Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
Triamcinoloneimpregnated nasal dressing following endoscopic sinus surgery: a randomized, doubleblind, placebocontrolled study
Rhinological and Otological Society, Inc.
Triamcinolone-Impregnated Nasal DressingFollowing Endoscopic Sinus Surgery: ARandomized, Double-Blind, Placebo-Controlled Study
David W. J. Coˆte´, MD, MPH; Erin D. Wright, MD CM, MEd
Objectives/Hypothesis: To evaluate the impact
the groups at 3- and 6-month observations (Lund-
of steroid-impregnated absorbable nasal dressing on
Kennedy, P ¼ .007 and P ¼ .02, respectively; POSE, P
wound healing and surgical outcomes after endoscopic
¼ .049 and P ¼ .01, respectively).
Conclusions: Data analysis suggests a signifi-
Study Design: A prospective, randomized, dou-
cant improvement in early postoperative healing in
ble-blinded, placebo-controlled trial.
nasal cavities receiving triamcinolone-impregnated
Methods: Chronic rhinosinusitis patients with
absorbable nasal packing following ESS and is also
polyposis who were to undergo bilateral endoscopic
associated with improved healing up to 6 months
sinus surgery were recruited and randomized to
dressing (Nasopore; Stryker Canada, Hamilton, On-
tario, Canada) in one nasal cavity and saline-impreg-
nated dressing contralaterally. Postoperative healing
assessments of edema, crusting, secretions, and scar-ring were done at postoperative days 7, 14, 28 and at3 and 6 months using validated Lund-Kennedy and
Perioperative Sinus Endoscopy (POSE) scores.
Since its advent in the 1980s, endoscopic sinus sur-
Results: Analysis of 19 enrolled patients having
gery (ESS) has replaced antrostomies and Caldwell-Luc
completed observation shows no significant differencebetween the cavity scores preoperatively using both
procedures as the treatment of choice for intractable rhi-
the POSE and Lund-Kennedy scores. There was, how-
nosinustits.1 Wound healing is a significant determinant
ever, a statistically significant difference at day 7 and
of successful outcomes in endoscopic sinus surgery. Fac-
14 in both the Lund-Kennedy (P ¼ .04 and P ¼ .03,
tors that can lead to poor surgical outcomes include
respectively) and POSE scores (P ¼ .03 and P ¼ .001,
scarring/synechiae, ostial or middle meatal obstruction,
respectively) for the treatment and control groups,
infection, and persistent inflammation in the opened
and a significant difference was also detected between
sinus cavities. Although there exists some debate as tooptimal postoperative stenting or dressing materials fol-lowing ESS, absorbable nasal dressing has been shown
From the Division of Otolaryngology, Head and Neck Surgery,
University of Alberta, Edmonton, Alberta, Canada.
in previously published literature to trend toward
Editor’s Note: This Manuscript was accepted for publication Feb-
improved wound healing and was subjectively preferred
by patients when compared to standard nasal sponges.2,3
This article has been awarded the Shirley Baron Resident
Topical steroids used preoperatively have been eval-
Research Award, Western Section, and was presented at the TriologicalSociety Combined Sections Meeting, Orlando, Florida, U.S.A., February
uated and showed a lesser rate of bacterial recovery,
again suggesting a beneficial role to postoperative out-
Investigator-initiated study with Nasopore dressings donated by
comes.4 Intranasal triamcinolone acetonide has been
Stryker Canada. Stryker Canada had no involvement in study design,protocol, methods, or analysis. The authors have no other funding, finan-
evaluated in clinical trials and found to be beneficial in
cial relationships, or conflicts of interest to disclose.
minimizing nasal secretory response, reducing inflam-
Send correspondence to David W. J. Coˆte´, MD, MPH, Chief Resi-
mation in medical treatment of rhinosinusitis. In a risk-
dent, c/o Division of Otolaryngology, Head and Neck Surgery, Universityof Alberta, 1E4 Walter McKenzie Centre, 8440-112 Street NW, Edmon-
benefit analysis, it has been associated with markedly
ton, Alberta, Canada T6G 2B7. E-mail: dcote@post.harvard.eduor cote@
few adverse side effects.4 As such, The International
Consensus Conference Proceedings on Rhinitis recom-
mend intranasal steroids as a first line therapy in
Coˆte´ and Wright: Triamcinolone-Impregnated Nasal Dressing
Fig. 1. Perioperative Sinus Endoscopy (POSE)score.
allergic rhinosinusitis.5 However, in the postoperative
there is value to a course of postoperative systemic ste-
time frame, the use of topical corticosteroid sprays, in an
roids but no strong evidence that topical steroids in a
effort to prevent recurrence of chronic rhinosinusitis
spray delivery system is beneficial. Based on this litera-
with polyposis, has met with mixed results.6 A relatively
ture and logic, we hypothesized that a more prolonged
recent, well-designed study showed no impact on recur-
and direct delivery of topical steroids in the immediate
rence rates in such patients at 1 year postoperatively. In
postoperative time frame might be able to achieve the
addition, it has been previously suggested that the use
improved objective/endoscopic appearance achieved with
of nasal packs to deliver topical antibiotics in the postop-
systemic steroids. This study, therefore, sought to assess
the potential benefit of impregnating an absorbable
What has been demonstrated to be of clinically sig-
nasal dressing with a topical steroid solution, for use as
nificant effect on objective surgical outcomes after ESS
a slow-delivery modality after sinus surgery, which had
is a short course of systemic steroids given periopera-
yet to be evaluated in a clinical trial.
tively.8 A randomized, double-blind, placebo-controlledstudy, in which patients were given 30 mg of prednisonefor 9 days postoperatively, showed a clinically significant
improvement in the endoscopic appearance of the sino-
A prospective, randomized, double-blinded, placebo-con-
nasal cavity in the short (2–4 weeks) and medium term
rhinosinusitis with polyposis who underwent bilateral ESS.
Patients were recruited in a subspecialized rhinology clinic
As discussed above, there remains a lack of consen-
among patients with chronic rhinosinusitis with polyposis re-
sus regarding optimal perioperative nasal dressing and
fractory to medical treatment requiring bilateral sinus surgery.
packing as well as the optimal postoperative medical
Consecutive adult patients with chronic rhinosinusitis were
regimen. Evidence-based practice would suggest that
approached for inclusion. Patients were excluded if they were
Coˆte´ and Wright: Triamcinolone-Impregnated Nasal Dressing
Perioperative Sinus Endoscopy Scores.
POSE ¼ Perioperative Sinus Endoscopy scores.
ineligible for informed consent, unwilling or unable to complywith the postoperative visits necessary for data collection, or
had any history of intolerance to triamcinolone. Ethics approvalwas obtained from the Human Research Ethics Board of theUniversity of Alberta, study ID# Pro00002016. Of the patients
patients missed one or two of the postoperative clinic
approached for recruitment, there were no patients declining
appointments. No adverse side effects were noted in the
Baseline Lund-Mckay, Perioperative Sinus Endoscopy
A statistically significant difference is noted at the
(POSE), and Lund-Kennedy scores were collected.8–10 These
day 7 and 14 values in both the Lund-Kennedy (P ¼ .04
objective endoscopic scoring systems for sinonasal cavities
and P ¼ .03, respectively) and POSE scores (P ¼ .03 and
include assessments of features such as crusting, mucosal
P ¼ .001, respectively) for the treatment and control
edema, polyposis, secretions, and scarring (Lund-Kennedy, two
groups. The difference lacked statistical significance
points for each category), as well as additional assessments of
at postoperative day 28 (Lund-Kennedy, P ¼ .13; POSE,
the middle turbinate, middle meatal antrostomy, and secondary
P ¼ .27), but a significant difference was detected
sinuses (POSE). The POSE scoring system has been specificallydeveloped for studies such as this, adds additional data richness
between the groups at 3 and 6 month observations
in the ethmoid inflammation category, and includes scoring
(Lund-Kennedy, P ¼ .007 and P¼ .02, respectively;
instructions for the baseline assessment (Fig. 1).8
POSE, P ¼ .049 and P ¼ .01, respectively) (see Table II
At the conclusion of the ESS, the patient was randomized
to either the left or right nasal cavity to receive 2 mL of a 40-mg/mL triamcinolone solution-impregnated bioresorbable (4 cm)dressing (Nasopore; Stryker Canada, Hamilton, Ontario, Can-ada), whereas the contralateral cavity received an identical 4-
cm dressing soaked in 2 mL of normal saline. This was done by
Success in outcomes of ESS in patients with chronic
the nursing staff, based on standardized instructions and con-
rhinosinusitis with polyposis is heavily dependant on
cealed from the surgical staff. The primary investigator left the
reducing postoperative scarring, edema, and crusting
room and nasal packing was placed in appropriate cavities
that can inhibit natural ciliary function and sinus drain-
according to the randomization. Nasal packing remained in situ
age. To this end, many rhinologists advocate aggressive
until suctioned from middle meatus at the first postoperative
use of saline irrigation and nasal steroid sprays postop-
visit 1 week later. Randomization allocation was placed in an
eratively along with meticulous debridement of the
envelope and remained sealed until all postoperative data was
ethmoid cavities and secondary sinus outflow tracts.
With this practice, incidence of synechiae formation in
Postoperative healing assessments of edema, crusting,
secretions, and scarring were done at postoperative days 7, 14,
the nasal cavity is lessened. A separate evaluation of the
28 and at 3 and 6 months using validated Lund-Kennedy and
synechia data from the POSE and Lund-Kennedy scores
POSE scores. Patients were all to resume their nasal saline irri-
was performed. Synechiae were rare in both the treat-
gation and intranasal steroid sprays postoperatively per routine
ment and control groups; there was a trend to less
synechia formation in the cavities assigned to the treat-
Sample size was calculated based on previously published
ment group, but the data lacked statistical significance
literature using the POSE scoring system with a standard devi-
ation of 3.43 as seen for a similar group of patients, with an aof 5% and a power of 80% to detect a difference in meansbetween populations of 3.5, which was felt to be clinically rele-
vant. The calculated sample size was 32 surgical cavities (16
patients) with patients serving as their own controls. Statistical
analysis was performed using the Wilcoxon signed rank test
using a significance level of P < .05.
Nineteen patients were enrolled through the rhinol-
ogy clinic at the Alberta Sinus Centre and completed
observation. Analysis of the preoperative POSE, Lund-Kennedy, and Lund-Mckay score shows no significant
difference between the cavities (see Table I). Some
Coˆte´ and Wright: Triamcinolone-Impregnated Nasal Dressing
Although Nasopore as a biologically inert absorbabledressing was an effective choice for slow delivery in themiddle meatus, one study suggested that it may be associ-ated with a slight delay in healing when compared toMerocel (Medtronic Merocel, Mystic, CT).15 Additionally,the ideal dosing remains to be clarified to achieve maxi-mal clinical benefit using this method. These are bothareas of future investigation. This practice-modifyingresult has led us to reflect on further potential targets ofthis postoperative concept. Examples of this include therole for triamcinolone-impregnated packing in postsur-gery recurrence of sinonasal inflammation and polyposisand stenting of the sphenoid ostium or frontal recess aftersurgery, which has yet to be established. Such innovations
Fig. 2. Perioperative Sinus Endoscopy (POSE) and Lund-Kennedy
are likely to become commonplace in the next several
scores postoperatively in the treatment and control groups. POD¼ postoperative day. [Color figure can be viewed in the online
years as biomaterials and pharmacology of same contin-
issue, which is available at www.interscience.wiley.com.]
Perioperative systemic steroids have also been pro-
posed as an adjuvant to topicals to reduce recurrence of
edema and polyposis, but liberal use has been limited by
The results of this study reveal a significant improve-
the side effect profile of systemic steroids. A previously
ment in early postoperative healing in sinonasal cavities
published study evaluating 30 mg of perioperative pred-
receiving triamcinolone-impregnated absorbable nasal
nisone found a difference in cavities of treatment
packing following ESS and is also associated with signifi-
patients up to 6 months postoperatively when compared
cantly improved healing up to 6 months postoperatively.
to the nasal cavities of controls, with the most signifi-cant difference noted at 2 weeks postoperatively.8
The present study presents a perfectly matched,
1. Lazar RH, Younis RT, Long TE. Functional endonasal sinus
double-blinded, placebo-controlled trial that demonstrates
surgery in adults and children. Laryngoscope 1993;103:
that a bioresorbable sinonasal dressing soaked in triamcin-
olone, when used as an adjuvant to saline irrigation and
2. Wormald PJ, Boustred RN, Le T, Hawke L, Sacks R. A pro-
conventional topical steroid sprays, is associated in a stat-
spective single-blind randomized controlled study of useof hyaluronic acid nasal packs in patients after endo-
istically and clinically significant fashion with improved
scopic sinus surgery. Am J Rhinol 2006;20:7–10.
objective sinonasal cavity findings up to 6 months postop-
3. Franklin JH, Wright ED. Randomized, controlled, study of
eratively (see Fig. 2). These significant improvements, in
absorbable nasal packing on outcomes of surgical treat-
both established objective outcome measures (Lund-Ken-
ment of rhinosinusitis. Am J Rhinol 2007;21:214–217.
nedy and POSE), combined with the benign side effect
4. Desrosiers M, Hussain A, Frenkiel S, et al. Intranasal corti-
costeroid use is associated with lower rates of bacterial
profile of topical triamcinolone compared to systemic ste-
recovery in chronic rhinosinusitis. Otolaryngol Head
roids, has led to a change in standard practice at our
institution whereby all chronic rhinosinusitis patients with
5. Gawchik SM, Saccar CL. A risk-benefit assessment of intra-
polyposis routinely receive this nasal dressing impregnated
nasal triamcinolone acetonide in allergic rhinitis. DrugSaf 2000;23:309–322.
6. Dijkstra MD, Ebbens FA, Poublon RM, Fokkens WJ. Fluti-
Previous studies have attempted to address the chal-
casone proprionate aqueous nasal spray does not influ-
ence the recurrence rate of chronic rhinosinusitis and
formation by application of topical antiproliferative
nasal polyps 1 year after functional endoscopic sinus sur-
agents.11,12 Although these attempts have, in some cases,
gery. Clin Exp Allergy 2004;34:1395–1400.
7. Shikani AH. Use of antibiotics for expansion of the Merocel
demonstrated limited success, limitations of study design
packing following endoscopic sinus surgery. Ear Nose
and follow-up, as well as concerns regarding toxicity and
long-term deleterious effects such as malignancies,
8. Wright ED, Agrawal S. Impact of perioperative systemic
remand this practice out of the mainstream. In addition, a
steroids on surgical outcomes in patients with chronicrhinosinusitis with polyposis: evaluation with the novel
recent systematic review demonstrated little value in
perioperative sinus endoscopy (POSE) scoring system.
other wound-healing modifiers, such as retinoic acid or
Laryngoscope 2007;117(11 pt 2 suppl 115):1–28.
hyaluronic acid, after ESS.13 One animal study using a
9. Lund VJ, Kennedy DW. Staging for rhinosinusitis. Otolar-
sheep mucosal model found no difference in epithelializa-
yngol Head Neck Surg 1997;117:S35–S40.
10. Lund VJ, Mackay IS. Staging in rhinosinusitis. Rhinology
impregnated with prednisolone.14 The present study
11. Konstantinidis I, Tsakiropoulou E, Vital I, Triaridis S, Vital
offers an alternative to these agents that provides evi-
V, Constantinidis J. Intra- and postoperative application
dence of overall improved surgical outcomes, including
of Mitomycin C in the middle meatus reduces adhesions
measures of edema, crusting, secretions, and scarring.
and antrostomy stenosis after FESS. Rhinology 2008;46:107–111.
Limitations to our study include the likely variable
12. Anand VK, Tabaee A, Kacker A, Newman JG, Huang C.
consistency and duration of delivery of the triamcinolone.
The role of mitomycin C in preventing synechia and
Coˆte´ and Wright: Triamcinolone-Impregnated Nasal Dressing
stenosis after endoscopic sinus surgery. Am J Rhinol
15. Shoman N, Gheriani H, Flamer D, Javer A. Prospective,
13. Weitzel EK, Wormald PJ. A scientific review of middle mea-
tal packing/stents. Am J Rhinol 2008;22:302–307.
biodegradable synthetic polyurethane foam (NasoPore) as
14. Robinson S, Adams D, Wormald PJ. The effect of nasal
packing and prednisolone on mucosal healing and recilia-
sinus surgery. J Otolaryngol Head Neck Surg 2009;38:
tion in a sheep model. Rhinology 2004;42:68–72.
Coˆte´ and Wright: Triamcinolone-Impregnated Nasal Dressing
Muira puama is the Viagra of the herbal world. It has a long history as aBrazilian folk remedy for impotence and clinical trials support this exotic Supplement Facts plant's role as a sexual stimulant. Furthermore, European and Brazilianphysicians have used muira puama to successfully treat menstrualcramps, premenstrual syndrome, rheumatism, stress, dysentery, central Amount Per Serving ne
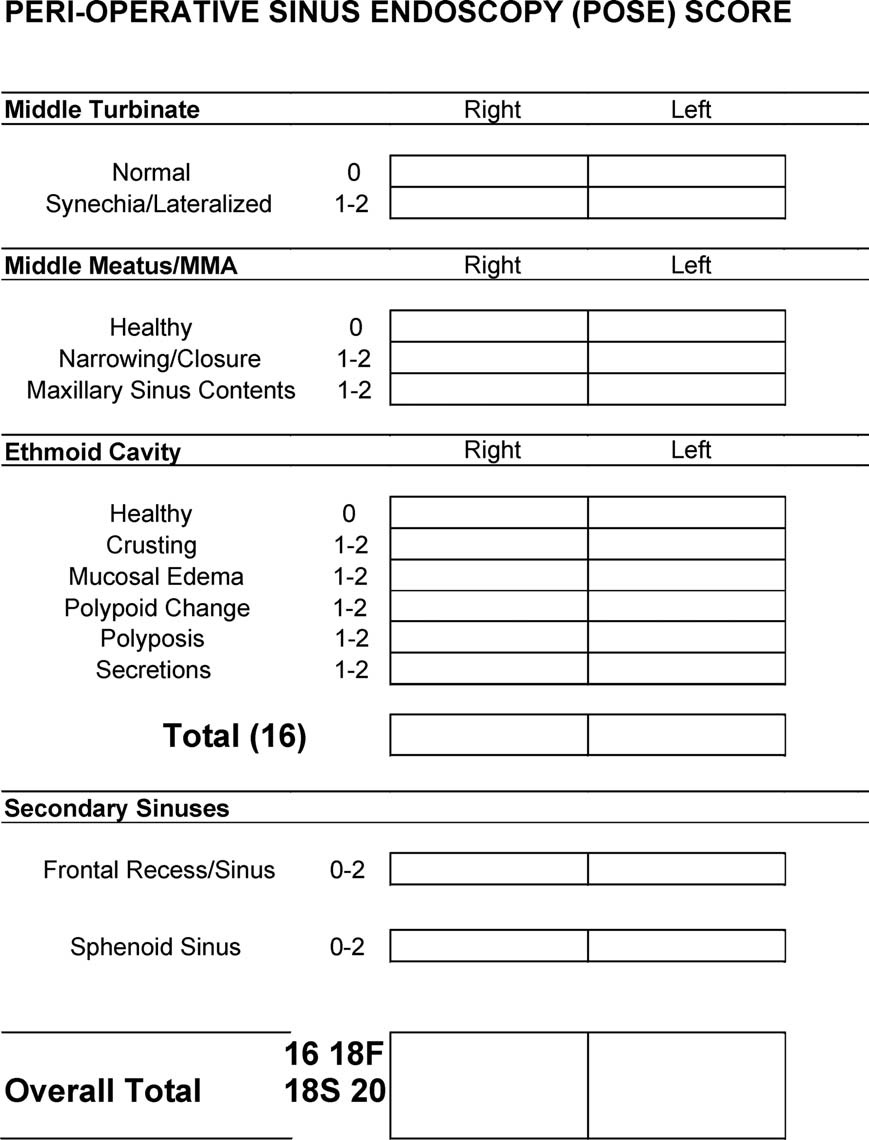 Fig. 1. Perioperative Sinus Endoscopy (POSE)score.
Fig. 1. Perioperative Sinus Endoscopy (POSE)score.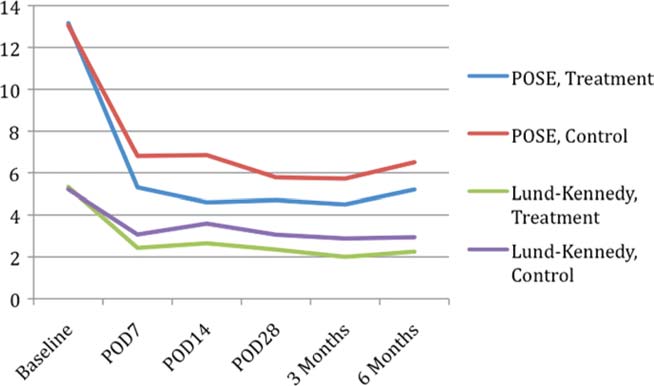 Although Nasopore as a biologically inert absorbabledressing was an effective choice for slow delivery in themiddle meatus, one study suggested that it may be associ-ated with a slight delay in healing when compared toMerocel (Medtronic Merocel, Mystic, CT).15 Additionally,the ideal dosing remains to be clarified to achieve maxi-mal clinical benefit using this method. These are bothareas of future investigation. This practice-modifyingresult has led us to reflect on further potential targets ofthis postoperative concept. Examples of this include therole for triamcinolone-impregnated packing in postsur-gery recurrence of sinonasal inflammation and polyposisand stenting of the sphenoid ostium or frontal recess aftersurgery, which has yet to be established. Such innovations
Fig. 2. Perioperative Sinus Endoscopy (POSE) and Lund-Kennedy
are likely to become commonplace in the next several
scores postoperatively in the treatment and control groups. POD¼ postoperative day. [Color figure can be viewed in the online
years as biomaterials and pharmacology of same contin-
issue, which is available at www.interscience.wiley.com.]
Perioperative systemic steroids have also been pro-
posed as an adjuvant to topicals to reduce recurrence of
edema and polyposis, but liberal use has been limited by
The results of this study reveal a significant improve-
the side effect profile of systemic steroids. A previously
ment in early postoperative healing in sinonasal cavities
published study evaluating 30 mg of perioperative pred-
receiving triamcinolone-impregnated absorbable nasal
nisone found a difference in cavities of treatment
packing following ESS and is also associated with signifi-
patients up to 6 months postoperatively when compared
cantly improved healing up to 6 months postoperatively.
Although Nasopore as a biologically inert absorbabledressing was an effective choice for slow delivery in themiddle meatus, one study suggested that it may be associ-ated with a slight delay in healing when compared toMerocel (Medtronic Merocel, Mystic, CT).15 Additionally,the ideal dosing remains to be clarified to achieve maxi-mal clinical benefit using this method. These are bothareas of future investigation. This practice-modifyingresult has led us to reflect on further potential targets ofthis postoperative concept. Examples of this include therole for triamcinolone-impregnated packing in postsur-gery recurrence of sinonasal inflammation and polyposisand stenting of the sphenoid ostium or frontal recess aftersurgery, which has yet to be established. Such innovations
Fig. 2. Perioperative Sinus Endoscopy (POSE) and Lund-Kennedy
are likely to become commonplace in the next several
scores postoperatively in the treatment and control groups. POD¼ postoperative day. [Color figure can be viewed in the online
years as biomaterials and pharmacology of same contin-
issue, which is available at www.interscience.wiley.com.]
Perioperative systemic steroids have also been pro-
posed as an adjuvant to topicals to reduce recurrence of
edema and polyposis, but liberal use has been limited by
The results of this study reveal a significant improve-
the side effect profile of systemic steroids. A previously
ment in early postoperative healing in sinonasal cavities
published study evaluating 30 mg of perioperative pred-
receiving triamcinolone-impregnated absorbable nasal
nisone found a difference in cavities of treatment
packing following ESS and is also associated with signifi-
patients up to 6 months postoperatively when compared
cantly improved healing up to 6 months postoperatively.