Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
Bitte initialen eingeben
Paper presented at the Partnership-Meeting: “ADHD among inmates in
prison” the 8th November 2004 in Bremen, Germany
Life-Course and Delinquency
To see the specific problematic of ADHD in inmates in prisons we have to
take into account the embeddedness of the relationship of ADHD anddelinquent be
In the last years, there is a strong focus on longitudinal studies incriminological theory and research. These studies focus on the
development of delinquent behaviour, starting as early as possible, to findthe risk factors for this trajectory. A so called ‘life-course perspective’ has
been developed (cf. Laub, Sampson 2001).
This longitudinal research is based on the assumption, that crime anddelinquency starts often before the age of criminal responsibility / liability
(like in: Germany: 14 years, Italy: 14 years; Norway: 15 years; Estonia:15 years) . And of course, the research looks for causes, risk factors and
social and personal problems in early life, on problem behaviour and
disorders, that will predict delinquent behaviour in later ages, but also, and this has been done in the last years, on the desistance of criminal
See for the description of ADHD, especially in the context of the prison: Matt 2004.
That means, the focus is not just on the deed, on the single offence, buton the question, how is delinquency based or linked to the life-course of
the -later- offender. That way, personal conditions and social
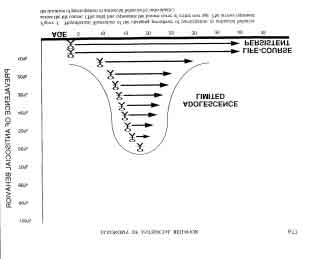
circumstances come into play in a longer time perspective. One starting point of the argumentation is the so called: age-crime curve.
It seems that delinquent behaviour is strongly related to age. The amountof delinquent behaviour varies strongly by age group. Terrie Moffitt (1993,
p. 677) used to make a theoretical model out of this insight:
In her model Terry Moffitt makes the distinction of adolescence limited
and life course persistent antisocial behaviour. This difference is of
most importance because it distinguishes two different groups and typesof delinquent behaviour with different pathways: One, the adolescent
limited, which has more to do with adolescence, peer orientation, beingyoung, and the transition to adulthood (and this means, it is an episode, it
is of brief appearance, one which will end getting older) and the other
one, the life-course persistent group, which start often rather early, and,in some cases, will not end with adulthood. (Empirically we have to add
that also some persistent offenders are starting their career lately,
sometimes even as an adult (that means, a late onset is of course alwayspossible)). This last group is in the focus of the criminological longitudinal
research, sometimes they are also called: chronic offenders, persistent
offenders or we talk about criminal careers. And an early onset is apredictor for a relatively long criminal career. This is the more problematic
group (and it is this group we find very often in prison).
In longitudinal research it is tried to do the first research (the first wave)
as early as possible (8 or 9 years in one, 3 years in another research, butsome, especially psychological one would even start before birth - and
then go on to come back to them in a one year or two year distance, justto see their development). Doing this kind of prospective research means
trying to find out, if and how different developmental pathways and
disorders can explain the (later) onset of delinquent behaviour. Researchhas found a list of many factors, and, of course, there are different lists,
Factors for delinquency:
conduct behaviour in early life, traumatic experiences,
Predictors of Delinquency - impulsivity
- attention problems- low school attainment
- parental conflict- an antisocial parent
These factors focus more on social and on personal problematic situations.
Especially the accumulation of negative experiences, of having more than
one burden, is something that leads to the onset and persistence of
A number of risk factors has been found: Also we can distinguish betweenindividual risk factors, family risk factors, but of course also school risk
Family risk factors - criminal and antisocial parents;
- large family size; - child-rearing methods (poor supervision, poor discipline, coldness and
rejection, low parental involvement with the child);
- abuse (physical or sexual) or neglect; and- parental conflict and disrupted families. Individual risk factors: ♦ personality, ♦ temperament, ♦ empathy, ♦ impulsiveness:
not considering consequences before acting, a poor ability to plan ahead,
risk-taking, and a poor ability to delay gratification.
In this list, Farrington shows that impulsiveness is one of the mostimportant individual factors that predict offending. And we see most of the
symptoms related to ADHD. In some longitudinal research there has been
some focus on ADHD, because it is of importance for the development ofdelinquency.
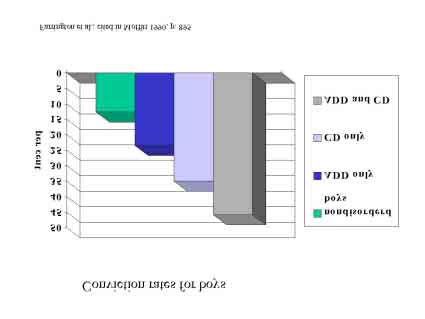
Many studies show that hyperactivity predicts later offending. Just one
“Whereas 12,6% of nondisordered boys were convicted, conviction ratesfor boys with ADD only, CD only, and both CD and ADD were,respectively, 23,5%, 35% and 45,8%” Moffitt 1990, p. 895.
In Germany, we do not find studies relating ADHD to delinquency. Thesituation here is, that the discussion just starts.
But, of course, we find some indications that it is of relevance.
Means or ratings of lack of impulse control
In their study about school bullying Lösel and Bliesener (2003) asked
school pupils and teachers to rate the dimensions. Bullying as a kind ofaggression is seen as an important misbehaviour, leading also to
delinquency. So it is this special group focussed on in school research. But
as we see, also attention problems play a role in the group of the ‘bullies’.
But I must add that as in most studies they did not use ADHD on the basis of a clinical diagnosis, but they only used some dimensions, some rating
scales to distinguish the groups, focussing on some symptoms of ADHD.
The relevant dimensions are of course, impulsivity and attention deficitdisorders.
And of course, they found statistically significant differences in thisgroups.
It is important in this perspective to see the development from the firstpersonal disorders to a negative career and later, to incarceration. This
can be conceptualised as an interaction of personal and social inadequate
behaviour and the social reactions on it. Missing social support,inadequate help (systems), difficult familial and social situation and, in the
further development, the forms of punishment by court, can increase theprocess.
The problem is to find an adequate conceptualisation and description of
this process, because most factors are just risk factors, that means, theyincrease the risk that delinquency occurs, but they do not determine this
development. So we find different models to describe the pathways.
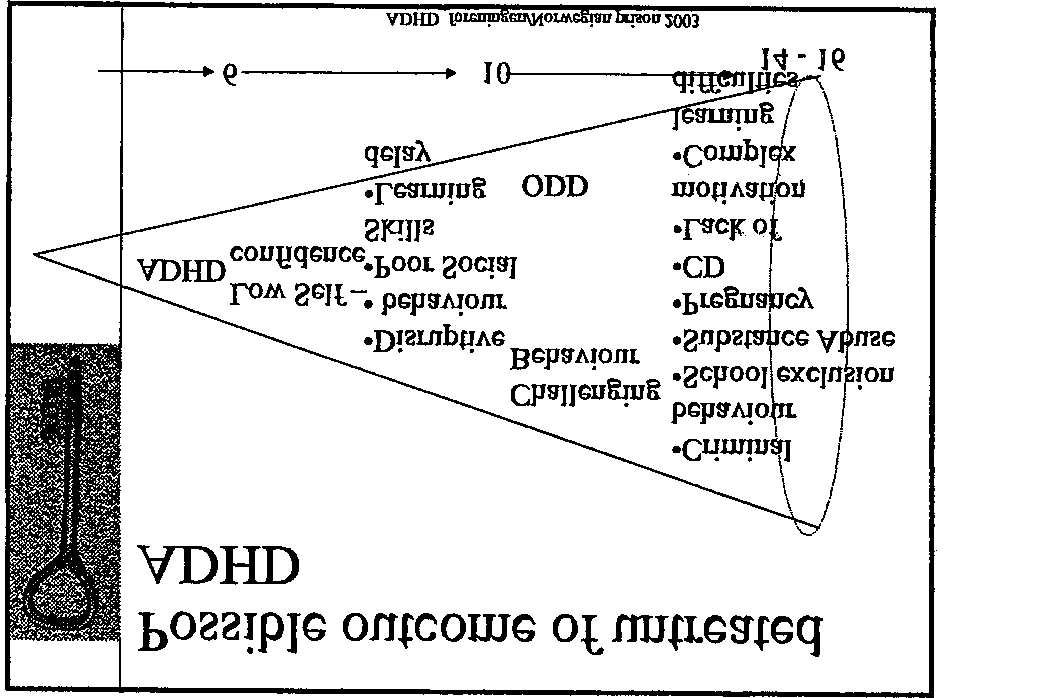
In this model, the focus is on ongoing activity or disorder. This means of course, too, that there must not be an involvement in the other
pathways, the other problem behaviour. Of course, there must be no co-morbidity.ncies or
This is also a reminder, that ADHD must not in all cases have negative concequences.
Some authors like to say that even some very famous person in history have been diagnosedpost mortem as having ADHD like: Hans Christian Andersen, Ludwig von Beethoven,Winston Churchill, Walt Disney, Thomas Edison, Albert Einstein, Benjamin Franklin et al.
In this model Bronder, shown at the ADHD meeting in HØnefoss in 2003,
the development of the disorders and the possible interaction with other
disorders (which can occur, but must not) is better conceptualised.
Another way of describing the development is described by Hampel and
In this model, the focus is more on co-morbidity. Than means, there canbe some changes in the symptoms over the life-course, being dominant in
different stages of development in the life-course.
Maybe, this model explains better why we rarely find a clear symptomatic
of ADHD in later life (in inmates in the prisons). Due to this model, thereare these changes in symptoms. So the basic ‘cause’ of the difficult
behaviour of the inmate has been once ADHD, but know it shows itself as
In the last 20 years there has been the discussion that ADHD does notend with adulthood. Now, in the German discussion it is said that about
50% of young adults show some further symptoms, that means with
impairments of daily activities. And, if we take the last model intoaccount, it will not be easy to diagnose them.
So we have different pathways of the role of ADHD in the life-course. Different ways of development:
• Desistance before adulthood • Persistance of the disease in full-blown state or in residual state with
decreasing hyperactivity and persisting attention-deficit
• Persistance of ADHD together with psychiatric disorders,
The last group is of most relevance for the discussion of delinquency and
But there are also some difficulties in diagnosis ADHD in adult persons:
Criteria of anamnesis for adults:
- personality disorder- affective disorder- anxiety disorder- tic – disorder- learning disorder- sleeping disorder
It is well known that comorbidity plays an important role in ADHD. About 2/3 of the diagnosed cases show some form of comorbidity. About half of
them show aggressive and antisocial behaviour. Other problems are drug
abuse, learning disturbances, bad schooling.
The drug topic seems of importance, especially the common appearanceof drug use and ADHD (in adults).
Wilms et al (2003) showed in a meta-analysis of studies that the risk for
drug abuse can be reduced by a rate of 50%, if the ADHD-person istreated early.
The topic of addicted adult persons (drug abuse) and ADHD as an
underlying cause, a comorbid condition, is also a new discussion in
Germany. Some researcher talk about a rate of 50% of ADHD of the drugusers, other studies found an abuse of alcohol (1/3) and drugs (1/5). The
discussion is in progress, so we do not have a good diagnostic procedureor an adequate therapy.
And we do not know much about the topic of self-medication with drugs
done by the ADHD persons. But this seems to be a real phenomena.
So their is a high risk for drug abuse for ADHD patients without treatment.
Another point in longitudinal studies is the question of desistance. Not
only what are the reasons to go into delinquency, but even more thosefactors leading to come out, to get straight. Taking into account the
question of comorbidity in ADHD, maybe also this factor is of importance. In this strand of research we find some factors:
Factors of Desistance
! Life events, that influence the life course
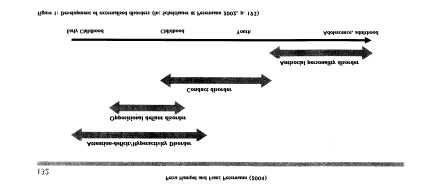
The longitudinal studies also show that we should not only look at riskfactors, but we should also look at protective factors. And these are also
the factors, that make desistance more probable. (Here it is of utmost
importance. the quality of social ties, be it in the family, in school, at
work, with friends; also important is a good integration into theworkplace, but also school qualification, motivation to learn, vocational
Only when we take into account this interaction between risk factors and
protective factors we are able to understand, why even in case ofcomparable bad living situations and risk factors only a part of these
Studies suggest that new social bonds or changing live conditions or
situations can generate turning points in the life-course. They can do so,but the must not do it. This depends heavily on the quality of these
changes, that would mean, only a good marriage or a good job will
change life, but also some changes of the self-conception, of somechanges in viewing oneself, changes in values are necessary (Maruna
There has to be some self-reform, initiated by themselves, by others, by
new experiences in school work or partnership. For persons with ADHD itmay be important to find the diagnosis, to get help in coping with the
symptoms, to get special training so that they will be enabled to have andto experience success. This is to start motivation to change the life course,
to start to get straight. This can and will be a very long process,
depending on how long the person has been involved in his deviant lifestyle, his criminal career, his history of disorder. Giving this new
experiences is an utmost important task to fulfil. The results, the changeof life-course, will not be seen at once, but mostly in later times. But small
So when the young persons come into prison, mostly they will have manyproblems:
Problems of inmates: - conduct behaviour
It is important to know about the ways they became the person they arenow, about their development, to find a good and adequate reaction to
the person, just to see what could be done with them.
Not to change this pathways, they will go on and on and on. It is of
utmost importance to look more closely on this type/group of inmates, thechronic offenders, the life persistent group, just to make a change in their
development possible. And to do this in prison, the only way to do this is
to make some experiences of success possible for them. This is not much,but it is something that is possible.
Literature:
Bronder, Knut Halvard: Living with ADHD. Vortrag. Hønefoss 2003Farrington, David: Developmental criminology and risk-focused
prevention. In: M. Maquiere et al. (Hrsg.): Oxford Handbook ofCriminology. Oxford 2002³, S. 657-701
Hampel, Petra; Franz Petermann: Aufmerksamkeits-/Hyperaktivitäts-
störungen. In: Kindheit und Entwicklung 13, 2004, S. 131-136
Laub, John, H.; Robert J. Sampson: Understanding desistance from crime.
Loeber, Rolf; David Farrington; Magda Stouthamer-Loeber; Welmoet B.
Van Kammen: Antisocial Behavior and Mental Health Problems. Explanatory Factors in Childhood and Adolescence. Mahwah 1998
Lösel, Friedrich; Thomas Bliesener: Aggression und Delinquenz unter
Jugendlichen. Untersuchungen von kognitiven und sozialenBedingungen. Neuwied 2003
Maruna, Shadd: Making Good. How Ex-Convicts reform and rebuild their
Matt, Eduard: Zappelphilipp im Gefängnis. Zum Umgang mit einer
schwierigen Klientel. In: Zeitschrift für Strafvollzug undStraffälligenhilfe 53, 2004, S. 76-81 (engl. translation: Fidget Philippin jail.
Moffitt, Terrie E.: Juvenile Delinquency and Attention Deficit Disorder:
Boys‘ developmental trajectories from age 3 to age 15. In: ChildDevelopment 61, 1990, S. 893-910
Moffitt, Terrie E.: Adolescence-limited and life-course-persistent antisocial
behavior: A developmental taxonomy. In: Psychological Review 100,1993, S. 674-701
Moffitt, Terrie E.; Avshalom Caspi; Honalee Harrington; Barry J. Milne:
Males on the life-course-persistent and adolescence-limitedantisocial pathways: Follow-up at age 26 years. In: Developmentand Psychopathology 14, 2002, S. 179-207
Sobanski, E.; B. Alm: Aufmerksamkeitsdefizit-/Hyperaktivitätsstörung
(ADHS) bei Erwachsenen. Ein Überblick. In: Der Nervenarzt 2004, S. 697-715
Wilems, Timothy E. et al.: A controlled clinical trial of Bupropion for
Attention Deficit Hyperactivity Disorder in adults. In: AmericanJournal of Psychiatry158, 2001, S. 282-288
In this model, Petermann et al. start from birth, going on with possible
problems, until it leads in young adulthood in delinquency. But one has toremind, that every step can have another way out, taking into account
possible protective factors. And it also shows that it is a long developmentwith many steps in between, until the stage of (a life-long persistent)
Naltrexone and Alcoholism Treatment Multiple Choice 1. Executive Summary and Recommendations Naltrexone has been approved as an adjunct to psychosocial treatment and should not be seen as a replacement for psychoso 2. Patients requiring narcotic analgesia are suitable candidates for naltrexone treatment. 3. Naltrexone interferes with nonopiod pain medications such as as ibuprofen
Gruppterapi Ahlin, G. (1996). Exploring Psychotherapy Group Cultures. Akademisk Avhandling, Stockholm: Karolinska Institutet. Burlingame, G. M., MacKenzie, K.R., Strauss, B. ( 2004). Small-group treatment: Evidence for effectiveness and mechanisms of change. I Lambert, M. J. (Ed.) Bergin and Garfield’s Handbook of Psycho- therapy and Behavior Change . New York: John Wiley & Sons.

 Paper presented at the Partnership-Meeting: “ADHD among inmates in
prison” the 8th November 2004 in Bremen, Germany
Life-Course and Delinquency
Paper presented at the Partnership-Meeting: “ADHD among inmates in
prison” the 8th November 2004 in Bremen, Germany
Life-Course and Delinquency
 That means, the focus is not just on the deed, on the single offence, buton the question, how is delinquency based or linked to the life-course of
the -later- offender. That way, personal conditions and social
circumstances come into play in a longer time perspective. One starting point of the argumentation is the so called: age-crime curve.
That means, the focus is not just on the deed, on the single offence, buton the question, how is delinquency based or linked to the life-course of
the -later- offender. That way, personal conditions and social
circumstances come into play in a longer time perspective. One starting point of the argumentation is the so called: age-crime curve.
 sometimes even as an adult (that means, a late onset is of course alwayspossible)). This last group is in the focus of the criminological longitudinal
research, sometimes they are also called: chronic offenders, persistent
offenders or we talk about criminal careers. And an early onset is apredictor for a relatively long criminal career. This is the more problematic
group (and it is this group we find very often in prison).
sometimes even as an adult (that means, a late onset is of course alwayspossible)). This last group is in the focus of the criminological longitudinal
research, sometimes they are also called: chronic offenders, persistent
offenders or we talk about criminal careers. And an early onset is apredictor for a relatively long criminal career. This is the more problematic
group (and it is this group we find very often in prison).
 Predictors of Delinquency
Predictors of Delinquency
 Family risk factors
Family risk factors
 In this list, Farrington shows that impulsiveness is one of the mostimportant individual factors that predict offending. And we see most of the
symptoms related to ADHD. In some longitudinal research there has been
some focus on ADHD, because it is of importance for the development ofdelinquency.
In this list, Farrington shows that impulsiveness is one of the mostimportant individual factors that predict offending. And we see most of the
symptoms related to ADHD. In some longitudinal research there has been
some focus on ADHD, because it is of importance for the development ofdelinquency.
 Means or ratings of lack of impulse control
Means or ratings of lack of impulse control
 It is important in this perspective to see the development from the firstpersonal disorders to a negative career and later, to incarceration. This
can be conceptualised as an interaction of personal and social inadequate
behaviour and the social reactions on it. Missing social support,inadequate help (systems), difficult familial and social situation and, in the
further development, the forms of punishment by court, can increase theprocess.
The problem is to find an adequate conceptualisation and description of
this process, because most factors are just risk factors, that means, theyincrease the risk that delinquency occurs, but they do not determine this
development. So we find different models to describe the pathways.
In this model, the focus is on ongoing activity or disorder. This means of
It is important in this perspective to see the development from the firstpersonal disorders to a negative career and later, to incarceration. This
can be conceptualised as an interaction of personal and social inadequate
behaviour and the social reactions on it. Missing social support,inadequate help (systems), difficult familial and social situation and, in the
further development, the forms of punishment by court, can increase theprocess.
The problem is to find an adequate conceptualisation and description of
this process, because most factors are just risk factors, that means, theyincrease the risk that delinquency occurs, but they do not determine this
development. So we find different models to describe the pathways.
In this model, the focus is on ongoing activity or disorder. This means of
 In this model Bronder, shown at the ADHD meeting in HØnefoss in 2003,
the development of the disorders and the possible interaction with other
disorders (which can occur, but must not) is better conceptualised.
Another way of describing the development is described by Hampel and
In this model Bronder, shown at the ADHD meeting in HØnefoss in 2003,
the development of the disorders and the possible interaction with other
disorders (which can occur, but must not) is better conceptualised.
Another way of describing the development is described by Hampel and

 In this model, the focus is more on co-morbidity. Than means, there canbe some changes in the symptoms over the life-course, being dominant in
different stages of development in the life-course.
Maybe, this model explains better why we rarely find a clear symptomatic
of ADHD in later life (in inmates in the prisons). Due to this model, thereare these changes in symptoms. So the basic ‘cause’ of the difficult
behaviour of the inmate has been once ADHD, but know it shows itself as
In the last 20 years there has been the discussion that ADHD does notend with adulthood. Now, in the German discussion it is said that about
50% of young adults show some further symptoms, that means with
impairments of daily activities. And, if we take the last model intoaccount, it will not be easy to diagnose them.
So we have different pathways of the role of ADHD in the life-course.
In this model, the focus is more on co-morbidity. Than means, there canbe some changes in the symptoms over the life-course, being dominant in
different stages of development in the life-course.
Maybe, this model explains better why we rarely find a clear symptomatic
of ADHD in later life (in inmates in the prisons). Due to this model, thereare these changes in symptoms. So the basic ‘cause’ of the difficult
behaviour of the inmate has been once ADHD, but know it shows itself as
In the last 20 years there has been the discussion that ADHD does notend with adulthood. Now, in the German discussion it is said that about
50% of young adults show some further symptoms, that means with
impairments of daily activities. And, if we take the last model intoaccount, it will not be easy to diagnose them.
So we have different pathways of the role of ADHD in the life-course.
 But there are also some difficulties in diagnosis ADHD in adult persons:
Criteria of anamnesis for adults:
But there are also some difficulties in diagnosis ADHD in adult persons:
Criteria of anamnesis for adults:
 discussion is in progress, so we do not have a good diagnostic procedureor an adequate therapy.
And we do not know much about the topic of self-medication with drugs
done by the ADHD persons. But this seems to be a real phenomena.
So their is a high risk for drug abuse for ADHD patients without treatment.
discussion is in progress, so we do not have a good diagnostic procedureor an adequate therapy.
And we do not know much about the topic of self-medication with drugs
done by the ADHD persons. But this seems to be a real phenomena.
So their is a high risk for drug abuse for ADHD patients without treatment.
 work, with friends; also important is a good integration into theworkplace, but also school qualification, motivation to learn, vocational
Only when we take into account this interaction between risk factors and
protective factors we are able to understand, why even in case ofcomparable bad living situations and risk factors only a part of these
Studies suggest that new social bonds or changing live conditions or
situations can generate turning points in the life-course. They can do so,but the must not do it. This depends heavily on the quality of these
changes, that would mean, only a good marriage or a good job will
change life, but also some changes of the self-conception, of somechanges in viewing oneself, changes in values are necessary (Maruna
There has to be some self-reform, initiated by themselves, by others, by
new experiences in school work or partnership. For persons with ADHD itmay be important to find the diagnosis, to get help in coping with the
symptoms, to get special training so that they will be enabled to have andto experience success. This is to start motivation to change the life course,
to start to get straight. This can and will be a very long process,
depending on how long the person has been involved in his deviant lifestyle, his criminal career, his history of disorder. Giving this new
experiences is an utmost important task to fulfil. The results, the changeof life-course, will not be seen at once, but mostly in later times. But small
work, with friends; also important is a good integration into theworkplace, but also school qualification, motivation to learn, vocational
Only when we take into account this interaction between risk factors and
protective factors we are able to understand, why even in case ofcomparable bad living situations and risk factors only a part of these
Studies suggest that new social bonds or changing live conditions or
situations can generate turning points in the life-course. They can do so,but the must not do it. This depends heavily on the quality of these
changes, that would mean, only a good marriage or a good job will
change life, but also some changes of the self-conception, of somechanges in viewing oneself, changes in values are necessary (Maruna
There has to be some self-reform, initiated by themselves, by others, by
new experiences in school work or partnership. For persons with ADHD itmay be important to find the diagnosis, to get help in coping with the
symptoms, to get special training so that they will be enabled to have andto experience success. This is to start motivation to change the life course,
to start to get straight. This can and will be a very long process,
depending on how long the person has been involved in his deviant lifestyle, his criminal career, his history of disorder. Giving this new
experiences is an utmost important task to fulfil. The results, the changeof life-course, will not be seen at once, but mostly in later times. But small

 So when the young persons come into prison, mostly they will have manyproblems:
Problems of inmates:
So when the young persons come into prison, mostly they will have manyproblems:
Problems of inmates: 
 Literature:
Literature:
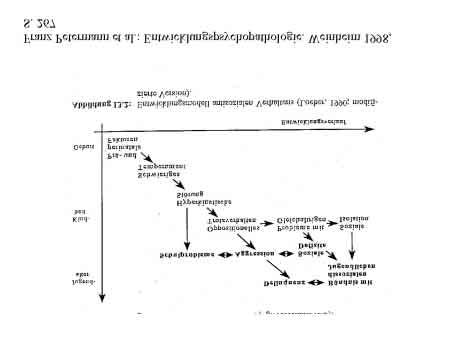 In this model, Petermann et al. start from birth, going on with possible
problems, until it leads in young adulthood in delinquency. But one has toremind, that every step can have another way out, taking into account
possible protective factors. And it also shows that it is a long developmentwith many steps in between, until the stage of (a life-long persistent)
In this model, Petermann et al. start from birth, going on with possible
problems, until it leads in young adulthood in delinquency. But one has toremind, that every step can have another way out, taking into account
possible protective factors. And it also shows that it is a long developmentwith many steps in between, until the stage of (a life-long persistent)