Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
Pain-spine.com
Patient Name: Insurance Information Primary Insurance: Secondary Insurance: Worker’s Comp Insurance * Motor-Vehicle Accident Insurance (circle one) I understand and agree that all services rendered are charged directly to me and that I am personally responsible for payment in the event that my claim for Workers Compensation benefits, Auto Claim, or Insurance is denied.CONSENT FOR THE USE AND DISCLOSURE OF HEALTH INFORMATION FOR TREATMENT, PAYMENT OR HEALTHCARE OPERATIONS ACCORDING TO HIPPA LAWS
I, _____________________________________, understand that as part of my health care, Pain and Spine Institute originates and maintains paper and/or electronic records describing my health history, symptoms, examination and test results, diagnoses, treatment and any plans for future care or treatment. I understand that this information serves as:
A basis for planning my care and treatment
A means of communication among the many health professionals who contribute to my care
A source of information for applying my diagnosis and surgical information to my bill
A means by which a third-party payer can verify that services billed were actually provided
A tool for routine healthcare operations such as assessing quality and reviewing the competence of
. It is the policy of this office to remind patients of their appointments. We may do this by
telephone, e-mail,U.S mail, or by any means convenient for the practice and/or as requested by you. We may send you other communications informing you of changes to office policy and new technology that you might find valuable or informative.
You agree to bring any concerns or complaints regarding privacy to the attention of the office
We agree to provide patients with access to their records in accordance with state and federal laws.
You have the right to request restrictions in the use of your protected health information and to
request change in certain policies used within the office concerning your PHI. However, we are not obligated to alter internal policies to conform to your request
We may change, add, delete or modify any of these provisions to better serve the needs of the both
I understand and have been provided with a Notice of Information Practices that provides a more complete description of information uses and disclosures. I understand that I have the following rights and privileges:
The right to review the notice prior to signing this consent
The right to object to the use of my health information for directory purposes The right to request restrictions as to how my health information may be used or disclosed to carry
our treatment, payment or health care operations. I understand that Pain and Spine Institute is not required to agree to the restrictions requested. I understand that I may revoke this consent in writing, except to the extent that the organization has already taken action in reliance thereon. I also understand that by refusing to sign this consent or revoking this consent, this organization may refuse to treat me as permitted by Section 164.506 of the code of Federal Regulations. I further understand that Pain and Spine Institute reserves the right to change their notice and practice and prior to implementation, in accordance with Section 164.520 of the Code of Federal Regulations. Should Pain and Spine Institute change their notice, they will send a copy of any revised notice to the address I’ve provided. I understand that as part of this organization’s treatment, payment or health care operations, it may become necessary to disclose my protected health information to another entity, and I consent to such disclosure for these permitted uses, including disclosures vial fax. I fully understand and accept / decline the terms of this consent.
__________________________________ ____________________ Patient’s Signature Date FINANCIAL POLICY
Thank you for choosing Pain and Spine Institute as your healthcare provider. We are committed to providing the best medical care possible. Please understand that payment of your bill is considered a part of your treatment. The following statement explains our Financial Policy which we ask you to read, sign and return to us prior to your treatment.
All patients should provide accurate and complete personal and insurance information prior to being seen by the doctor. All applicable co-pays, personal balances, both current and prior, are due at the time of serviceWe accept cash, personal checks, MasterCard and Visa. Regarding Insurance We participate on most insurance plans. Read and understand your insurance policy. Your policy is a contract between you and the insurance carrier. Read it, understand it and ask questions. DO NOT ASSUME YOUR POLICY AUTOMATICALLY COVERS EVERYTHING. Even different policies from the same insurance company can have different requirements. It is YOUR responsibility to know what your policy covers and what it does not. Always carry your insurance card with you. You will need it for all office visits and may need it in case of an emergency. Some insurance carriers require we verify your coverage for each office visit. Without this information, we may have to reschedule your appointment or you may have to pay at time of service. Some carriers require a referral or prior authorization from your primary care provider. It is YOUR responsibility to obtain this referral. IF YOU DO NOT HAVE A REFERRAL OR PRIOR AUTHORIZATION, YOU WILL BE RESPONSIBLE FOR PAYMENT OR WE WILL RESCHEDULE YOUR APPOINTMENT. Usual and Customary RatesWe are committed to providing the best treatment for our patients and we charge what we believe to be reasonable and customary fees for our region and specialty. If your insurance company uses a different fee schedule, you will be responsible for any balance remaining. Past Due AccountsOver due accounts will be referred to a collection agency. Legal fees that we pay to secure past due balances will be added to your account. Returned Checks For checks returned to us for non sufficient funds by your bank, we will charge a $25.00 fee. Insurance DenialsIn the event that any date of service is denied by the insurance carrier for ineligibility or no referral, the remaining balance will be turned over to patient responsibility. Insurance Non-paymentIf a claim is forty-five (45) days old and there has been no response from the insurance carrier, the balance due will be turned over to patient responsibility for payment. Please contact our Billing Department if you have any questions or concerns at (815) 729-0700
I have read the Financial Policy. I understand and agree to the Financial Policy.
___________________________ _________________ Patient Signature Today’s Date Narcotic Prescribing Policy ***PLEASE READ*** **VERY IMPORTANT**
The prescribing of narcotics for chronic pain is a challenge under the best of circumstances due to issues of substance abuse, addiction, legal requirements, and the historical high percentage of drug abusers intermingled with the chronic pain population, and other factors. In order to continue prescribing narcotics to patients, it is necessary to have tight controls and rigid rules established to eliminate those who procure narcotics for illegal purposes or for substance abuse, to protect the privileges of our practice to prescribe, maintain the health and welfare of the patients, and to obey the laws under which we operate, both federal and state.
Narcotics are but one avenue of pain therapy and never represent the sole method of pain control. Narcotics have potential for addiction and substance abuse, are diverted by some for sale or for improper routes of administration or shared with others. Narcotics may produce dependence, tolerance, and addiction. Side effects or narcotics include sedation, respiratory depression, swelling in the feet, dental decay acceleration, hives, itching, slurred speech, impaired thinking and function to the point a person may be dangerous when driving or operating machinery when taking narcotics, ICU admission, coma and death. For reasons, we reserve the right to change to a non-narcotic therapy at any time it is medically indicated. We also reserve the right to insist on an in or out patient treatment for narcotic dependence. ***There is no implied or expressed patient right to narcotic therapy in a physician’s office or in a hospital. ***
EXPECTATIONS OF APPROPRIATE PATIENT BEHAVIOR AND RESPONSIBILITY:
Our medical practice will be the only entity prescribing narcotics for chronic pain. If there is acute pain for a new condition for which the patient seeks care elsewhere, out practice must be called to let us know of the other physician’s prescribing, at that time we may adjust your chronic pain medications. If it is discovered patients are chronically receiving narcotics from multiple physicians, we will immediately discontinue medication prescribing and notify pharmacies and other treating physicians of the patient’s substance abuse, please be aware you will be subject to immediate discharge as well. In certain states, there may be laws prohibiting patients from obtaining narcotics under false pretenses (eg. Seeing multiple physicians for narcotics without notifying the other physicians), In all states, there are laws which prohibit sharing of prescription narcotics with others, changing or altering a narcotic prescription in order to obtain early refills or an increased quantity of narcotics, or the selling or trading of narcotics. These events are felonies under federal law and are not protected by the patient - doctor professional relationship. Therefore any information we receive regarding the commission of a felony will be reported to the police or US Drug Enforcement Agency.
A.) One pharmacy must be used for scripts. If that pharmacy does not have the prescription, then we expect patients to go to another
pharmacy rather than receive a partial refill on the narcotic.
B.) Refills of scripts for narcotics are only performed during scheduled office visits. We will not call in narcotic prescriptions nor write
prescriptions at the time of patient procedures or during non-office hours. C.) There are no early refills. The patient is expected to make the prescription quantity last until the next office visit typically your
prescription is for a 30 day supply, if you are unsure ASK. We do not refill prescriptions that were lost, stolen, spilled, eaten by the cat etc…*****The responsibility for safekeeping of these medications lies solely with the patient. Therefore, each patient is expected to keep a lock box or location for safekeeping for the main supply of the narcotic medication instead of carrying around the entire month’s supply. ***** D.) On request of our medical practice, the patient will submit a urine sample to a designated laboratory for testing to assure the medications
being prescribed are actually in the urine. On request, a pill count may be necessary and the patient has to bring in the narcotics to be counted by our staff. For patients out of town, it is acceptable to have a local pharmacist perform a pill count and we will call the pharmacist to verify.
E.) There will be no alcohol or illicit drug use while taking narcotic medications. Discovery of such via internal or external sources may result
in discontinuation of narcotics immediately and leave you subject to immediate discharge.
F.) It is the policy of our practice that driving or operating machinery while taking narcotics may have untoward consequences, and if the
patient elects to operate machinery or equipment, they do so at their own risk of injury or death.
G.) Sudden cessation of narcotics may cause injury to the patient only in very rare circumstances however, sudden cessation of high dose
narcotics will result in severe abdominal cramping, severe anxiety, rapid heart rate, elevated blood pressure, nausea, etc. Therefore it is prudent to use the narcotics as prescribed rather than running out early or violation of our policies which will result in sudden cessation of narcotic prescribing.
H.) Please be aware you may be asked to submit a urine sample before any narcotics will be prescribed. It is also possible you may have
a brief waiting period before medications can be prescribed pending results of screen. If you are a cash patient there is a $50.00 fee that MUST be paid in CASH before your next visit.
The patient will be told that under no circumstances is the patient to operate heavy machinery while under the influence of opiate medications that may impair their judgment. Such activities may result in severe civil and/or criminal penalties. The patient will be carefully instructed regarding the risk of the use of opiates in combination with other medications or substances that may depress the CNS including anxiety, muscle relaxants, narcotics, ETOH, illicit drugs, etc. The patient will also be advised that the combination of these medications may have serious adverse consequences including respiratory depression, coma, and death (accidental poisoning). The patient agrees to inform Pain & Spine Institute (PSI) regarding any medications prescribed by other physicians that fall into the classes mentioned above, and if they are not sure what type of medication it is, notify PSI immediately before taking new medications. The patient expresses understanding that, if prescribed these types of medications whether by a physician in this office or another physician, they must be extremely cautious the first time they use these medications in conjunction with each other. The patient also expresses understanding that they must be extremely careful at all times utilizing these medications together because of their additive and possible synergistic effects.
We do fill 90 day supply mail order prescriptions if it is for narcotic medication.
4. REASONS NARCOTICS MAY BE IMMEDIATELY DISCONTINUED AND POSSIBLE DISCHARGE: A.) Evidence of prescription alteration or fraud or solid evidence presented to our clinic that the patient has been selling the
narcotics, sharing narcotics with others, injection of oral or trans dermal narcotics.
B.) Threats of legal action or violence made against any of our staff in order to obtain narcotics, etc. In such cases the police will be
called immediately to report a felony drug diversion or attempted extortion, and the patient will be immediately discharged from out
practice. Committing a narcotics related crime is not protected by doctor-patient privilege and will not be tolerated Period!
C.) Refusal to take a urine drug screen of the request, refusal to bring in medications for a pill count when requested, a positive drug
test for illicit drug use or narcotics not prescribed by our clinic, or a negative urine drug screen for narcotics we are prescribing will be
met with discontinuation of narcotics.
D.) External source confirmation of “doctor shopping” or obtaining narcotics chronically from multiple physicians simultaneously
will require sudden narcotic discontinuation.
E.) Impairment of the patient to such a degree that in the opinion of our medical practice that the patient poses a risk to themselves or
to others may require narcotic discontinuation.
F.) Using suicide as a threat or suicidal attempts will result in immediate and complete discontinuation of all medications with the
5. REASONS NARCOTIC THERAPY MAY BE MODIFIED OR REDUCED OR POSSIBLE DISCHARGE FROM CLINIC:
Reasons for which narcotic therapy will be modified or discontinued with the possibility of a drug taper or non-narcotic withdrawal medication
administration: loss of scripts, overuse of medications, failure of escalating doses of narcotics provide relief in the absence of any demonstrable worsening findings on clinical examination including x-rays/MRI, arrest for driving while impaired, arrest for any alcohol related offense,** excessive frequent calls to our clinic regarding chronic pain issues or medication refills, prevarication regarding prior treatment and substance abuse, canceling appointments for procedures but showing up for office visits, failure to participate in the integrated therapies of our practice, etc.
Chronic pain is just that… it is a long standing problem which has been
present for months or years. It is important that patients keep a long term perspective on the treatment of this condition. Frequent calls to our clinic for non-urgent issues, frequent requests of narcotics changes outside appointment times, or histrionic behavior in the absence of new conditions may make patients non-candidates for continued therapy in our center. However, in the case of potentially life threatening emergencies such as severe respiratory depression and over sedation, our physicians may be contacted 24 hours a day by calling the designated number and asking for the Pain Physician on call. Calls made for non-emergent issues or issues which should be handled during office hours may jeopardize continued treatment in our practice. Evaluation of the Patient---A medical history and physical examination must be obtained, evaluated, and documented in the medical record. The medical record should document the nature and intensity of the pain, current and past treatments for pain, underlying or coexisting diseases or conditions, the effect of the pain on physical and psychological function, and history of substance abuse. The medical record also should document the presence of one or more recognized medical indications for the use of a controlled substance. Treatment Plan---The written treatment plan should state objectives that will be used to determine treatment success, such as pain relief and improved physical and psychosocial function, and should indicate if any further diagnostic evaluations or other treatments are planned. After treatment begins, the physician should adjust drug therapy to the individual medical needs of each patient. Other treatment modalities or a rehabilitation program may be necessary depending on the etiology of the pain and the extent to which the pain is associated with physical and psychosocial impairment. Informed Consent and Agreement for Treatment---The physician should discuss the risks and benefits of the use of controlled substances with the patient, persons designated by the patient or with the patient’s surrogate or guardian if the patient is without medical decisions-making capacity. The patient should receive prescriptions from one physician and one pharmacy whenever possible. If the patient is at high risk for medication abuse or has a history of substance abuse, the physician should consider the use of a written agreement between physician and patient outlining patient responsibilities, including urine/serum medication levels screening when requested; number and frequency of all prescription refills; and reasons for which drug therapy may be discontinued (e.g. violation of agreement). Consent for narcotic treatment by our practice is given on the initial visit as part of the paperwork packet. Periodic Review---The physician should periodically review the course of pain treatment and any new information about the etiology of the pain or the patient’s state of health. Continuation or modification of controlled substances for pain management therapy depends on the physician’s evaluation of progress toward treatment objectives. Satisfactory response to treat may be indicated by the patient’s decreased pain, increased level of function, or improved quality of life. Objective evidence of improved or diminished function should be monitored and information from family members or other caregivers should be considered in determining the patient’s response to treatment. Our medical practice’s periodic patient review is usually 1 month for initial patients or during changes in therapy, 2-3 months for chronic stable Schedule III (hydrocodone/codeine/Darvocet) opiate therapy in addition to physical therapy and psychological treatment where appropriate, and review may be as often as one week or less for high risk patients or those with a substance abuse history. Patients receiving Schedule III medications (Oxycontin, Duragesic, MS Contin, MS IR, Kadian, Avinza, dilaudid, methadone) are seen at monthly intervals.
General Policies Our Mission At Pain and Spine Institute, we offer a multidisciplinary evaluation/treatment for acute and chronic pain syndromes, as well as cancer pain. Our goal is to achieve maximum pain relief for the greatest length of time possible and to facilitate the return to a normal productive life. Office Hours Monday – Friday 7:30am – 5:30pm Appointments Please call during regular clinic hours. If you are unable to keep your appointment, please let us know as far in advance as possible. If you call to cancel with less than 24 hours notice you may be subject to a late cancellation fee of $35.00 and if you NO SHOW for your scheduled appointment you will be charged $50.00, in addition if you chronically NO SHOW or cancel your appointment 3 times or more you will be discharged from our practice. Remember it is the responsibility of the patient to be at your scheduled appointment, reminder calls are a courtesy. If you are more than 10 min. late you will be asked to reschedule. Phone Calls The reception desk will return phone calls in order of urgency. All calls will be returned within 24 hrs Prescription Refills Prescription refills will only be given during regular office hours with a 48 hour advance notice. No refills/new prescriptions will be given on weekends or on Fridays. STRICTLY ENFORCED: please be aware we do not give out 90 day supply of controlled medication no exceptions! Notice of Privacy Practices The Pain & Spine Institute respects your privacy. We understand that you personal health information is very sensitive. Financial Policy Preferred method of payment is cash, but we will accept personal checks, debit cards, master card, and visa. Private Pay patient’s cash or credit card only! Payment is due in full at time of service no exceptions! Insurance It is the patient’s responsibility to contact your insurance to make sure you are eligible for services. Co-Pays Insurance requires that co-payments are collected at the time of service. If you cannot provide your co-payment we are required to reschedule your appointment. Appropriate Conduct We have a Zero tolerance policy for any patient who behaves inappropriately to clinical staff, office staff and physicians will be discharged from our clinic immediately (ex: cursing, violence, verbal threats etc.) Medical Forms: Pain & Spine Institute management charges a flat fee of $50.00 (you may be subject to a FCE test to determine your functional capacity before the forms can be filled out*please note this may or may not be covered by your insurance) which applies to forms that need to be completed and signed by the physician. Forms will take from 7 – 10 business days to be completed. Forms not accompanied with payment will be returned incomplete. We must have payment before the forms are filled out so we can block adequate time for the doctor to complete forms. In addition these forms must be turned in to the doctor at your scheduled appointment for disability determination. Delinquent Accounts If your account is delinquent you will receive a letter from our Billing Department notifying you that you need to make a payment to clear your account or if you can not pay the whole bill we expect you to contact the billing department to make payment arrangements. If payment is not made, your account will be turned over to a collection agency, in addition you will no longer be offered services until this has been taken care of. Narcotics Prescribing and General Office Policy Contract I, ____________________________________ have read and understand the Narcotics prescribing and
general office policies. In addition, if I break any terms of the agreement, The Pain & Spine Institute has the right to discharge me from the practice immediately.
I am also giving my physician (Dr. Samir Sharma MD or Dr. Udit Patel DO) permission to view my medication history.
Patient’s Signature ______________________________________Date: __________________
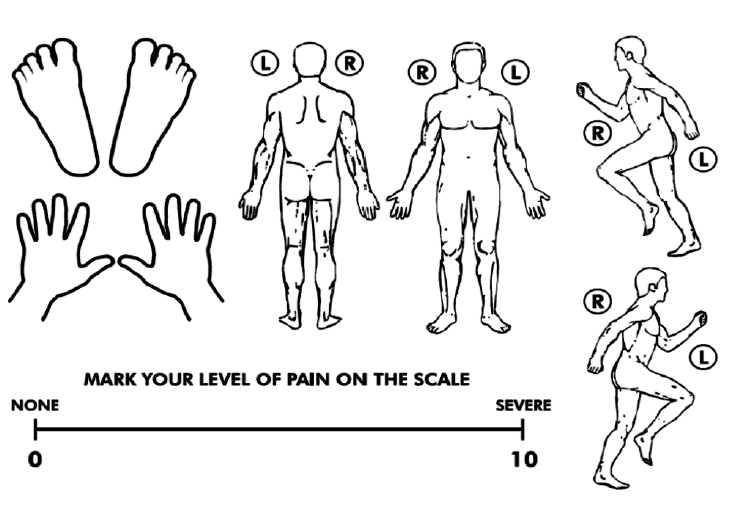
***Pharmacy Name: Address: Description of Pain Circle Words That BEST Describe Your Pain History of Present Illness
Is this a Work Injury or Auto Injury? (pleas circle) Yes or No
How did the injury or pain occur (Use back of page if more space is needed)?
How has your pain or its treatment affected your daily activities or relationship with family/friends
___________________________________________________________________________________________________________
Is there anything that makes the pain better?
Where in your body does the pain radiate to?
Have you missed work due to your condition?
Are you, or could you possibly be pregnant?
Previous Treatments (eg: Physical Therapy/Chiropractic/Occupational Therapy/ Massage) Type of Therapy
Home Exercise Program? (Please circle) YES or NO? If so, when did you start?_____________________________________________
_____________________________________________________________________________________________________________
_____________________________________________________________________________________________________________ Previous Injection Therapy Type of Injection? Injection Date/How long ago? Did the injection help? Length of relief? Tests performed to evaluate the problem (Circle all that apply) Review of Systems General (Constitutional) Gastrointestinal Respiratory Cardiovascular Musculoskeletal Skin (Integumentary) Genitourinary System Hematology Endocrine Neurologic Psychiatric
___________________________________________
___________________________________________
Relationship to Patient (mother, father, etc.)
drugs? (i.e. marijuana, heroin, cocaine, inhalants, etc.)
List any mental health issues that you have suffered or currently suffering from
My signature confirms that the answers to the above questions are accurate and stated to the best of my ability.
Parent or Guardian Signature (if under 18):
Protective I ntellectual Property Services, LLC Trade Secret MAXIMIZING THE VALUE OF YOUR INTELLECTUAL PROPERTY BY TRATEGIC INTELLECTUAL PROPERTY MANAGEMENT This newsletter contains current news about US patents and the US Patent and Trademark Office, current intellectual property (IP) court cases, domestic and international IP news and IP information of general interest t
GARA 2012 7 26 osteguna Mato KNEZ Geruza Atomikoen Estalketaren Teknikan (ALD) nazioarteko adituaKimikan aditua, Stuttgart-eko (Alemania) Max Planck Institute of Solid State Research-ean doktoretza burutu zuen2003an Kroaziako ikerlariak. Hamar urtetik gorako esperientzia du Italiako, Alemaniako, Koreako eta AEBetakoegoitzetan, eta aurten, Gaede Prize sari esanguratsua lortu du ALD teknikar
 Patient Name:
Patient Name: CONSENT FOR THE USE AND DISCLOSURE OF HEALTH INFORMATION FOR TREATMENT, PAYMENT OR
CONSENT FOR THE USE AND DISCLOSURE OF HEALTH INFORMATION FOR TREATMENT, PAYMENT OR  FINANCIAL POLICY
FINANCIAL POLICY Narcotic Prescribing Policy
Narcotic Prescribing Policy 4. REASONS NARCOTICS MAY BE IMMEDIATELY DISCONTINUED AND POSSIBLE DISCHARGE:
4. REASONS NARCOTICS MAY BE IMMEDIATELY DISCONTINUED AND POSSIBLE DISCHARGE: General Policies
General Policies Narcotics Prescribing and General Office Policy Contract
Narcotics Prescribing and General Office Policy Contract
 Description of Pain
Description of Pain Previous Treatments (eg: Physical Therapy/Chiropractic/Occupational Therapy/ Massage)
Previous Treatments (eg: Physical Therapy/Chiropractic/Occupational Therapy/ Massage) ___________________________________________
___________________________________________
___________________________________________
___________________________________________
 Relationship to Patient (mother, father, etc.)
drugs? (i.e. marijuana, heroin, cocaine, inhalants, etc.)
List any mental health issues that you have suffered or currently suffering from
My signature confirms that the answers to the above questions are accurate and stated to the best of my ability.
Parent or Guardian Signature (if under 18):
Relationship to Patient (mother, father, etc.)
drugs? (i.e. marijuana, heroin, cocaine, inhalants, etc.)
List any mental health issues that you have suffered or currently suffering from
My signature confirms that the answers to the above questions are accurate and stated to the best of my ability.
Parent or Guardian Signature (if under 18):