Estradiol, and Male Mortality
J Clin Endocrinol Metab, July 2009, 94(7):2482–2488
TABLE 3. HRs of low levels of sex steroids (quartile 1 vs.