Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
Untitled
Adriano B. L. Tort . Oscar P. Dall’Igna . Ricardo V. de Oliveira . Carlos E. A. Mantese . Paulo Fett . Márcio W. S. Gomes . Juliana Schuh . Diogo O. Souza . Diogo R. Lara
Atypical antipsychotic profile of flunarizine in animal models
Received: 12 April 2004 / Accepted: 29 May 2004 / Published online: 28 July 2004
Abstract Rationale: Flunarizine is known as a calcium
channel blocker commonly used in many countries to treatmigraine and vertigo. Parkinsonism has been described as
Atypical antipsychotics were an important advance in the
one of its side-effects in the elderly, which is in agreement
treatment of schizophrenia and other psychotic disorders
with its recently characterized moderate D2 receptor
(Meltzer et al. ). Their main advantages include better
tolerability, especially regarding extrapyramidal symp-
evaluation of flunarizine as a potential antipsychotic.
toms, efficacy in a wider range of symptoms (Volavka et
Methods: We evaluated the action of orally administered
al. and increase in quality of life (Karow and Naber
flunarizine in mice against hyperlocomotion induced by
). However, there are concerns about metabolic and
amphetamine and dizocilpine (MK-801) as pharmacolo-
cardiovascular side-effects that may affect morbidity and
gical models of schizophrenia, induction of catalepsy as a
mortality of patients (Meltzer et al. ), added to the
measure for extrapyramidal symptoms and impairment
high cost of treatment, making them inaccessible for many
induced by dizocilpine on the delayed alternation task for
patients, particularly in developing countries. Furthermore,
working memory. Results: Flunarizine robustly inhibited
except for injectable depot risperidone, atypical antipsy-
hyperlocomotion induced by both amphetamine and
chotics are not yet available in long-acting formulations,
dizocilpine at doses that do not reduce spontaneous
which facilitate adhesion to treatment.
locomotion (3–30 mg/kg). Mild catalepsy was observed
Flunarizine, a piperazine derivative with chemical
at 30 mg/kg, being more pronounced at 50 mg/kg and
structure similar to the neuroleptic trifluoperazine, is a
100 mg/kg. Flunarizine (30 mg/kg) improved dizocilpine-
non-selective T-type, N-type and L-type calcium channel
induced impairment on the delayed alternation test.
blocker, which has long been used in some countries for
Conclusions: These results suggest a profile comparable
the treatment of migraine, vertigo and cerebrovascular
to atypical antipsychotics. The low cost, good tolerability
disorders (Todd and Benfield ; Leone et al. ;
and long half-life (over 2 weeks) of flunarizine are
Schmidt and Oestreich Flunarizine is usually well
possible advantages for its use as an atypical antipsychot-
tolerated, but clinical reports showed aggravation and
ic. These results warrant clinical trials with flunarizine for
inducement of extrapyramidal motor signs secondary to
chronic treatment with flunarizine, mainly in elderlypatients (Chouza et al. ; Brücke et al.
Keywords Flunarizine . Amphetamine . Dizocilpine .
Accordingly, animal studies suggested that this side-effect
Locomotion . Antipsychotic . Schizophrenia
could be due to moderate striatal D2 receptor antagonism(Pani et al. ; Ambrosio and Stefanini Kariya etal. ; Haraguchi et al. which was in the low to
A. B. L. Tort . O. P. Dall’Igna . R. V. de Oliveira .
moderate micromolar range. In humans, this was con-
C. E. A. Mantese . P. Fett . M. W. S. Gomes . J. Schuh .
firmed by Brücke et al. ), who found around 50% of
D2 receptor blockade in a SPECT study in patients
Departamento de Bioquímica, ICBS, UFRGS,
chronically treated with flunarizine. Thus, based on its in
vivo D2 receptor occupancy and in vitro affinity, fluna-
rizine can be categorized as a dopamine D2 receptor
antagonist of moderate affinity, in the range between
Av. Ipiranga, 6681-Prédio 12 A, Caixa Postal 1429,
olanzapine and clozapine (Seeman et al. ), therefore
sharing the main mechanism of atypical antipsychotics,
e-mail: drlara@pucrs.brFax: +55-51-33203612
according to Seeman’s proposal (Seeman and Tallerico
Kapur and Seeman ). Importantly, extrapyra-
midal symptoms typically appear after at least 6 months oftreatment with flunarizine, which can be explained by its
Mice were orally treated at 8:00 a.m. with vehicle or flunarizine atdifferent doses (1.0, 3.0, 10.0, 30.0 mg/kg). Three hours later,
long-half life (around 15–20 days) (Kariya et al.
spontaneous locomotor activity was recorded for 1 h, followed by IP
leading to its accumulation due to daily administration up
injection with dizocilpine (0.25 mg/kg) or amphetamine (5 mg/kg)
to the point when dopaminergic activity is excessively
and further recording for 3 h. A control group with oral vehicle
inhibited. Also, all patients who experienced extrapyrami-
(water) and IP saline was also included. For all injections (oral andIP), a volume of 10 ml/kg was administered.
dal symptoms in the literature were older than 55 years,
To assess locomotor activity, mice were randomly allocated to
when the physiological dopaminergic tone is decreased
individual triangular boxes (50 cm×30 cm×30 cm, 50 cm high) with
rounded corners, placed on the floor of a soundproof and diffusely
Despite these findings, flunarizine has not been
illuminated room. Locomotor activity of eight mice was recorded
proposed for the treatment of psychotic disorders or
simultaneously by a video-computerized system, with imageanalysis at four frames per second. The software (programmed by
adequately tested in pre-clinical studies aiming at its
ABL Tort) tracked the animals by distinguishing their white color
putative antipsychotic actions. However, flunarizine,
from the black background of the floor, registering X and Y
among other calcium channel blockers, has already been
horizontal coordinates. The method was set to examine horizontal
used as a pharmacological tool to study the role of calcium
locomotor activity, ignoring small movements, such as breathing,head and tail actions, and tremors. Animals had not been previously
channels in the effects of amphetamine and NMDA
habituated to the boxes and were observed for a total of 4 h (1 h
receptor antagonists, which are pharmacological models
habituation, and 3 h after IP injection), with data divided into 10 min
with predictive validity for antipsychotics in pre-clinical
studies. It was observed that flunarizine produced asignificant inhibitory effect against behaviors induced bythe indirect dopaminergic agonist amphetamine in rodents
Mice were orally treated with flunarizine at different doses (3.0,
Barrett ; Hori et al. and a borderline inhibitory
10.0, 30.0, 50.0 and 100.0 mg/kg) or vehicle, and had their catalepsy
effect against the NMDA receptor antagonist PCP (Grebb
time determined 3 h and 6 h later. Mice treated with haloperidol
1 mg/kg PO were used as positive controls. Catalepsy time was
prevented, whereas haloperidol potentiated, the EEG
measured after mice forepaws were placed over a horizontal glass
effects of PCP (Popoli et al. Feinberg and Campbell
bar (0.6 cm diameter), elevated 6 cm from the floor. The time micemaintained both forepaws over the bar and both hindpaws on the
Importantly, in all these studies flunarizine has been
ground was recorded with a cut-off time of 180 s, allowing three
administered up to 30 min before testing, not taking into
immediate attempts to replace the animal in cataleptic position
account the 2–4 h period to reach peak serum levels
within the first 10 s. Mice that kept their paws over the bar, but
showed active body or head movements were also not considered ascataleptic. The experimenter was blind to drug treatment.
In this study we investigated the profile of flunarizine as
an atypical antipsychotic. To this end, we evaluated theeffect of orally administered flunarizine on hyperactivity
induced by systemic administration of the NMDA receptorantagonist dizocilpine (MK-801) and the indirect dopa-
Delayed alternation performance was assessed in the T-maze task.
mine agonist amphetamine as pharmacological models of
The starting arm is 60 cm long, each side arm is 30 cm long, and
schizophrenia. The motor side-effects of flunarizine were
both are 20 cm high and 10 cm wide, and the test was performed in adimly illuminated room.
also evaluated by testing the potency to reduce spontane-
Mice were deprived from food until they achieved 80% of their
ous locomotor activity and to induce catalepsy. Finally,
initial weight. Then they were habituated in the T-maze for 4 days,
cognitive impairment induced by dizocilpine on the
receiving a food reward (Nescau cereal) at the end of the goal arms.
delayed alternation task was used as a measure of working
In this habituation period, each mouse was placed in the start arm of
the maze and permitted to explore it freely for 10 min, with the twoopen “goal” arms baited.
After these adaptation sessions, mice were trained as follows. In
the first trial, food reward was presented in both goal arms. During
the next 15 trials, the arm opposite to the one the animal had enteredon the previous trial was baited with food reward, except when theanimal had gone to the empty arm on the last trial. In this case, the
food was left in the same place and the baited side was changed onlyafter the animal had alternated. Sliding doors were used to keep the
Experiments were performed with male adult albino mice (CF1)
animal for a 10 s inter-trial interval in the starting arm, and to
purchased from Fundação Estadual de Pesquisa em Saúde (FEPS)
confine the mouse into the goal arm for 20 s, once it had entered in
when 21 days old and maintained in our own animal facilities under
it. This training continued until the animal reached a criterion of at
controlled environment (23±2°C, 12 h light/dark cycle, lights on at
least 11 correct choices (score) in 15 trials on 3 consecutive days. A
7:00 a.m. with free access to standard food and water) up to 3–4
maximum of 10 blocks of 15 trials (10 days) was given to each
months old (35–45 g). All behavioral experiments were in
mouse. Animals that failed to reach the criterion in these training
accordance with the Guidelines for Animal Care of our university.
Different groups of animals were used in the distinct experiments.
In the day after they matched the criterion, they received
flunarizine (10 mg/kg or 30 mg/kg) or vehicle PO and after 3 hthey were tested (15 trials). This first score was considered as pre-dizocilpine. As soon as this session was over, they received
dizocilpine (0.4 mg/kg IP) and after 30 min they were retested. Thissecond testing session was called post-dizocilpine.
Dizocilpine maleate and d-amphetamine sulfate were purchased
from Sigma (St Louis, Mo., USA) and were dissolved in fresh saline(0.9% NaCl) for acute administrations. Commercially availablesolutions for oral use of flunarizine (Flunarin, Asta Medica) andhaloperidol (Haldol, Janssen) were used.
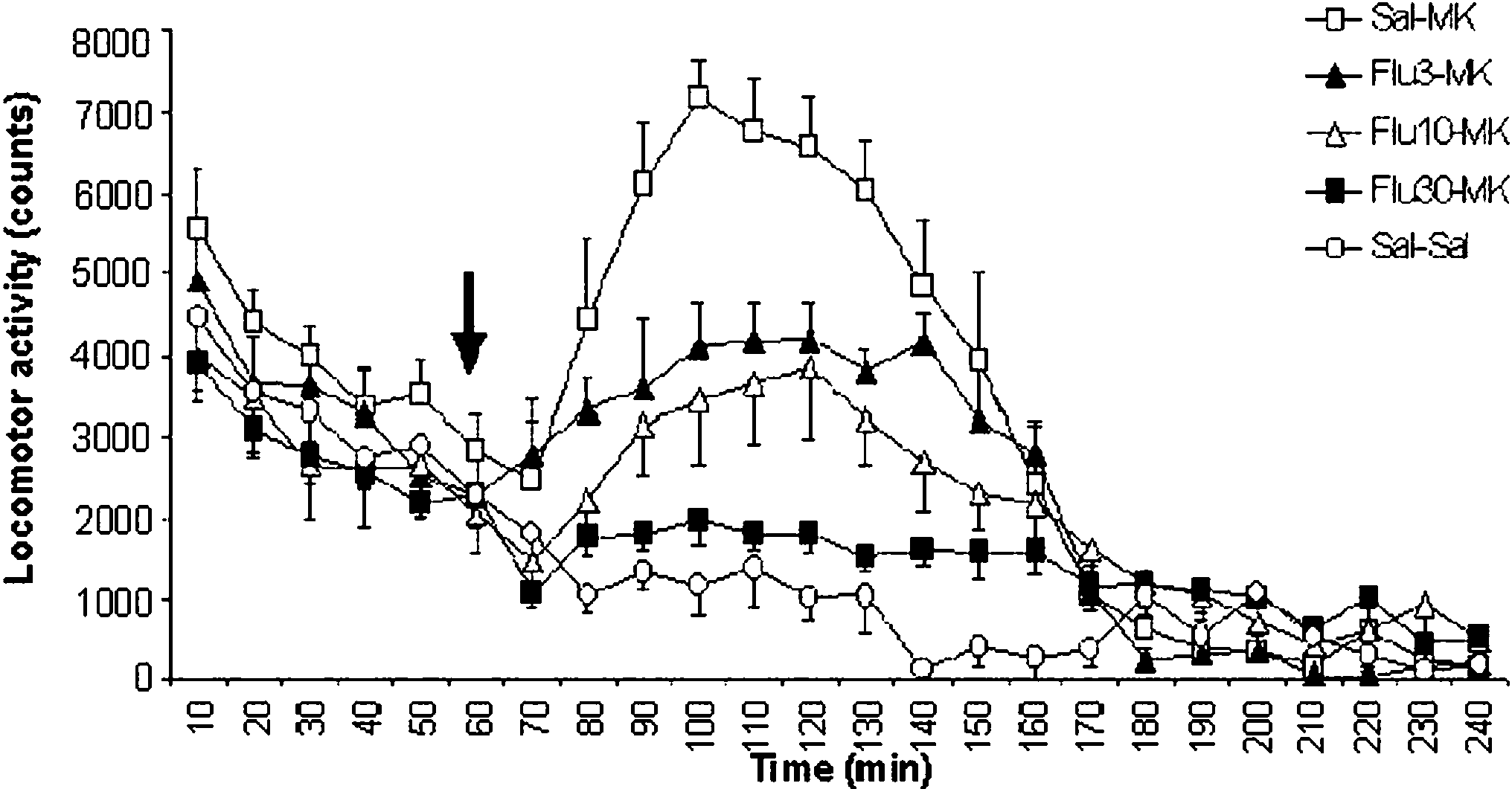
Fig. 2 Flunarizine inhibits hyperlocomotion induced by dizocilpinein mice. Flunarizine was orally administered to male adult albino
Comparisons of locomotor activities at different time points were
mice 3 h before spontaneous locomotor recording in a computerized
analyzed using General Linear Model (GLM) repeated measure
system. After 1-h habituation, mice were injected with 0.25 mg/kg
(drug treatment versus time) with time as the repeated measure.
dizocilpine or saline IP and locomotion was recorded for 3 h (n=6
Duncan’s post hoc was used to determine differences among specific
per group). Results shown as mean±SEM. Statistics (two-way
groups. Catalepsy time and delayed alternation task performance
ANOVA with time as the repeated measure): no difference between
were analyzed using the Kruskal–Wallis followed by the Mann–
groups at 0–60 min interval; saline > flu3=flu10 > flu30 at 70–
Whitney U-test due to cut-off time. A value of P<0.05 was
considered statistically significant.
statistically different from saline controls (P=0.08). Flu-
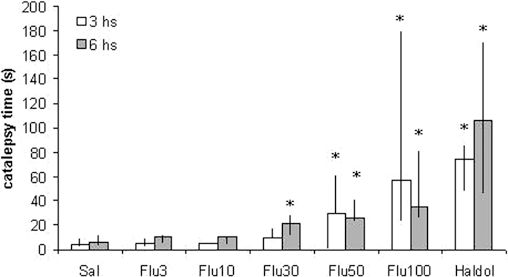
narizine caused catalepsy in a dose-dependent fashion,with no or minimal catalepsy up to 30.0 mg/kg (at 6 h: Z=
−2.747; P=0.006), whereas the higher doses of 50.0 mg/kg
and 100.0 mg/kg produced consistent catalepsy at both 3 h
P<0.001], with sal=1.0>3.0=10.0=30.0 mg/kg [between
(Z=−3.724 for 50.0 mg/kg and −3.832 for 100.0 mg/kg;
groups: F(5,36)=7.205; P<0.001] (Fig. Against
P<0.001) and 6 h (Z=−3.592 for 50.0 mg/kg and −3.622
dizocilpine, flunarizine presented a dose-time-dependent
for 100.0 mg/kg; P<0.001) after oral injections, but still
inhibition of the hyperlocomotion induced by this NMDA
less than 1 mg/kg haloperidol (at 3 h: Z=−4.310 and at 6 h
receptor antagonist [F(68,374)=7.779; P<0.001], with sal
>3.0=10.0>30.0 mg/kg [between groups: F(4,22)=9.008;
In the delayed alternation task, flunarizine 30 mg/kg
attenuated the impairment provoked by dizocilpine (Z=
Regarding motor side-effects, considering the data of
−1.983; P<0.05), while the dose of 10 mg/kg did not
the 1 h habituation period in both trials, flunarizine 30 mg/
kg presented, if anything, a mild inhibition of spontaneous
locomotion (about 18% reduction), which was not
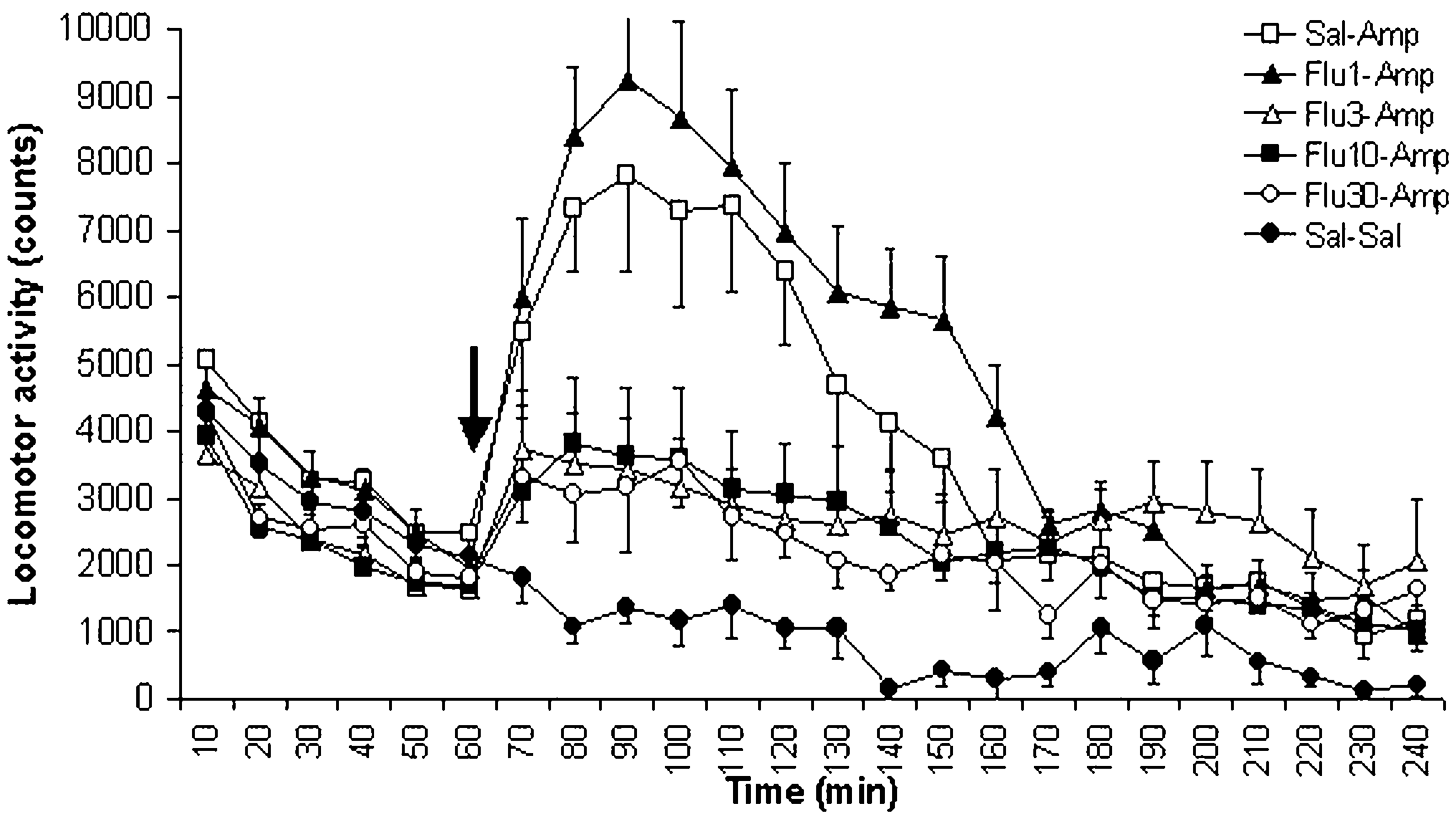
Fig. 1 Flunarizine inhibits hyperlocomotion induced by amphet-amine in mice. Flunarizine was orally administered to male adultalbino mice 3 h before spontaneous locomotor recording in acomputerized system. After 1-h habituation, mice were injected with
Fig. 3 Effect of flunarizine and haloperidol on catalepsy. Catalepsy
5 mg/kg amphetamine or saline IP and locomotion was recorded for
time was determined 3 h and 6 h after treatment with vehicle,
3 h (n=6 per group). Results shown as mean±SEM. Statistics (two-
flunarizine or haloperidol PO. A cut-off time of 180 s was used. n=8
way ANOVA with time as the repeated measure): no difference
for all groups. Data presented as medians and interquartile range. *
between groups at 0–60 min interval; sal=flu1 > flu3=flu10=flu30 at
Denotes statistically significant (P<0.05) difference from control
synaptically by A1 receptors, which inhibit dopaminerelease, as well as post-synaptically by decreasing D2receptor affinity via A –
and Souza ). Nevertheless, these combined mechan-isms seem not to excessively decrease dopaminergicactivity based on its much lower potency to producesignificant catalepsy and hypolocomotion, which is at least1 order of magnitude distant from the effective dosesagainst amphetamine and dizocilpine induced hyperloco-motion. A similar pattern has been observed forolanzapine (Ninan and Kulkarni
Age (especially >70 years old) was found to be a risk
factor for developing extrapyramidal symptoms withflunarizine (Brücke et al. similarly to antipsycho-tics. This profile is probably due to the ontogenetic decay
Fig. 4 Flunarizine attenuates dizocilpine induced impairment in the
of dopaminergic tone (Brücke et al. To our
delayed alternation task. In mice previously trained to perform a
knowledge, there is no report of extrapyramidal effect of
delayed alternation task, flunarizine (10 mg/kg or 30 mg/kg) or
flunarizine in patients younger than 55 years old. Long-
vehicle PO was orally administered to male adult albino mice 3 hbefore testing 15 trials (pre). As soon as this session was over, they
term use (usually more than 6 months) was another risk
received dizocilpine (0.4 mg/kg IP) and after 30 min they were
factor, which is not unexpected considering flunarizine’s
retested (post). n=8 for all groups, * denotes statistically significant
long half-life (more than 2 weeks). This characteristic has
(P<0.05) difference from its respective pre-test control, # denotes
been consistently overlooked in clinical practice, since it is
statistically significant (P<0.05) difference from saline post-test
normally prescribed at daily intakes. With such long half-life, rats treated daily with flunarizine presented an almostlinear accumulation of the drug in plasma and striatum
(Kariya et al. indicating that dose reduction orlonger intervals between intakes should be considered to
The present work showed that flunarizine potently
avoid motor side-effects. Apart from this side effect after
inhibited hyperlocomotion induced by amphetamine and
long-term use, flunarizine is well tolerated even by the
dizocilpine, two models with predictive validity for
antipsychotics, at doses that produced no hypolocomotion
Glutamate NMDA receptor antagonists, such as phen-
and cataleptic behavior, a characteristic suggestive of
cyclidine and dizocilpine, have also been used as a
atypical antipsychotics (Ninan and Kulkarni ). Flu-
pharmacological model for schizophrenia, producing both
narizine also improved dizocilpine-induced impairment in
hyperlocomotion and cognitive deficits in rodents (Ninan
the delayed alternation test at 30 mg/kg, a dose that caused
and Kulkarni ). Of note, typical antipsychotics
only mild catalepsy. Such profile was observed with a 3-h
typically inhibit hyperactivity induced by NMDA receptor
pretreatment interval, which is more suitable to the
antagonists at doses that inhibit spontaneous activity per
pharmacokinetic profile of flunarizine, in contrast with
se, contrary to atypical antipsychotics (O’Neill and Shaw
previous studies, which typically administered flunarizine
). Flunarizine produced a substantial dose-dependent
15–30 min before the experiments (Grebb ; Sukho-
effect in this model without significantly inhibit sponta-
neous locomotion. Flunarizine was also able to attenuate
Among animal models to identify novel compounds
the cognitive impairment induced by dizocilpine in the
with potential antipsychotic action, the indirect dopamine
delayed alternation test for working memory, which is
agonist amphetamine has been the most used pharmaco-
thought to assess frontal lobe function (Le Marec et al.
logical strategy for decades (Ellenbroek This model
). These results, therefore, further suggest an atypical
has gained further merit after direct evidence of increased
profile of flunarizine, which may count with the contribu-
dopaminergic activity in a high proportion of schizo-
tion of other mechanisms of action, such as sodium
phrenic patients (for review, see Kapur Flunarizine
channel blockade, which may also inhibit the effects of
potently inhibited amphetamine induced locomotion with-
NMDA receptor antagonists (Farber et al.
out a gradual dose response, since 1 mg/kg was ineffective
Based on its pharmacological profile in clinical practice
and the doses of 3, 10 and 30 mg/kg were equally
(regarding tolerability) and in these models, flunarizine
effective. Given the complex mechanism of action fluna-
has putative antipsychotic action without major motor
rizine, perhaps this effect may not be ascribed solely to its
side-effects, similarly to atypical antipsychotics. More-
D2 receptor antagonist properties. Inhibition of calcium
over, after target symptoms have improved, flunarizine has
and sodium channels by flunarizine (Holmes et al.
the potential to be orally administered weekly or twice a
Velly et al. ; Pauwels et al. can inhibit
month, which could considerably improve typically poor
catecholamine release. Also, a possible increase in aden-
treatment compliance in psychotic patients (Perkins
osine (Phillis et al. ; Popoli et al. ) by flunarizine
The long half-life also may prevent abrupt exacerbation of
treatment can also attenuate dopaminergic activity pre-
symptoms in the case of abandoning the treatment.
Conversely, if extrapyramidal side-effects occur, anticho-
Lara DR, Souza DO (2000) Schizophrenia: a purinergic hypothesis.
linergic treatment would have to be initiated until plasma
Leone M, Grazzi L, La Mantia L, Bussone G (1991) Flunarizine in
levels decrease significantly after dose adjustment.
migraine: a minireview. Headache 31:388–391
Another notable advantage of flunarizine is its very low
Le Marec N, Ethier K, Rompre PP, Godbout R (2002) Involvement
cost, which is 10–40 times lower in comparison with
of the medial prefrontal cortex in two alternation tasks using
atypical antipsychotics. It is also available in liquid
different environments. Brain Cogn 48:432–436
Meltzer HY, Davidson M, Glassman AH, Vieweg WV (2002)
formulation, which was used in this study. Taken together,
Assessing cardiovascular risks versus clinical benefits of
these characteristics may increase treatment compliance
atypical antipsychotic drug treatment. J Clin Psychiatry
with flunarizine in comparison with commercially avail-
able antipsychotics. Clinical trials with flunarizine for the
Ninan I, Kulkarni SK (1999) Preferential inhibition of dizocilpine-
treatment of schizophrenia and other psychotic disorders
induced hyperlocomotion by olanzapine. Eur J Pharmacol368:1–7
are therefore warranted to confirm its putative profile as a
O’Neill MF, Shaw G (1999) Comparison of dopamine receptor
antagonists on hyperlocomotion induced by cocaine, amphet-amine, MK-801 and the dopamine D1 agonist C-APB in mice. Psychopharmacology 145:237–250
This work was supported by grants of CNPq
Pani L, Kuzmin A, Stefanini E, Gessa GL, Rossetti ZL (1990)
Flunarizine potentiates cocaine-induced dopamine release andmotor stimulation in rats. Eur J Pharmacol 190:223–227
Pauwels PJ, Leysen JE, Janssen PA (1991) Ca++ and Na+ channels
involved in neuronal cell death. Protection by flunarizine. Life
Perkins DO (2002) Predictors of noncompliance in patients with
Ambrosio C, Stefanini E (1991) Interaction of flunarizine with
schizophrenia. J Clin Psychiatry 63:1121–1128
dopamine D2 and D1 receptors. Eur J Pharmacol 197:221–223
Phillis JW, Wu PH, Coffin VL (1983) Inhibition of adenosine uptake
Brücke T, Wober C, Podreka I, Wober-Bingol C, Asenbaum S, Aull
into rat brain synaptosomes by prostaglandins, benzodiazepines
S, Wenger S, Ilieva D, Harasko-van der Meer C, Wessely P et
and other centrally active compounds. Gen Pharmacol 14:475–
al. (1995) D2 receptor blockade by flunarizine and cinnarizine
explains extrapyramidal side effects. A SPECT study. J Cereb
Popoli P, Pezzola A, Scotti de Carolis A (1990) Possible
involvement of the adenosinergic system in flunarizine anti-
Chouza C, Scaramelli A, Caamano JL, De Medina O, Aljanati R,
convulsant activity in rats. Arch Int Pharmacodyn Ther 306:45–
Romero S (1986) Parkinsonism, tardive dyskinesia, akathisia,
and depression induced by flunarizine. Lancet 1:1303–1304
Popoli P, Pezzola A, Benedetti M, Scotti de Carolis A (1992)
Ellenbroek BA (1993) Treatment of schizophrenia: a clinical and
Verapamil and flunarizine inhibit phencyclidine-induced ef-
preclinical evaluation of neuroleptic drugs. Pharmacol Ther
fects: an EEG and behavioural study in rats. Neuropharmacol-
Farber NB, Jiang XP, Heinkel C, Nemmers B (2002) Antiepileptic
Rosenzweig-Lipson S, Barrett JE (1995) Modification of the
drugs and agents that inhibit voltage-gated sodium channels
behavioral effects of (±) BAY k 8644, cocaine and d-
prevent NMDA antagonist neurotoxicity. Mol Psychiatry
amphetamine by L-type calcium channel blockers in squirrel
monkeys. J Pharmacol Exp Ther 274:842–851
Feinberg I, Campbell IG (1998) Haloperidol potentiates the EEG
Schmidt R, Oestreich W (1991) Flunarizine in the treatment of
slowing of MK-801 despite blocking its motor effects:
vestibular vertigo: experimental and clinical data. J Cardiovasc
implications for the PCP model of schizophrenia. Neuroreport
Seeman P, Tallerico T (1998) Antipsychotic drugs which elicit little
Grebb JA (1986) Nifedipine and flunarizine block amphetamine-
or no Parkinsonism bind more loosely than dopamine to brain
induced behavioral stimulation in mice. Life Sci 38:2375–2381
D2 receptors, yet occupy high levels of these receptors. Mol
Haraguchi K, Ito K, Kotaki H, Sawada Y, Iga T (1998) Catalepsy
induced by calcium channel blockers in mice. Biopharm Drug
Seeman P, Corbett R, Van Tol HH (1997) Atypical neuroleptics have
low affinity for dopamine D2 receptors or are selective for D4
Holmes B, Brogden RN, Heel RC, Speight TM, Avery GS (1984)
receptors. Neuropsychopharmacology 16:93–110
Flunarizine. A review of its pharmacodynamic and pharmaco-
Sukhotina IA, Dravolina OA, Medvedev IO, Bespalov AY (1999)
kinetic properties and therapeutic use. Drugs 27:6–44
Effects of calcium channel blockers on behaviors induced by
Hori Y, Takeda H, Tsuji M, Matsumiya T (1998) Differentiation of
the N-methyl-D-aspartate receptor antagonist, dizocilpine, in
the inhibitory effects of calcium antagonists on abnormal
rats. Pharmacol Biochem Behav 63:569–580
behaviors induced by methamphetamine or phencyclidine.
Todd PA, Benfield P (1989) Flunarizine. A reappraisal of its
pharmacological properties and therapeutic use in neurological
Kapur S (2003) Psychosis as a state of aberrant salience: a
framework linking biology, phenomenology, and pharmacology
Velly J, Grima M, Marciniak G, Spach MO, Schwartz J (1987)
in schizophrenia. Am J Psychiatry 160:13–23
Effects of some antianginal and vasodilating drugs on sodium
Kapur S, Seeman P (2001) Does fast dissociation from the dopamine
influx and on the binding of 3H-batrachotoxinin-A 20-alpha-
D2 receptor explain the action of atypical antipsychotics? A
benzoate and 3H-tetracaine. Naunyn-Schmiedeberg’s Arch
new hypothesis. Am J Psychiatry 158:360–369
Kariya S, Isozaki S, Masubuchi Y, Suzuki T, Narimatsu S (1995)
Volavka J, Czobor P, Sheitman B, Lindenmayer JP, Citrome L,
Possible pharmacokinetic and pharmacodynamic factors affect-
McEvoy JP, Cooper TB, Chakos M, Lieberman JA (2002)
ing parkinsonism inducement by cinnarizine and flunarizine.
Clozapine, olanzapine, risperidone, and haloperidol in the
treatment of patients with chronic schizophrenia and schizoaf-
Karow A, Naber D (2002) Subjective well-being and quality of life
fective disorder. Am J Psychiatry 159:255–262
under atypical antipsychotic treatment. Psychopharmacology162:3–10
Solution orale Duphalac VERS UN EMBALLAGE HARMONIEUX… Chaque mois, Fabrice Peltier , président L’étiquette « pelable » de la bouteille de solution oralede P’Référence - Dynamiseur de marques,Duphalac remplace à elle seule les traditionnels étuiprésente un produit qui, à ses yeux, a suet la notice. De plus elle incorpore aussi lamatériaux d’emballage, gain
Prova scritta del concorso pubblico per la nomina di n. 400 allievi vice ispettori del Corpo forestale dello Stato (bando in G.U. 29 novembre 2011) Sessione 3 Nominativo Data di nascita Luogo di nascita Punteggio Prova scritta del concorso pubblico per la nomina di n. 400 allievi vice ispettori del Corpo forestale dello Stato (bando in G.U. 29 novembre 2011) Sessione 3 Nominativo
 dizocilpine (0.4 mg/kg IP) and after 30 min they were retested. Thissecond testing session was called post-dizocilpine.
dizocilpine (0.4 mg/kg IP) and after 30 min they were retested. Thissecond testing session was called post-dizocilpine.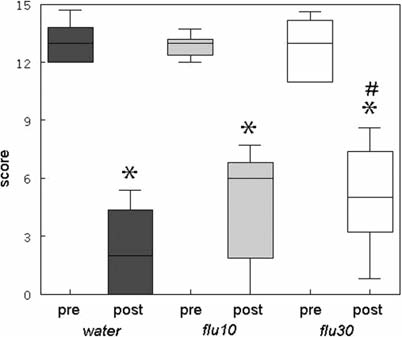 synaptically by A1 receptors, which inhibit dopaminerelease, as well as post-synaptically by decreasing D2receptor affinity via A –
and Souza ). Nevertheless, these combined mechan-isms seem not to excessively decrease dopaminergicactivity based on its much lower potency to producesignificant catalepsy and hypolocomotion, which is at least1 order of magnitude distant from the effective dosesagainst amphetamine and dizocilpine induced hyperloco-motion. A similar pattern has been observed forolanzapine (Ninan and Kulkarni
Age (especially >70 years old) was found to be a risk
factor for developing extrapyramidal symptoms withflunarizine (Brücke et al. similarly to antipsycho-tics. This profile is probably due to the ontogenetic decay
Fig. 4 Flunarizine attenuates dizocilpine induced impairment in the
of dopaminergic tone (Brücke et al. To our
delayed alternation task. In mice previously trained to perform a
knowledge, there is no report of extrapyramidal effect of
delayed alternation task, flunarizine (10 mg/kg or 30 mg/kg) or
flunarizine in patients younger than 55 years old. Long-
vehicle PO was orally administered to male adult albino mice 3 hbefore testing 15 trials (pre). As soon as this session was over, they
term use (usually more than 6 months) was another risk
received dizocilpine (0.4 mg/kg IP) and after 30 min they were
factor, which is not unexpected considering flunarizine’s
retested (post). n=8 for all groups, * denotes statistically significant
long half-life (more than 2 weeks). This characteristic has
(P<0.05) difference from its respective pre-test control, # denotes
been consistently overlooked in clinical practice, since it is
statistically significant (P<0.05) difference from saline post-test
normally prescribed at daily intakes. With such long half-life, rats treated daily with flunarizine presented an almostlinear accumulation of the drug in plasma and striatum
(Kariya et al. indicating that dose reduction orlonger intervals between intakes should be considered to
The present work showed that flunarizine potently
avoid motor side-effects. Apart from this side effect after
inhibited hyperlocomotion induced by amphetamine and
long-term use, flunarizine is well tolerated even by the
dizocilpine, two models with predictive validity for
antipsychotics, at doses that produced no hypolocomotion
Glutamate NMDA receptor antagonists, such as phen-
and cataleptic behavior, a characteristic suggestive of
cyclidine and dizocilpine, have also been used as a
atypical antipsychotics (Ninan and Kulkarni ). Flu-
pharmacological model for schizophrenia, producing both
narizine also improved dizocilpine-induced impairment in
hyperlocomotion and cognitive deficits in rodents (Ninan
the delayed alternation test at 30 mg/kg, a dose that caused
and Kulkarni ). Of note, typical antipsychotics
only mild catalepsy. Such profile was observed with a 3-h
typically inhibit hyperactivity induced by NMDA receptor
pretreatment interval, which is more suitable to the
antagonists at doses that inhibit spontaneous activity per
pharmacokinetic profile of flunarizine, in contrast with
se, contrary to atypical antipsychotics (O’Neill and Shaw
previous studies, which typically administered flunarizine
). Flunarizine produced a substantial dose-dependent
15–30 min before the experiments (Grebb ; Sukho-
effect in this model without significantly inhibit sponta-
neous locomotion. Flunarizine was also able to attenuate
Among animal models to identify novel compounds
the cognitive impairment induced by dizocilpine in the
with potential antipsychotic action, the indirect dopamine
delayed alternation test for working memory, which is
agonist amphetamine has been the most used pharmaco-
thought to assess frontal lobe function (Le Marec et al.
synaptically by A1 receptors, which inhibit dopaminerelease, as well as post-synaptically by decreasing D2receptor affinity via A –
and Souza ). Nevertheless, these combined mechan-isms seem not to excessively decrease dopaminergicactivity based on its much lower potency to producesignificant catalepsy and hypolocomotion, which is at least1 order of magnitude distant from the effective dosesagainst amphetamine and dizocilpine induced hyperloco-motion. A similar pattern has been observed forolanzapine (Ninan and Kulkarni
Age (especially >70 years old) was found to be a risk
factor for developing extrapyramidal symptoms withflunarizine (Brücke et al. similarly to antipsycho-tics. This profile is probably due to the ontogenetic decay
Fig. 4 Flunarizine attenuates dizocilpine induced impairment in the
of dopaminergic tone (Brücke et al. To our
delayed alternation task. In mice previously trained to perform a
knowledge, there is no report of extrapyramidal effect of
delayed alternation task, flunarizine (10 mg/kg or 30 mg/kg) or
flunarizine in patients younger than 55 years old. Long-
vehicle PO was orally administered to male adult albino mice 3 hbefore testing 15 trials (pre). As soon as this session was over, they
term use (usually more than 6 months) was another risk
received dizocilpine (0.4 mg/kg IP) and after 30 min they were
factor, which is not unexpected considering flunarizine’s
retested (post). n=8 for all groups, * denotes statistically significant
long half-life (more than 2 weeks). This characteristic has
(P<0.05) difference from its respective pre-test control, # denotes
been consistently overlooked in clinical practice, since it is
statistically significant (P<0.05) difference from saline post-test
normally prescribed at daily intakes. With such long half-life, rats treated daily with flunarizine presented an almostlinear accumulation of the drug in plasma and striatum
(Kariya et al. indicating that dose reduction orlonger intervals between intakes should be considered to
The present work showed that flunarizine potently
avoid motor side-effects. Apart from this side effect after
inhibited hyperlocomotion induced by amphetamine and
long-term use, flunarizine is well tolerated even by the
dizocilpine, two models with predictive validity for
antipsychotics, at doses that produced no hypolocomotion
Glutamate NMDA receptor antagonists, such as phen-
and cataleptic behavior, a characteristic suggestive of
cyclidine and dizocilpine, have also been used as a
atypical antipsychotics (Ninan and Kulkarni ). Flu-
pharmacological model for schizophrenia, producing both
narizine also improved dizocilpine-induced impairment in
hyperlocomotion and cognitive deficits in rodents (Ninan
the delayed alternation test at 30 mg/kg, a dose that caused
and Kulkarni ). Of note, typical antipsychotics
only mild catalepsy. Such profile was observed with a 3-h
typically inhibit hyperactivity induced by NMDA receptor
pretreatment interval, which is more suitable to the
antagonists at doses that inhibit spontaneous activity per
pharmacokinetic profile of flunarizine, in contrast with
se, contrary to atypical antipsychotics (O’Neill and Shaw
previous studies, which typically administered flunarizine
). Flunarizine produced a substantial dose-dependent
15–30 min before the experiments (Grebb ; Sukho-
effect in this model without significantly inhibit sponta-
neous locomotion. Flunarizine was also able to attenuate
Among animal models to identify novel compounds
the cognitive impairment induced by dizocilpine in the
with potential antipsychotic action, the indirect dopamine
delayed alternation test for working memory, which is
agonist amphetamine has been the most used pharmaco-
thought to assess frontal lobe function (Le Marec et al.