Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
Oral xylose isomerase decreases breath hydrogen excretion and improves gastrointestinal symptoms in fructose malabsorption a doubleblind, placebocontrolled study
Oral xylose isomerase decreases breath hydrogen excretionand improves gastrointestinal symptoms in fructosemalabsorption – a double-blind, placebo-controlled study
P. Komericki*, M. Akkilic-Materna*, T. Strimitzer†, K. Weyermair†, H. F. Hammer‡ & W. Aberer*
Dermatology and Venereology,Medical University of Graz, Graz,
Austria. †Austrian Agency for Health and Food
Incomplete resorption of fructose results in increased colonic hydrogen pro-
duction and is a frequent cause of abdominal symptoms. The only treat-
‡Division of Gastroenterology andHepatology, Department of InternalMedicine, Medical University of Graz,
To study whether orally administered xylose isomerase (XI), an enzymethat catalyses the reversible isomerisation of glucose and fructose, candecrease breath hydrogen excretion in patients with fructose malabsorption.
Correspondence to:Prof. Dr P. Komericki, Department of
Environmental Dermatology andVenereology, Medical University of
Patients received 25 g fructose in 100 mL water together with either pla-
cebo or XI capsules. Primary endpoint was the reduction in breath hydro-
gen excretion, as assessed by the area under the breath hydrogen curve
over 4 h (AUC). A secondary endpoint was the reduction in abdominalpain, bloating and nausea assessed on a visual analogue scale (VAS, range:
0–10). A P value <0.05 was considered statistically significant.
Sixty-five patients in whom fructose malabsorption had been diagnosed by
positive breath hydrogen test within the previous year, were included in thestudy [15 males, 50 females; mean age 43.3 (s.d. = 14.4), range:21–73 years]. The median AUC was 885 ppm/240 min in the XI groupcompared to 2071 ppm/240 min in the placebo group (P = 0.00). Medianscores for abdominal pain (0.7 vs. 1.3) and nausea (0.2 vs. 0.6), but not forbloating (P = 0.053), were significantly improved after XI (P = 0.009 andP = 0.005) as compared with placebo.
ConclusionsOral administration of xylose isomerase significantly decreased breathhydrogen excretion after ingestion of a watery fructose solution. Nauseaand abdominal pain were significantly improved by xylose isomerase.
breath hydrogen test. The sensitivity of this breath
Fructose is present in modern diets either as a constitu-
hydrogen test, however, is influenced by the prevalence
ent of the disaccharide sucrose or as the monosaccha-
of hydrogen non-excretion, which has been reported to
ride. Average daily intake varies from 11 to 54 g.1
be up to 18%.24 Incomplete fructose absorption usually
Fructose is used as a sweetener or as high fructose corn
is identified by a positive result on a breath hydrogen
syrup in soda, fruit juices or candy, and it is naturally
test after ingestion of 25–50 g of fructose.
present in fruits like apples, peaches, pears and oranges.2
There is a lack of information on the prevalence of
From 1970 to 1997, daily per capita intake of fructose
incomplete absorption of fructose in the healthy popula-
increased from below 1 g to over 70 g while consump-
tion, but self selection of persons coming to the test may
tion of sucrose, a disaccharide in which fructose is linked
play an important role. In studies on small numbers of
healthy subjects between 11% and 50% had a positive
The absorptive capacity for fructose that is not accom-
breath hydrogen test after 25 g of fructose, and between
panied by glucose is small.4 The normal absorptive
38% and 81% of subjects had a positive breath hydrogen
capacity for fructose depends on other nutrients as well,
test after 50 g of fructose. In normal subjects who
and still is poorly understood. It has been suggested that
ingested 25 g of fructose, incomplete absorption docu-
healthy subjects have the capacity to absorb up to 25 g
mented by a positive hydrogen breath test had only a
of fructose, whereas many have incomplete absorption
marginal effect on symptoms, whereas after 50 g of fruc-
and intolerance with intake of 50 g of fructose.5 Inges-
tose there was a more pronounced effect on symptoms
tion of food that contains fructose in excess of glucose
in previously asymptomatic normal subjects with docu-
may result in symptoms such as abdominal bloating or
diarrhoea and also may provoke symptoms in patients
The same review also summarised results of hydrogen
with irritable bowel syndrome (IBS).6–8 It has been sug-
breath testing in patients with functional gut disorders.1
gested that as little as 3 g of fructose may induce symp-
In these patients, the prevalence of a positive hydrogen
toms in functional bowel disorders. Gender may
breath test after 25 g of fructose was between 39% and
80%, increasing with the concentration of the fructose
Incompletely absorbed fructose reaches the colon,
where bacterial carbohydrate metabolism results in pro-
When studies in patients or normal subjects using
duction of short chain fatty acids and gases like hydro-
25 g of fructose were compared, patients with functional
gen. This may cause symptoms like abdominal pain,
gut disorders and a positive hydrogen breath test in gen-
bloating, discomfort and diarrhoea.10–12 These symptoms
eral had a higher likelihood of symptoms as compared
are not specific for fructose malabsorption but also occur
with previously asymptomatic normal subjects with a
with other incompletely absorbed carbohydrates, like die-
positive breath hydrogen test. However, after 50 g of
tary fibres, sorbitol, lactose in case of lactase deficiency
fructose, the proportion of patients with a positive
or carbohydrate malabsorption in severe restriction of
breath hydrogen tests and the proportion of patients
pancreatic digestive or intestinal absorptive capac-
who had symptoms related to incomplete fructose
ity.11, 13–15 Recently the term FODMAP, describing fer-
absorption was similar to normal subjects.1 These obser-
mentable oligo-, di- and monosaccharides and polyols
vations suggest that patients with functional gastrointes-
has been used to characterise short chain carbohydrates
tinal disorders may have a greater likelihood to be
which potentially may trigger abdominal symptoms and
referred to a fructose hydrogen breath test, and that they
for which dietary restriction has been suggested to be
may be more sensitive to lower doses of malabsorbed
efficacious.16, 17 Continued ingestion of high amounts of
fructose has been suggested to result in a variety of other
Xylose isomerase (XI, EC 5.3.1.5, CAS 9023-82-9) is
impairments. Since the year 1975 it has been discussed
an enzyme that catalyses the reversible isomerisation of
that enhanced dietary fructose could induce obesity,
glucose and fructose.26 It has been used for the industrial
accelerated ageing, insulin resistance and non-alcoholic
conversion of glucose to fructose in the manufacture of
fatty liver disease.18–22 In addition, some types of depres-
high fructose corn syrup.27 XI is available from industrial
sion could be related to long time consumption of high
production and has been proven not to provoke allergic
reactions in man. Furthermore, GRAS (Generally Recog-
Hydrogen produced in the colon is absorbed and
nized As Safe) status of the enzyme has been affirmed
excreted in breath. This can be used for a diagnostic
Xylose isomerase in fructose malabsorption
We hypothesised that orally administered XI is able to
under the breath hydrogen curve (AUC) over a 4 h
catalyse the conversion of poorly absorbable fructose into
observation period. AUC after fructose plus XI was com-
well-absorbable glucose in the human intestine in vivo and
pared with AUC after fructose plus placebo. Secondary
thereby reduce breath hydrogen excretion after ingestion
endpoint was the reduction of the symptoms abdominal
of fructose in patients with incomplete fructose absorp-
pain, bloating and nausea using a visual analogue score.
tion. To assess this hypothesis, we performed a double-blind randomised crossover study in patients with
previously established fructose malabsorption. Breath
The XI capsule (258.2 mg) (Fructosin; Sciotec, Tulln,
hydrogen excretion was assessed in patients who received
Austria) contains 43.12 mg of this enzyme showing an
either XI or placebo with an oral watery fructose load. A
activity of approximately 1.6 lkat per caps. Further
secondary endpoint was the assessment of the effect of XI
ingredients, amongst others are microcrystalline cellulose
on symptoms using a visual analogue scale (VAS).
(70.43 mg), gelatine (47.24 mg), maltose (25.13 mg),shellac
(20.4 mg). Placebo capsules are composed of microcrys-talline cellulose (200 mg) and gelatine (47.24 mg). To
ensure reproducible activity of the enzyme a crystallisa-
This randomised, double-blind, placebo-controlled, pro-
tion process that yields highly active and stable crystals
spective, crossover interventional study was conducted in
of XI was developed (patent application EP2161034).
the Department of Environmental Dermatology and Ve-
These crystals were then incorporated into small micro-
nereology of the Medical University of Graz, Austria,
pellets with a diameter of approximately 1 mm. This size
from June 2009 until May 2010 in accordance with the
ensures that pellets are emptied during the digestive
principles of Good Clinical Practice (GCP) correspond-
phase of stomach emptying.28 Pellets had an enteric
ing to the ICH guidelines (International Conference on
coating with a thin film of shellac to protect the enzyme
Harmonisation of drugs and medical devices).
from acidic denaturation during stomach transit. The
The protocol was registered at ClinicalTrials.gov
pellets were packed into gelatine capsules which dissolve
(NCT00916487) and at EudraCT (EUDRACT2008-
quickly in the stomach releasing the pellets.29
005861-80) and approved by the Ethics Committee ofthe Medical University of Graz (EK 20-024 ex 08/09).
Preparation, randomisation protocol and use of testkits
The producer of XI capsules prepared numbered test kits
The study was performed in patients who were referred
containing (i) fructose for two tests (25 g each in two
for a fructose hydrogen breath test for the evaluation of
100 mL plastic bottles), and (ii) three capsules of XI and
abdominal symptoms, and in whom fructose malabsorp-
three capsules of placebo which were randomly assigned
tion was confirmed within the preceding 12 months. Tests
to sealed bags marked with ‘X’ and ‘Y’ respectively. Test
were performed in the departments of gastroenterology or
kits were sent by courier to the test centre. XI and pla-
dermatology of our university. Fructose malabsorption
cebo capsules looked and tasted identical. This procedure
was confirmed if there was an increase in end expiratory
guaranteed blinding of researchers and participants. Sub-
breath hydrogen concentration of at least 20 ppm over
jects were randomised to groups A and B according to a
baseline after 25 or 30 g of fructose; 30 g was used at the
scheme defined before starting inclusion and randomly
department of gastroenterology and 25 g was used at the
assigned to a predefined test kit number. Subjects of
department of dermatology. Exclusion criteria were preg-
group A had to start with capsules contained in the
nancy, breast feeding, diabetes mellitus and gastrointesti-
sealed bag ‘X’, and subjects of group B started with cap-
nal surgery, endoscopy or antibiotic treatment within the
sules contained in bag ‘Y’. For the second test, the cap-
preceding 4 weeks. Before enrolment, every patient signed
sules in the remaining bag (Y or X, respectively) had to
a declaration of consent after having been provided with
be taken. Deblinding of test kits was done in a joint
thorough verbal and written information.
meeting of investigators (P. K, T. S.) and representativesof the producer of capsules.
Therefore, randomisation was performed on several
Primary endpoint was the assessment of breath H2
levels. XI and placebo capsules were randomly assigned to
excretion after fructose intake by calculating the area
sealed bags marked with ‘X’ or ‘Y’ for each test kit before
test kit preparation. Test kits were numbered consecu-
tively. Subjects were randomly assigned to a numbered
Nonparametric methods were used for the inference sta-
test kit and, independently, to group A and B. Assignment
to groups A and B determined the order of use of bags ‘X’
The regular distribution analysis was performed
and ‘Y’ for the first or second test respectively. All ran-
according to Kolmogorov-Smirnov and to Shapiro-Wilk.
domisation steps were performed according to lists pro-
The Wilcoxon signed-rank test was used to compare the
vided by a statistical institute (Data collection, Statistics,
two related samples XI and placebo. A P value <0.05
Risk assessment; Austrian Agency for Health and Food
was considered statistically significant.
Safety) before starting package preparation and oral prov-
The same statistical tests (Kolmogorov-Smirnov and
ocations using the random sample SAS (9.2; SAS Inc.,
Wilcoxon) were used for the VAS symptom scores for
bloating, abdominal pain and nausea.
Data were analysed with SAS 9.2 and SPSS version 19
Two tests were performed at an interval between 4 daysand 21 days. One day prior to each visit, subjects were
asked to consume a lactose- and fructose-restricted diet.
Sixty-five patients (15 men and 50 women; mean age 43.3
All the subjects fasted overnight and were not allowed to
(s.d. = 14.4), range: 21–73 years) participated in the
smoke 12 h before the test. The fasting end expiratory
study. No subject dropped out from the trial. One of 65
breath H2 concentration (termed 0 min) was measured
tested subjects did not complete the symptom question-
using a Gastro+ Gastrolyser (Bedfont Scientific Ltd,
naire. In the current study, peak increases in end expira-
Rochester, England) which has a sealed electrochemical
tory hydrogen concentrations after fructose did not
sensor specific for H2. Immediately thereafter subjects had
exceed 20 ppm in 19 patients after placebo; after inges-
to take three capsules ‘X’ or ‘Y’ and then to ingest 25 g of
tion of XI, four of these patients had an increase in breath
fructose freshly dissolved in 100 mL of mineral water
hydrogen concentration after fructose exceeding 20 ppm.
taken from one single production batch which was added
On the other hand, XI decreased peak hydrogen excretion
to the plastic bottles which contained the fructose. Sub-
after fructose to less than 20 ppm in 16 patients who had
jects were advised to drink the solution within 5 min.
an increase exceeding 20 ppm after placebo.
Thereafter, end expiratory breath H2 concentration was
The median AUC after 25 g of fructose was 885 ppm/
recorded every 30 min for the first 2 h, then every 60 min
240 min (25th percentile 60, 75th percentile 4009) in the
for the next 2 h (for a total of 240 min) by a study physi-
XI group, and 2071 ppm/240 min (25th percentile 487,
cian (M. A.-M.). The second test was performed identi-
75th percentile 5898) in the placebo group (Table 1, Fig-
cally with the remaining capsules (‘Y’ or ‘X’).
ure 1). This difference in AUC was statistically signifi-cant (Z-value À3.585, two-sided asymptotic significance;
P = 0.00) in favour to the XI group.
After plotting the breath H2 concentrations (in ppm) vs.
There were marked inter-individual differences in
time for the 4 h observation period the area under the
scores for all three symptoms, covering the whole range
curve (AUC) was calculated for each subject for both
of the VAS scale from 0 to 10. In general, bloating was
tests and expressed as ppm/240 min. Fasting breath H2
scored to be the most bothersome symptom although its
concentration at 0 min was used as the baseline for
median score was only 0.8 (range: 0–8.2) in the placebo
AUC determination. For example, if basal breath hydro-
group and 0.2 (range: 0–10) in the XI group. This differ-
gen concentration was 5 ppm, the AUC was calculated
ence failed to reach statistical significance (Z = À1.935,
from the area under the curve exceeding this baseline of
P = 0.053). Median scores for abdominal pain and nau-
sea were significantly lower after XI as compared withplacebo
P = 0.005 respectively) (Table 2, Figure 2).
The symptoms bloating, nausea and abdominal painwere assessed individually before ingestion of the test
solutions and at each time of breath hydrogen measure-
Xylose isomerase (EC 5.3.1.5, CAS 9023-82-9), also
ment by visual analogue scale covering a range of 0
referred to as glucose isomerase, is an enzyme that cataly-
ses the chemical reaction D-xylose ⇌ D-xylulose and
Xylose isomerase in fructose malabsorption
AUC, area under curve; n, number; s.d., standard deviation; Min, minimum; Max, maxi-mum.
sule design has been used in the past for protecting
drugs from the acidic environment of the stomach,allowing gastric emptying of micropellets with a size
between 2 mm and 3 mm through the pylorus with food
and quick release of the enzymes in the neutral environ-
ment of the duodenum.29 Ingested watery solutions ofpoorly absorbable carbohydrates start reaching the
cecum after an oro-cecal transit time of 60 ± 7 min
[mean + standard deviation (s.d.)] in symptomatic and
96 ± 16 min (mean + s.d.) in asymptomatic persons32;
during this time the enzyme presumably would catalyse
the isomerisation of fructose to glucose, which is actively
absorbed by the intestinal mucosa via the SGLT-1 trans-porter.33 We hypothesised that due to active absorption
Figure 1 | Significant reduction (P = 0.00) in the breath
of glucose, the equilibrium of the isomerisation process
hydrogen area under curve (AUC; ppm/240 min) in
would be pushed towards glucose. As a consequence, less
the XI group (n = 65) compared with the placebo
fructose would enter the colon and be metabolised by
group (n = 65) (logarithmic scaling). The median
colonic bacteria, resulting in less hydrogen production,
values for XI and placebo group were 885 and
and possibly also reduced symptoms related to incom-
To prove this hypothesis, we studied the effect of XI
fructose ⇌ glucose.7 It has been used since 1957 industri-
on breath hydrogen excretion after ingestion of fructose.
ally to convert glucose to fructose in the manufacture of
Our study group consisted of patients who had presented
high fructose corn syrup and is one of the highest tonnage
for the evaluation of abdominal symptoms and in whom
industrial enzymes.30, 31 Glucose isomerase enzyme prepa-
fructose malabsorption was established within the previ-
rations are used in the production of high fructose corn
ous 12 months by the use of a fructose hydrogen breath
syrup described in § 184.1866 of the FDA GRAS Notice
test. It has been demonstrated in the past, that this
Inventory. They are derived from recognised species of
group may include patients with functional gastrointesti-
precisely classified nonpathogenic and nontoxicogenic
nal disorders who are more likely to develop symptoms
microorganisms, including Streptomyces rubiginosus, Acti-
at lower doses of ingested fructose,1 possibly representing
noplanes missouriensis, Streptomyces olivaceus, Streptomy-
visceral hypersensitivity which has been demonstrated in
ces olivochromogenes and Bacillus coagulans, that have
been grown in a pure culture fermentation that produces
Although we had originally planned to repeat the
fructose hydrogen breath test immediately before start of
As XI is also able to convert poorly absorbable fruc-
the study, this repeat procedure was declined by the
tose to well-absorbable glucose in vitro, we hypothesised
ethics committee of our university, to spare patients of
that this enzyme could be used for conversion of excess
the symptoms associated with an oral fructose load.
fructose to glucose in the human small intestine in vivo.
Unexpectedly, it turned out that in the course of the
To test this hypothesis, capsules containing enteric
study in 29% of patients the increase in end expiratory
coated micropellets of XI were manufactured. This cap-
hydrogen concentration was less than 20 ppm. This
Table 2 | Symptom scores forabdominal pain, bloating and
n, number; s.d., standard deviation; Min, minimum; Max, maximum; XI, xylose isomer-ase.
excess hydrogen production due to fructose malabsorp-
tion. The dose of 25 g fructose in our study is on thelower end of the dose range which has been used by
different authors.1 At this dose, patients with functionalgastrointestinal disorders are more likely to develop
symptoms than normal subjects. This is relevant for thepotential clinical application of our study results,
because if a drug treatment would be considered in
fructose malabsorption, this should be limited to
patients who develop symptoms, regardless whether ornot symptoms may be aggravated by an underlying vis-
ceral hypersensitivity. Since pharmacological treatment
options for functional gastrointestinal disorders are very
limited detection of small amounts of fructose beingmalabsorbed has a clinical relevance, directing attention
Figure 2 | XI significantly reduced symptom scores for
at excluding even small amounts of fructose from the
abdominal pain (P = 0.009) and nausea (P = 0.005),
but not for bloating (P = 0.053), in 64 patients who
In this study, oral supplementation of XI revealed a
received XI or placebo on two study days.
statistically significant decrease in breath hydrogenexcretion over a 4 h period after ingestion of fructose,as compared with placebo. Decrease in the area under
suggests a considerable intraindividual variability of
the breath hydrogen curve after XI suggests that XI
breath hydrogen excretion, which needs future attention
catalysed the isomerisation of fructose which resulted in
in trials using breath hydrogen test. In this context, it
a lower amount of fructose reaching the colon. It is
has to be kept in mind, that the cut off value of 20 ppm
reasonable to end the measurement period at 4 h since
which is commonly used clinically to establish malab-
breath hydrogen excretion after ingestion of poorly
sorption is only one point on the hydrogen excretion
absorbable carbohydrates reaches its peak before that
curve, plotted as hydrogen excretion over time. Consid-
time. In a previous study on lactose malabsorption,
erably more information on colonic gas production and
hydrogen peak occurred at 160 ± 16 min (mean + s.d.),
excretion can be gained from cumulative flatus collec-
regardless whether patients were symptomatic or not,
tions or AUC.11, 36 In the current study, AUC was used
and in a study with cumulative measurement of anal
to assess colonic hydrogen accumulation over the
curves flattened after 210–240 min in the majority of
In those patients who did not exceed the cut off
level of 20 ppm, there was still a demonstrable increase
A surprising finding in our study was, that, although
in the breath hydrogen over the baseline, indicating
patients had presented in the preceding year for evaluation
Xylose isomerase in fructose malabsorption
of abdominal symptoms, indicating that they were both-
Future studies will have to demonstrate whether XI is
ered by their symptoms enough to warrant diagnostic
effective with carbohydrate mixtures which are present in
evaluation at a tertiary care centre, only few patients had
fructose containing food, and to assess long-term effects
high scores on the VAS assessment of symptom severity
and safety and to identify patients who most benefit from
during this study. This may indicate a large intra-
the treatment. The presence of fructose malabsorption in
individual variability in the severity of symptom scores
patients with functional gut symptoms may represent not
presumably associated with incomplete fructose absorp-
only an opportunity for dietary manipulation, as stated by
tion. Although median symptom scores therefore were
Barrett et al.,17 but for additional application of XI to
quite low in our study, scores for nausea and abdomi-
assist in the amelioration of such symptoms.
nal pain were significantly improved by XI. There was
Isomerisation of fructose by XI may also be useful to
no significant effect on bloating after administration of
avoid high fructose uptake into the body. Further studies
XI; however, it has been shown in the past that repro-
are required to confirm this hypothesis.
ducibility of symptoms associated with large bowel dila-tation is higher with better characterised symptom of
pain as compared with the less specific symptom of
Declaration of personal interests: P. Komericki has served
as a speaker for Sciotec Diagnostic Technologies, Tulln,
In summary, our proof of concept study has demon-
Austria, and M. Akkilic-Materna has received research
strated that in patients with incomplete fructose absorp-
funding from Sciotec Diagnostic Technologies, Tulln,
tion, oral administration of xylose isomerase can reduce
Austria. Declaration of funding interests: This study was
breath hydrogen excretion in vivo and reduce symptoms
funded in full by Sciotec Diagnostic Technologies, Tulln,
associated with fructose malabsorption.
self-reported severe lactose intolerance.
2. Rumessen JJ. Fructose and related food
absorption, and clinical implications.
9. Szilagyi A, Malolepszy P, Yesovitch S,
Porter JL, Schiller LR, Fordtran JS.
Scand J Gastroenterol 1992; 27: 819–28.
3. Elliott SS, Keim NL, Stern JS, Teff K,
diarrhea. J Clin Invest 1990; 86: 1936–44.
16. Gibson PR, Shepherd SJ. Personal view:
10. Hammer HF, Santa Ana CA, Schiller LR,
Pharmacol Ther 2005; 21: 1399–409.
absorption: quantification of its effect
bacterial fermentation of carbohydrates.
Gastroenterol Hepatol 2007; 5: 959–63.
caused by carbohydrate malabsorption.
19. Dills W. Protein fructosylation: fructose
7. Beyer PL, Caviar EM, McCallum RW.
carbohydrate–free diet in the rat. Nutr
22. Yilmaz Y. Review article: fructose in
diabetic patients. Gastroenterology 1984;
non-alkoholic fatty liver disease. Aliment
29. Porter SC, Ridgway K. The permeability
malabsorption–effect of simethicone.
conversion of D-glucose to D-fructose.
isomerization of D-xylose to D-xylulose.
Arch Biochem Biophys 1954; 48: 120–9.
27. Bhosale SH, Rao MB, Deshpande VV.
nitric oxide “Guanosine 3’, 5’ – cyclic
Pharmacy and Therapeutics Committee Meeting of September 13, 2005 Kellogg Center, Michigan State University MEETING MINUTES I. Welcome and Introductions, and Approval of June 7, 2005 Meeting Minutes The meeting was called to order at 6:00PM by Richard Slaughter, Chair. In attendance were Richard Slaughter, MSc., D.VanLoo, PharmD., M. Robins DO, G. Perri, MD, Jonathan Arend, Ph
To Change the colour of the Background Click on the Button Below. Antique white Bisque silver slate green cadet blue white azure OriginalConduct of Pension Adalats on Railways. The intention of conducting Pension Adalats is to examine the grievances ofpensioners so as to redress the same by taking on the spot decisions and to obviatethe delays, if any, in the settlement of their dues. Such a st
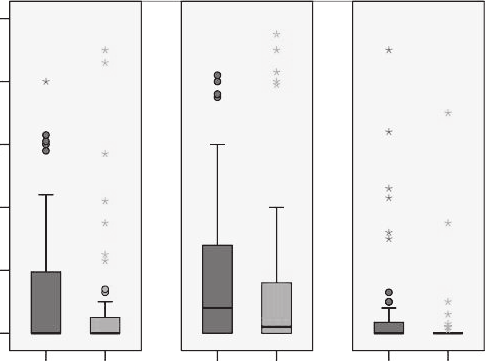 Table 2 | Symptom scores forabdominal pain, bloating and
n, number; s.d., standard deviation; Min, minimum; Max, maximum; XI, xylose isomer-ase.
Table 2 | Symptom scores forabdominal pain, bloating and
n, number; s.d., standard deviation; Min, minimum; Max, maximum; XI, xylose isomer-ase.