Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
Microsoft word - reich_frost_access_tdr-6.8.10.docx
Research Studies for Promoting Access to Health Technologies in Poor Countries* By Michael R. Reich and Laura J. Frost
Many people in developing countries lack access to health technologies, even basic ones. These technologies include life-saving medicines, such as antiretrovirals for HIV/AIDS, as well as life-enhancing medicines, such as medications that help stop asthma attacks and improve breathing. Limited access is also a problem with many other health products such as vaccines that can prevent debilitating diseases, diagnostics for infectious and chronic diseases, preventive technologies such as insecticide-treated bednets, and various kinds of contraceptives. In 1999 the World Health Organization (WHO) estimated that since the mid-1980s, around 1.7 billion people—approximately one third of the world’s population in 1999—did not have regular access to essential medicines and vaccines. The WHO’s estimate was based on a questionnaire survey of national experts in pharmaceutical policy (reflecting the difficulties of collecting accurate population-level data on this question) (WHO 1988; WHO 2004).1 In recent years, the issue of access to medicines and other health technologies has risen on the global policy agenda. The most contentious debates about inadequate access in poor countries have focused on drugs and vaccines, but similar problems exist for other health technologies. Access to diagnostics, for example, has been relatively unexplored in policy debates. And the focus on certain types of access barriers (especially pricing and patents) has tended to obscure other important obstacles to access such as distribution, delivery, and adoption problems. In recent work, we analyzed the histories of six health technologies as the basis for creating a more comprehensive view of access: praziquantel to treat schistosomiasis (a parasitic worm disease), hepatitis B vaccine, the Norplant contraceptive, malaria rapid diagnostic tests, vaccine vial monitors, and the female condom (see Exhibit 1) (Frost and Reich 2008). Four criteria guided our selection of case studies. We chose cases that: (1) include different types of health technologies; (2) reflect a range of health problems; (3) span different phases of access; and (4) include examples that have been successful as well as those that have encountered obstacles and faltered. Our approach in these case studies drew from anthropological research that traces the ‘life-cycles’ or ‘biographies’ of medicines from production to end-user (Van der Geest et al. 1996; Reynolds Whyte et al. 2002; Reynolds Whyte et al. 2006) and from public health case study research on barriers to technology access (Sevene et al. 2005). For each case study, we analyzed the social, economic, political, and cultural processes that shaped access to the health technology in developing countries. We followed the technology’s flow through different phases of access, identified barriers, and looked for measures that create access (Frost and Reich 2008).
* This draft chapter was prepared for the TDR Consultative Meeting on Implementation Research for Access and Delivery of New and Improved Tools, Strategies, and Interventions for the Control of Diseases of Poverty, Kampala, Uganda, 28-30 June 2010. (Draft of 8 June 2010)
Our case study research led to seven major findings with important implications for initiatives to develop global health products. These efforts are seeking to introduce new health products for poor countries (such as the Global Alliance for TB Drug Development, the Foundation for Innovative New Diagnostics, the International AIDS Vaccine Initiative, and OneWorld Health). Once developers demonstrate a product can improve the health of poor people in poor countries, they confront a series of new problems related to creating access. Specific research activities are then essential in promoting the development of access activities. Various models exist for studying access, but there is no guide on how to write an Access Plan, what it should include, and what kind of research should support its development. This paper addresses this gap in the literature. It presents seven lessons about the bottlenecks to access, the strategies that product developers and champions can use to overcome them, and the implications for 13 kinds of research studies that are needed to design an Access Plan. What do we mean by access? Stated simply, access refers to people’s ability to obtain and use good quality health technologies when they are needed. Access is not just a technical issue involving the logistics of transporting a technology from the manufacturer to the end-user. Access also involves social values, economic interests, and political processes. Access requires a product as well as services and depends on how health systems perform in practice. We think of access not as a single event but as a continuous process involving a series of activities and actors over time. Access framework: Our conception of access is based on four A’s: architecture, availability, affordability, and adoption (Exhibit 2). These four A’s are activity streams that occur simultaneously. Our access framework provides more complexity than the conventional view of a linear ‘value chain’ based on, for example, the stages of discovery, development, and delivery (IBM Institute for Business Value 2004). Our approach builds on previous research on barriers to access (Andersen and Andersen 1974; Hanson et al. 2003). It adapts the approach developed by the Global Alliance for TB Drug Development called the AAA strategy (Global Alliance for TB Drug Development 2009). We have changed some terms and added some ideas to improve both the clarity and comprehensiveness of the analysis. Our framework explicitly recognizes the organizational dimension of access, or architecture. This activity stream involves decisions about organizational structure that are required for coordinating the other three activity streams to produce access. The second stream concerns the availability of health technologies. This includes the activities of manufacturing, forecasting, procurement, distribution, and delivery to ensure a reliable and regular supply of the technology. The third stream concerns the affordability of technologies for developing-country governments, non-governmental agencies, and individual end-users. This includes activities ensuring that health technologies and related services are not too costly for the people who need them. The final stream involves the adoption of health technologies.
This involves activities at the global, national, district, and community levels to ensure acceptance of the health technology, with a focus on generating demand. Access activities: Our framework uses a comprehensive approach to access and maps activities from the global level to the end-user. The framework breaks down the process into access activities, which are defined by specific events and which must occur for access to achieve its potential health benefits. In the framework, we view access as beginning in the product development stage and concluding when end-users (including both providers and patients) are using the technology appropriately. Importantly, we have extended our view of access beyond simply reaching the end-user because we recognize that how people use the technology plays a major role in the ultimate effects produced. Thus, our concept of access includes ideas about both appropriate and inappropriate use of technology. Findings for Product Development Partnerships Getting the four activity streams right can produce successful access for health technologies. But doing so is not easy. Based on the case histories, we reached the following findings about the process of creating access and the role of 13 applied research studies that are needed to design an Access Plan (see Exhibit 3). Finding 1: Developing a safe and effective technology is necessary but not sufficient for ensuring technology access and health improvement.Showing that a new technology is safe and efficacious in clinical trials represents an exciting and important result. Working through the regulatory process to license the new technology also constitutes significant progress. But these measures should not be viewed as endpoints; they are only midway successes in a complicated process of creating access. The case of the contraceptive implant Norplant nicely illustrates this point. Norplant was developed by the non-profit Population Council in New York City. Clinical trials demonstrated a high level of safety and efficacy, and by the end of 1996, more than five million implants had been distributed worldwide (about 3.6 million in Indonesia and close to a million in the United States) (Harrison and Rosenfield 1998). But Norplant’s use in the field faced many hurdles. Major access barriers arose in many countries related to affordability, the training and competence of providers, the health infrastructure’s capability to deliver high-quality services (including the capacity to remove the implant), adoption of new technologies by end-users, and the effects of media and litigation on product reputation. These problems led to the withdrawal of Norplant in the United States in 2002. This finding challenges the view held by some product developers that ‘if we make a good product that addresses an important health problem in developing countries, it will be used.’ The product needs to be managed throughout the access process to address the numerous obstacles along the pathway to the end-user. Products do not fly off the shelf on their own—especially technologies aimed at improving health conditions in poor
countries, because these products do not fit a conventional market-driven model. Many problems exist between the processes of technology innovation and actual diffusion and appropriate use in developing countries (Juma et al. 2001). Some technology developers do not know or understand the markets in developing countries, do not have existing organizational bases in those markets, and do not know how to enter those markets. For example, Temptime Corporation, the developer of vaccine vial monitors (VVMs), had not previously worked in global health and needed help from the Program for Appropriate Technology in Health (PATH) in entering this market, negotiating with international agencies, and redesigning its product for end-users. On the other side, developing-country governments often lack the financial capacity to purchase new technologies, but they also lack adequate purchasing mechanisms to push down prices for innovative products or to assure good quality. For these and other reasons, creating access for good health technologies requires concerted efforts. Two research methods—Problem Statement Analysis and a Target Product Profile— provide the foundation for initiating innovative product development and access planning. An Access Plan begins with Problem Statement research (Research Study 1) that demonstrates a public health need for a product (including epidemiological data) and an assessment of problems in developing effective products (scientific problems as well as market problems). This research should include an assessment of potential access barriers posed by government, market, and NGO failures. It should also involve an evaluation of whether the product has commercial market potential and if so, in which markets and under what conditions. In addition, the Problem Statement research should include an assessment of the basic characteristics of the product under development, often presented as the Target Product Profile (Research Study 2). These characteristics can include health impact, indications and usage, target population, mechanism, route of administration, dosage schedule, efficacy, safety, clinical pharmacology, price, product presentation, and storage. The Target Product Profile guides the product development process, as a living document that is updated regularly, and provides core data needed for access planning. Finding 2: Creating access depends on effective product advocacy by a product champion to construct and manage the architecture of access. Product champions in global health are people or organizations that believe in new technologies and are committed to developing products with wide access in poor countries. Product champions also take a major role in constructing and managing the architecture of access, especially the relationships among different organizations. Champions are found in many types of organizations working in global health (including technical agencies, nonprofit organizations, academic institutions, and manufacturers). In the case of VVMs, staff from PATH collaborated closely with WHO staff to ensure the introduction and scale-up of the technology on all Expanded Program on Immunization (EPI) vaccines. For Norplant, Population Council staff developed the product, introduced it, and acted as product champion for this new contraceptive delivery system. The main product champion for the female condom has been the manufacturer, the Female Health Company, and its foundation. Funding is key to the effectiveness of product champions. The product
champion’s role can range from stimulating awareness of the technology among specific groups to more strategic activities of overcoming difficult development or access barriers. One example of an effective product champion is the work of PATH in guiding the development of VVMs. The VVM is a miniature time-temperature indicator printed onto the label of a vaccine vial during the labeling process of vaccine production that aims to reduce vaccine wastage. At a critical point during product development in 1989, when Temptime had decided to give up on the project after months of failing to achieve technical success, representatives from PATH visited the company, explained the global significance of VVMs, and convinced Temptime to continue its work (without additional funding) (PATH 2005). PATH staff members continued to guide the access process for VVMs and provided crucial support to WHO staff through mentoring, technical assistance, and project documentation. By the end of 2005, close to 100 per cent of WHO-prequalified vaccine producers used the technology on their vaccine labels. Major challenges, however, still remain in expanding VVM access in the Pan American Health Organization (PAHO) region and in developing-country vaccine markets (Frost and Reich 2008, p. 158). Effective product advocacy depends on an access plan that frames the work activities of champions and partners and takes into account the perspectives of different actors. Product champions and their partners need to develop an access plan (sometimes with the assistance of external consultants) to assess potential barriers and opportunities at the global and national levels and identify strategies to navigate and shape the complex terrain of access. In constructing relationships among different groups and individuals, advocates work with actors who may have widely divergent views of new health technologies. In the case of VVMs, WHO staff and health workers viewed the technology as key to improving the cold chain (the process of keeping a vaccine at a safely cold temperature throughout production and transportation) and decreasing vaccine wastage. For the UNICEF Supply Division, VVMs challenged the UNICEF policy on sole suppliers and created stress in relationships with vaccine producers. For vaccine producers, attaching VVMs to their vaccines sold to UNICEF meant a number of legal, logistical, and commercial challenges to their business. Providing VVMs required a concerted effort—and a significant amount of time—to bring these diverse groups together and address their different perspectives on the technology. Product champions and their partners can use an access plan to frame their activities, map the position and power of these diverse actors, identify obstacles and opportunities, and prepare concrete strategies that promote access. The access plan allows champions to reshape their analysis and strategies as unexpected circumstances arise and the broader context evolves. The female condom case shows what can happen when there is no access plan. In the product introduction phase, individuals and organizations promoting the female condom identified next steps for access in global meetings. However, the steps were not prioritized or written into a plan; as a result, the next steps were never systematically implemented. This meant that advocates had no clear guide for moving access efforts forward.
One research tool that can help construct and manage the access architecture is Partnership Analysis (Research Study 3). This type of analysis can address the problem of how to organize the diverse partners involved in creating access. Partnership Analysis evaluates different potential partners, their roles, and potential structures to coordinate the partners. Managing the architecture often requires aligning the different interests and values of key stakeholders. One effective tool for conducting a stakeholder analysis and political strategies to manage partners is the software program for Political Analysis, known as PolicyMaker (Research Study 4) (Reich and Cooper 2009). Finding 3: Product champions need to create expert consensus about their health technology in international technical agencies and global health policy communities. Our case studies highlight the importance of creating ‘expert consensus’ on a new technology, within both the international health technical agencies and the broader international public health community. This role for expert consensus is emphasized by other public health analysts (Levine 2004). Product champions need to design strategies for producing expert consensus as one of their first tasks. The key question is: Whose consensus needs to be gained at the global level? The answer differs by technology because the specific actors vary. But for most technologies, approval by the relevant international technical agency is required to move forward on other areas of adoption for the product. Agencies signal their adoption with official decisions about the technology and the related disease or health condition. This approval process often occurs through WHO expert groups, which can challenge or confirm the conventional wisdom.
One good example of expert consensus is the resolution adopted at the World Health Assembly in May 2001 on treatment for schistosomiasis and soil-transmitted helminths (intestinal worms that include ascaris and hookworm). This official statement helped promote new efforts to make praziquantel (the drug to treat schistosomiasis) more widely available in Africa (WHO 2001). In the case of Norplant, the WHO conducted a technical evaluation and stated that the contraceptive was ‘particularly advantageous to women who wish an extended period of contraceptive protection’ (WHO 1985). These official announcements by an international agency, however, are not simply the result of technical consultations and decisions. They often depend on highly political negotiations among actors with different interests in the technology. Product champions would be helped in these tasks by conducting a stakeholder analysis of the key players involved and designing explicit political strategies for managing the stakeholders and the process of producing expert consensus to support their technology, as part of the Political Analysis in Research Study 4 (Reich 2002). Product champions can use the results from the Problem Statement Analysis (Research Study 1) and Target Product Profile (Research Study 2) in identifying strategies to mobilize support from both international agencies and technical experts. Finding 4: End-user adoption of a technology is an essential but often overlooked component of the entire process of creating access. Adoption of a technology by the end-user is vital to ensuring access—whether the end-user is a patient, a consumer, or a
provider. Adoption by end-users is influenced by the characteristics of the technology and the health problem it addresses, and by the social, political, and historical contexts. The female condom demonstrates how a technology’s characteristics can make adoption difficult for end-users in some contexts. Some women, for example, consider the female condom to be extremely large and bulky, aesthetically unappealing, prone to slippage and twisting during sexual intercourse, and stiff in its internal rings (AIDSCAP 1997). Developers of the first generation of female condoms did not adequately take into account the perspective of end-users. These negative impressions can be addressed and the chances of long-term use can be increased through extended and supportive counseling by providers (Telles Dias et al. 2006). Some women, however, do not have access to counseling while others are unwilling to endure a series of awkward ‘practice sessions’ in order to get the female condom ‘right.’ Sales of the female condom have remained low since its introduction in the early 1990s. By 2004, approximately 12.2 million units were sold per year, representing only 0.1-0.2 per cent of the number of male condoms sold worldwide (The Female Health Company 2005). New female condom designs in development are seeking to address the adoption issues of end-users by changing these negative technology characteristics, making female condoms more user- friendly, and using less expensive material to make the technology more affordable. Our cases show that paying attention to adoption by end-users must begin early in the life of a new technology. This attention starts during product development when technical characteristics of a new technology are first under consideration. It continues in field trials and pilot projects, when end-user views of a new technology can be assessed and addressed through technical changes. Attention to end-users is also important in later phases, when managing the perceptions of the technology is central to creating access. These efforts require an understanding of end-user preferences and concerns and the context in which they interpret new technologies. Research studies are essential in helping product developers understand problems from the perspective of end-users. This research can include market surveys and focus groups, as part of Product Acceptability Studies (Research Study 5). The information gathered in these studies is particularly important in designing products that meet the needs and wishes of the target population (including both end-users and providers). Communications and Branding Studies (Research Study 6) are also important for tailoring messages and brands targeted to end-users and providers. These studies provide the basis for the development of social marketing campaigns to promote adoption of the technology. Finding 5: The cost of health technologies and related services is a key barrier to access; strategies to expand access must address affordability. The literature on access highlights cost to governments and individuals as a major obstacle, and our findings support this. Decreasing product costs for governments can involve a range of strategies. For example, in seeking to lower the price of praziquantel, the Schistosomiasis Control Initiative (SCI) has used a bulk purchasing approach and has sought to expand competition by assisting manufacturers with registration and stimulating local
formulation in Africa. By increasing the number of registered suppliers in Burkina Faso, for example, the SCI helped to create a more competitive bidding process for government purchases, reducing the price per tablet for praziquantel from US $0.14 to $0.09 (Frost and Reich 2008). Other strategies to address government affordability are tiered pricing (used by the Population Council for Norplant) and threats of compulsory licensing (used by Brazil for antiretroviral products for HIV/AIDS) (Reich and Bery 2005). Another measure to address high costs is external funding for government procurement. For example, the Bill & Melinda Gates Foundation supports SCI to finance praziquantel purchases for the six African countries it works with. The biggest problem with the external financing approach concerns its sustainability over the medium and long term, because donors persistently seek to limit the timeframe of their funding commitments. Although affordability is essential, our cases show that making a technology more affordable is rarely sufficient on its own to create access for the product. Availability constraints as well as factors related to adoption and architecture all need to be considered and addressed. Research on several topics is important to address affordability barriers. One topic is product cost. Cost Analysis (Research Study 7) can be undertaken to study the different costs involved in manufacturing, distribution, social marketing, and other components of access. A second topic is end-users’ willingness to pay for products. Willingness-to-Pay Analysis (Research Study 8) assesses the capacity and willingness of end-users to use their own money (out-of-pocket) to purchase the product. (It is worth noting, however, that what people say they are willing to pay doesn’t always translate into reality, particularly for new products.) The third topic is financing. Financial Sources Analysis (Research Study 9) studies the different potential donors who could provide funding to assure access for the product and related services. Finding 6: Supply-side strategies that ensure the availability of a technology are needed to help expand access for health technologies in developing countries. Two supply-side strategies to assure availability are of particular importance. The first relates to information failures. Suppliers often lack good or complete information about product demand in developing countries. These information problems affect supply, since manufacturers may underestimate the potential market in a poor country or region and may not take the necessary steps to enter the market (such as registering the product with the government). Strategies to address these problems include disseminating information to manufacturers about demand and assisting companies in product registration. A Global Health Forecasting Working Group, convened by the Washington-based Center for Global Development in 2006, provides recommendations to the global health community for improving demand forecasting. The proposals include the establishment of an ‘infomediary’ that would allow product demand to be mobilized and information shared among manufacturers and global health partners in a coordinated way (Center for Global Development 2007). Another information barrier is that government procurement agencies in poor countries often have incomplete information about the availability and quality of products and
suppliers for a particular health technology. For example, although many government procurement agencies have financing from the Global Fund to Fight AIDS, TB and Malaria to procure malaria rapid diagnostic tests, they confront a rapidly changing range of available products and suppliers, making the purchase of diagnostics extremely difficult. One simple strategy that the WHO has used to address this problem is to give countries regularly updated information about rapid diagnostic products and suppliers on its Website (http://www.wpro.who.int/rdt) and in a ‘Sources and Prices’ document for malaria products (WHO et al. 2004). Reducing information asymmetries, by regularly disseminating updated information to producers and potential purchasers, can contribute to increased availability. A second important supply-side strategy relates to the difficulty of finding commercial partners willing to develop or manufacture a technology for use in poor countries. Such challenges are a major access barrier particularly for lower profit technologies (relative to, for instance, drugs and vaccines for sale in rich countries). Our study found that suitable private partners for low-profit technologies may be located among small to midsize companies that have existing commercial products, are already generating revenues from these products, and have experience in working with regulatory authorities (such as the U.S. Food and Drug Administration). This finding concurs with a 2005 study on neglected disease drug development that urged policymakers to target commercial incentives for research and development to smaller companies that have a good chance of becoming engaged with neglected disease markets (Moran 2005). One example of a technology that was produced by a small to midsize company is the case of a rapid diagnostic test for malaria. In this instance, when the Walter Reed Army Institute (WRAI) looked for a commercial partner to manufacture its malaria diagnostic, it encountered many barriers that set back its timeline significantly. Because the diagnostic would be used for U.S. soldiers, WRAI needed a company that could take the product through the FDA regulatory process. After years of seeking a partner, WRAI found one in Binax Inc.—a midsize company. In this search, WRAI learned that most diagnostic companies are small ‘mom-and-pop’ businesses that do not possess the resources, know-how, experience, or willingness to navigate the FDA process. It also discovered that the large companies with these features were not interested in partnering because the technologies were not profitable enough for them. Product developers and champions therefore need to expand their search for partners to small and midsize companies willing to take on niche products and also high-quality manufacturing firms in emerging markets (such as China and India). The challenges of finding good partners in emerging markets should not be underestimated, especially given the problematic regulatory environments in those countries (Yardley and Barboza 2008). It is worth noting, however, that a number of groups have found good manufacturing partners in these countries, as shown by the success of the SCI in working with praziquantel producers in both China and India. Several research studies can provide the empirical basis for market forecasting and can help identify the most promising partners for manufacturing and market introduction. Market Forecasting (Research Study 10) is needed to estimate the potential market, as
part of efforts to persuade manufacturers to produce the product. Regulatory Analysis (Research Study 11) identifies national procedures and standards, as well as the requirements of international agencies, to assure registration and financing support and to meet quality standards. Production Analysis (Research Study 12) assesses quality and cost issues in manufacturing, and the efficiency and safety of production processes. Finding 7: Limited health infrastructure in many developing countries impedes technology access, making it important to invest in health system strengthening to ensure sustained access. The successful delivery of technologies to patients and consumers depends in large part on the capacity of the health sector’s human resources, network of public and private providers, and availability of functioning equipment—in short, how the health system performs on a daily basis (Roberts et al. 2004). Different technologies, however, may depend on improving the performance of different aspects of the health system. Health system strengthening is especially important for new technologies (because many require the development of new systems and skills) and provider-dependent technologies. But it is also necessary for products designed for use in areas with limited health infrastructure—such as poor countries. The Norplant case study demonstrates how the failure to invest in health systems can impede access. Norplant, as a new contraceptive implant technology, required both insertion and removal by a trained provider. In the rapid scale-up of Norplant in countries such as Indonesia and the United States, many providers received training (particularly on insertion techniques), but the instruction was not deep or comprehensive enough. As a result, many health professionals were not well trained on removal techniques, and these training shortfalls led to later difficulties with implant removals. Other health system problems that emerged globally with Norplant included the lack of sufficient information and counseling about the method for end-users and concerns about informed choice, particularly whether uneducated, poor women were targeted for Norplant or steered to that method over other contraceptives. Overall, our study shows that strategies for health system strengthening are product- and context-specific, but they all require sufficient funding, attention, and time to adequately address health system barriers if access is to be produced and sustained. Research studies on Health Systems Analysis (Research Study 13) can help identify health system functions that are needed to assure that effective access is produced for specific health technologies. The diagnostic process in the book Getting Health Reform Right (Roberts et al. 2004) provides one method for assessing health system barriers and designing interventions to assure access. Concluding Remarks
Access to health technologies in poor countries is hindered by multiple obstacles. Inadequate access is rarely a single-failure problem. Access problems typically result from a combination of market failures, government failures, and NGO failures. The problems often affect all four dimensions of access—architecture, availability,
affordability, and adoption—although the patterns differ by specific technology. Addressing the multiple failures requires many steps directed at global-, national-, and local-level actors and depends on various kinds of expertise. Creating access requires that individuals and organizations devote time, passion, and resources to a new technology and carefully craft strategies for addressing the multiple barriers along the pathways to access. Specific research activities are an essential part of planning for access, and provide the foundation for an Access Plan. Product developers and champions without prior field experience may not fully appreciate the kinds of research that are necessary to develop an Access Plan and update it throughout the stages of product development, launch, and scale-up. Organizations with existing products and prior market experience may have the expertise and capacity to undertake these research studies, but even they are not always successful at assuring access to new products. Product development partnerships are now grappling with the complexity of developing a strong evidence base for creating access for the products they are developing. The specific research studies presented in this chapter can help advance the process of designing an Access Plan and help assure that safe and effective health technologies reach the hands of people in poor countries who need them most. Other chapters in this book provide additional lessons on the kinds of strategies and policies that will promote widespread access for their products in low-and middle-income countries.
The WHO survey in 1999 asked national experts ‘to estimate the percentage of the population who have access to a minimum list of 20 essential medicines, which are continuously available and affordable at a health facility or medicines outlet, within one hour’s walk from the patients’ home.’ For more information, see http://www.who.int/medicinedocs/en/d/Js6160e/9.html
ACKNOWLEDGMENTS This chapter is adapted from Chapter 9 of L.J. Frost and M.R. Reich, Access: How do good health technologies get to poor people in poor countries? (Harvard University Press, 2008). The research for that book was supported by the Bill & Melinda Gates Foundation. The authors thank Miguel Ángel González Block for his helpful comments on an earlier draft of the chapter. BIBLIOGRAPHY
AIDSCAP Women’s Initiative. (1997) The Female Condom: From Research to the Marketplace, Arlington, VA: Family Health International/AIDSCAP. Andersen, L.A. and Andersen, R. (1974) ‘A framework for the study of access to medical care”, Health Services Research, 9: 208–20. Center for Global Development Global Health Forecasting Working Group (2007) A Risky Business: Saving Money and Improving Better Demand Forecasts, Washington, DC: Center for Global Development. The Female Health Company (2005) No More Excuses: The Female Health Company 2005 Annual Report,Chicago: The Female Health Company. Frost, L.J. and Reich, M.R. (2008) Access: How Do Good Health Technologies Get to Poor People in Poor Countries? Cambridge, MA: Harvard Center for Population and Development Studies, distributed by Harvard University Press. Global Alliance for TB Drug Development. (2009) Our AAA Strategy. Published on the Internet, available at http://www.tballiance.org/aaa/mandate.php (accessed Sept 19, 2009). Hanson, K., Ranson, M.K., Oliveira-Cruz, V. and Mills, A. (2003) ‘Expanding access to priority health interventions: a framework for understanding the constraints to scaling- up’, Journal of International Development, 15: 1–14. Harrison, P.E. and Rosenfield, A. (eds) (1998) Contraceptive Research, Introduction, and Use: Lessons from Norplant, New York: National Academy Press. IBM Institute for Business Value. (2004) Pharma 2010: Silicon Reality, Somers, NY: IBM Global services. Published on the Internet, available at http://www- 935.ibm.com/services/us/index.wss/ibvstudy/imc/a1002316?cntxtId=a1000060(accessed 28 April 2009).
Juma, C., Fang, K., Horca, D. et al. (2001) ‘Global governance of technology: meeting the needs of developing countries,” International Journal of Technology Management, 22: 629–655. Levine, R. (2004) Millions Saved: Proven Successes in Global Health, Washington: Center for Global Development. Moran, M. (2005) ‘A breakthrough in R&D for neglected diseases: new ways to get the drugs we need’, PLoS Medicine, 2: e302. PATH (2005) HealthTech Historical Profile: Vaccine Vial Monitors, Seattle: PATH. Reich, M.R. (2002) ‘The Politics of Reforming Health Policies’, Promotion & Education, 9: 138-42. Reich, M.R. and Bery, P. (2005) ‘Expanding global access to ARVs: the challenges of prices and patents.’ In K.H. Mayer and H.F. Pizer, eds, The AIDS Pandemic: Impact on Science and Society, San Diego, CA: Elsevier Academic Press. Reich, M.R. and Cooper, D.M. (2009) PolicyMaker 4.0. Brookline, MA: PoliMap.
Reynolds Whyte, S., Van der Geest, S. and Hardon, A. (2002) Social Lives of Medicines, Cambridge: Cambridge University Press. Reynolds Whyte, S., Whyte, M.A., Meinert, L. and Kyaddondo, B. (2006). ‘Treating AIDS: dilemmas of unequal access in Uganda.’ In A. Petryna, A. Lakoff and A. Kleinman, eds, Global Pharmaceuticals: Ethics, Markets, Practices, Durham: Duke University Press, 240–62.
Roberts, M.J., Hsiao, W.C., Berman, P. and Reich, M.R. (2004) Getting Health Reform Right: A Guide to Improving Performance and Equity, New York: Oxford University Press. Sevene, E., Lewin, S., Mariano, A. et al. (2005) ‘System and market failures: the unavailability of magnesium sulphate for the treatment of eclampsia and pre-eclampsia in Mozambique and Zimbabwe’, BMJ, 331: 765–69. Telles Dias, P.R., Souto, K. and Page-Shafer, K. (2006) ‘Long-term female condom use among vulnerable populations in Brazil’, AIDS Behavior, 10: S67–75. Van der Geest, S., Reynolds Whyte, S. and Hardon, A. (1996) ‘The anthropology of pharmaceuticals: a biographical approach’, Annual Review of Anthropology,25: 153–79. WHO, Special Programme of Research, Development and Research Training in Human Reproduction (1985) ‘Facts about an implantable contraceptive [memorandum from a WHO Meeting]’, Bulletin of the World Health Organization, 63: 485–94.
WHO (1988) The World Drug Situation, Geneva: WHO. WHO (22 May 2001, Fifty-fourth World Health Assembly Resolution WHA54.19) Schistosomiasis and Soil-Transmitted Helminths, Geneva: WHO. Published on the Internet, available at http://ftp.who.int/gb/archive/pdf_files/WHA54/ea54r19.pdf (accessed Mar 10, 2009). WHO (2004) The World Medicines Situation, Geneva: WHO WHO, UNICEF, PSI and MS (2004) Sources and Prices of Selected Products for the Prevention, Diagnosis and Treatment of Malaria, Geneva: WHO. Published on the Internet, available at http://www.who.int/medicines/areas/access/AntiMalariaSourcesPricesEnglish.pdf (accessed Feb 5, 2007).
Yardley, J. and Barboza, D. (Sept 27, 2008) ‘Despite warnings, China’s regulators failed to stop tainted milk’, The New York Times, A1.
Exhibit 1: Access story summaries
Access to a medicine: Praziquantel Praziquantel is the drug of choice for treatment of schistosomiasis, an infectious disease caused by parasitic worms (schistosomes) that live in the blood vessels of the human host. Praziquantel became generally available on the international market in the 1980s but access was limited during the 1980s and 1990s in most schistosomiasis-endemic countries. The key barrier was the drug’s affordability. The Schistosomiasis Control Initiative (SCI) was established in 2002 with $27.8 million funding from the Bill & Melinda Gates Foundation. SCI significantly increased access to praziquantel in Africa through a series of strategies related to procurement, collaboration, information, registration, local formulation, and donation. From 2003 to June 2008,SCI delivered a total of 40.29 million treatments in six countries in Africa, to about 19.28 million individuals. While this accomplishment represents a significant success for SCI, the effort has reached only about 10 per cent of the population estimated to be infected with schistosomiasis and needing treatment with praziquantel. Future access to praziquantel will depend on many factors, including the evolving market for the product, the actions of key players, the availability of international aid funding, and the perceptions of national ministries of health regarding both the disease and its treatment. Access to a vaccine: Hepatitis B vaccine Hepatitis B is a serious liver infection caused by the hepatitis B virus. The first hepatitis B vaccine became available in 1981, making it possible to prevent hepatitis B virus infection. Introduction in developing countries in the 1980s and 1990s was slow and limited due to problems in affordability (high product price) and product adoption (safety concerns about plasma vaccines and a limited understanding about the hepatitis B burden). By 1995, only 35 of 90 countries with prevalence rates greater than or equal to eight per cent had begun hepatitis B vaccination programs. Key groups in the architecture of hepatitis B vaccines—including WHO, the International Task Force on Hepatitis B Immunization, and later the GAVI Alliance—then undertook a series of actions to solve access barriers. Their strategies included fostering competition, showing companies that a market existed in developing countries, forecasting demand across countries, and financing the procurement of hepatitis B vaccine for developing countries. The combined efforts led to a change in the global architecture for hepatitis B vaccine access, resulting in dramatic increases in access to the vaccine in the 2000s. As of June 2004, 82 per cent of the GAVI Fund-eligible countries with adequate delivery systems had introduced the vaccine into their routine systems (61 countries). Current challenges are addressing low coverage levels in many countries and ensuring continued access to the vaccine in the future. Access to a diagnostic: Malaria rapid diagnostic tests An estimated 40 per cent of the world population today is at risk of malaria infection. A major challenge for malaria treatment is the prompt and correct diagnosis of malaria infection. Rapid diagnostic tests for malaria (RDTs)—antigen-detecting tests based on immunochromatographic methods—offer a new diagnostic alternative for health professionals. The first RDTs became commercially available in the mid-1990s. In the
early 2000s, the use of RDTs increased rapidly (fueled by increased funding through the Global Fund to Fight AIDS, TB, and Malaria). At the same time, the number of products available rose quickly. WHO estimates that procurement nearly doubled from 2000 to 2004. The number of countries adopting RDT use and budgeting for them in malaria control activities rose from 1 country in 2000 to 32 countries in 2005. In this period of rapid uptake, three challenges associated with RDTs emerged: (1) varying performance of RDT products in field use and study findings, (2) confusing range of products on the market, and (3) limited health worker and patient adoption of malaria diagnostic results. In early 2002, a ‘global focal point’ for malaria RDTs was established at WHO in its Western Pacific Regional Office in Manila. This group used three strategies to address barriers to access for RDTs: policy development, information dissemination, and quality assurance. Whether RDTs influence malaria mortality and morbidity ultimately depends on what happens in the periphery of health systems in poor countries—whether end-users can obtain RDTs and how they use test results in patient management decisions, and on the availability and appropriate use of antimalarial medication. Access to a contraceptive: Norplant The Norplant system is a subdermal form of reversible contraceptive that can prevent pregnancy for up to five years with an efficacy rate of over 99.9 per cent. The implant system consists of six Silastic capsules that are inserted into a woman’s upper arm and release the synthetic progestin levonorgestrel on a continual basis. The Population Council began developing Norplant in the 1960s and negotiated patent and licensing arrangements to make a low-priced product available in the development countries in the early 1980s. Norplant was repeatedly shown to have high safety, efficacy, and effectiveness in clinical trials and postmarketing surveillance but still encountered numerous access problems within developed and developing countries, including (1) affordability, (2) end-user adoption, and (3) provider removal services. The relative importance of these barriers depended on the particular setting. Problems with provider removal services ultimately led to the product’s withdrawal in the United States in 2002. Yet millions of women around the world became Norplant users. By the end of 1992, 24 countries had granted regulatory approval to Norplant; by mid-1997, that number reached 58. As of 2002, an estimated 10.5 million units had been distributed worldwide. Access to a device: Vaccine vial monitors The vaccine vial monitor (VVM) is a miniaturized time-temperature technology that allows health workers to assess vaccine heat damage, and helps to reduce vaccine wastage and assure coverage in hard-to-reach areas. WHO and the Program for Appropriate Technologies in Health (PATH) began the search for a VVM in 1979 and provided critical assistance in product development and market entry to a small firm, Temptime Corporation (based in New Jersey). A suitable product was ready for introduction in 1991. Introduction of the vaccine vial monitor on the oral polio vaccine began in 1996 and five years later, the device was scaled up to all vaccines of the WHO Expanded Program on Immunization. Between 1996 and 2007, Temptime’s sales of VVMs for oral polio vaccine rose more than three-fold to nearly 200 million vials per year and for other EPI vaccines, sales rose from nothing to over 100 million vials per year. By the end of 2005, close to 100 per cent of WHO-prequalified vaccine producers
used the technology. Successful access to VVMs depended crucially on assuring the availability of high-quality products designed for different kinds of vaccines and the adoption and use of VVMs by global vaccine producers. VVM success has occurred for UNICEF-supplied vaccines but not for two other important vaccine markets for developing countries (vaccines provided by PAHO and those sold by developing country domestic manufacturers). Access to a dual protection technology: Female condoms In 2006, an estimated 39.5 million adults were living with HIV infection worldwide, almost half of whom were women. As of mid-2006, the only female-initiated HIV prevention method on the market with proven efficacy in preventing both pregnancy and sexually transmitted infections was the female condom. The FC female condom—designed and produced by the Female Health Foundation—was first introduced in 1992 and has been launched in almost 100 countries worldwide. While the technology generated high levels of initial enthusiasm, adoption by end-users, providers, and national governments has remained low. By 2004, approximately 12.2 million units were sold per year, representing only 0.1-0.2 per cent of the number of male condoms sold worldwide. Access barriers include: (1) limited affordability due to high product price, (2) low end-user adoption due to technical characteristics and the politics of sexual relations, (3) lack of provider adoption due to limited training and support to promote the female condom and problems in availability, (4) insufficient global consensus about the need for the technology and its relationship to other family planning and HIV prevention technologies, and (5) inadequate architecture and access planning. In a renewed effort to increase access to female condoms, product advocates and donors are attempting to increase affordability through the development of new, cheaper products; expand adoption for the technology through training and promotion; and build a new global architecture including strategic planning for access. Note: A full description of each case study can be found in Frost, L.J. and Reich, M.R. (2008) Access: How Do Good Health Technologies Get to Poor People in Poor Countries? Cambridge, MA: Harvard Center for Population & Development Studies.
Exhibit 2: The Access Framework
Champions Partners Access Plan
Source: Frost and Reich, Access, 2008.
Exhibit 3: Research Studies for Creating an Access Plan
1. Problem Analysis. This study demonstrates a public health need for a product (including epidemiological data), and an assessment of problems in developing effective products (scientific problems as well as market problems). This should include an assessment of access barriers posed by government, market, and NGO failures. This assessment should include an evaluation of whether the product has commercial market potential, and if so, in which markets and under what conditions. 2. Target Product Profile. This research describes the basic characteristics of the product under development. These characteristics can include health impact, indications and usage, target population, mechanism, route of administration, dosage schedule, efficacy, safety, clinical pharmacology, price, product presentation and storage. Architecture: 3. Partnership Analysis. This study evaluates different potential partners, their roles, and structures to coordinate the partners. Managing the architecture often requires aligning the different interests and values of key stakeholders. 4. Political Analysis. This study conducts stakeholder analysis and designs political strategies to manage partners and to create expert consensus and setting the policy agenda in the international technical agencies. Adoption: 5. Product Acceptability Studies. The information gathered in these studies is particularly important in designing products that meet the needs and the wishes of the target population (including both end-users and providers). 6. Communications and Branding Studies. These studies are also important for tailoring messages and brands targeted to end-users and providers. Affordability: 7. Cost Analysis, These studies examine the different costs involved in manufacturing, distribution, social marketing, and other components of access. 8. Willingness-to-Pay Analysis. These studies assess the capacity and willingness of end-users to use their own money (out-of-pocket) to purchase the product. 9. Financial Sources Analysis. These studies examine the different potential donors who could provide funding to assure access for the product and related services. Availability: 10. Market Forecasting. This research is needed to estimate the potential market, as part of efforts to persuade manufacturers to produce the product. 11. Regulatory Analysis. This study identifies national procedures and standards, as well as the requirements of international agencies, to assure registration and financial support, and to meet both quality standards. 12. Production Analysis. This study assesses quality and cost issues in manufacturing, and to improve the efficiency and safety of production processes. Health Systems: 13. Health System Analysis. This study identifies health system functions that are needed to assure that effective access is produced for specific health technologies. The diagnostic process in the book Getting Health Reform Right (Roberts et al, Oxford University Press, 2004) provides one method for assessing health system barriers and designing interventions to assure access.
Brief reports 309 Allergic contact dermatitis to topical minoxidil solution: Etiology and treatment Edward S. Friedman, BS, Paul M. Friedman, MD, David E. Cohen, MD MPH, andKen Washenik, MD, PhD New York, New York After more than a decade of use, topical minoxidil solution has proven to be a safe and effective treatmentfor androgenetic alopecia. However, some patients present with c
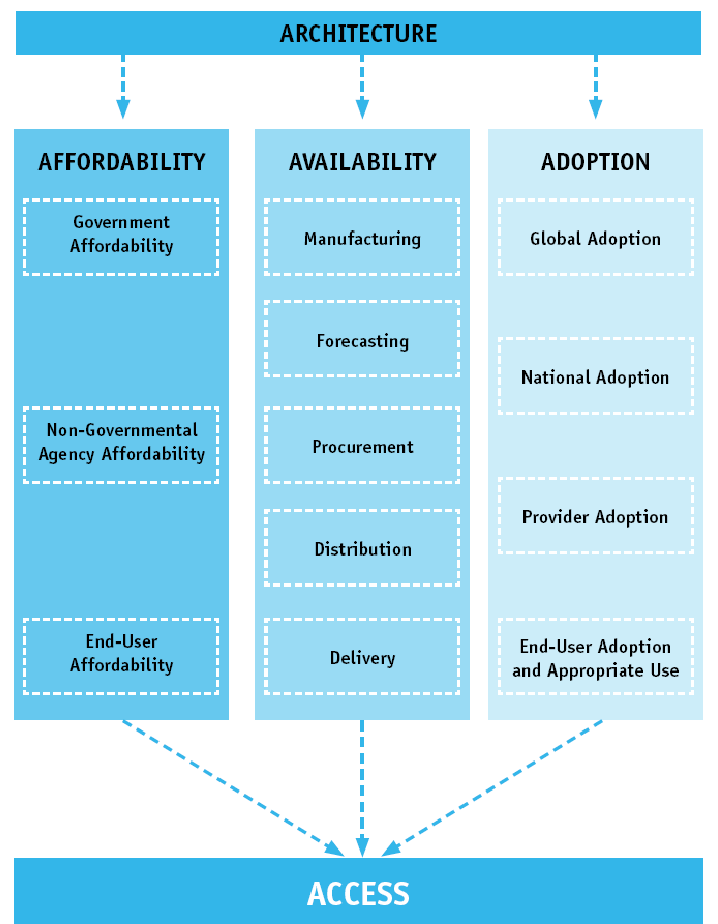
 Exhibit 2: The Access Framework
Exhibit 2: The Access Framework