Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
Untitled
GIUSEPPE G. L. BIONDI-ZOCCAI • GIACOMO MONTI • STEFANO TURI •
IMAD SHEIBAN • ELENA BIGNAMI • GIOVANNI LANDONI
ABSTRACT Introduction. Acute renal failure and fluid retention are common problems in pediatric patients after cardiac surgery. Furosemide, a loop diuretic drug, is frequently administered to increase urinary output. The aim of the present study was to compare efficacy and complications of continuous infusion of furosemide vs bolus injection among pediatric patients Methods. A systematic review and meta-analysis was performed in compliance with The Cochrane Collaboration and the Quality of Reporting of Meta-Analysis (QUORUM) guidelines. The following inclusion criteria were employed for potentially relevant studies: a) random treatment allocation, b) comparison of furosemide bolus vs continuous infusion, c) surgical or intensive care pediatric patients. Non-parallel design randomized trials (e.g. cross-over), duplicate publications and non-human experimental studies were excluded.Results. Up to August 2008, only three studies were found, with 92 patients randomized (50 to continuous infusion and 42 to bolus treatment). Overall analysis showed that continuous infusion and bolus administration were equally effective in achieving the predefined urinary output, and were associated with a similar amount of administered furosemide (WMD=-1.71 mg/kg/day [-5.20; +1.78], p for effect=0.34, p for heterogeneity<0.001, I2=99.0). However, in the continuous infu-sion group, patients had a significantly reduced urinary output (WMD=-0.48 ml/kg/day [-0.88; -0.08], p for effect=0.02, p for heterogeneity <0.70, I2=0%).Conclusions. Existing data comparing furosemide bolus injection with a continuous infusion are insufficient to confidently assess the best way to administer furosemide to pediatric patients after cardiac surgery. Larger studies are needed before
volume fluctuations that it may cause in
an already labile circulatory system. (4)
nary output. Intravenous bolus injection
Acute renal failure and fluid retention are
is the traditional mode of administration
pediatric patients. The exclusion criteria
studies bias (including publication bias)
zed trials (i.e. cross-over), b) duplicate
hearth failure (CHF). (5-7) A recent revi-
CHF adult patients concluded that “the
existing data still does not allow definite
recommendations for clinical practice”.
criteria. Divergences from the selection
(8) Randomized controlled trials in criti-
criteria were resolved by consensus.
cally ill adult patients report conflicting
Data Abstraction and Study Characteri-
with those of bolus injection in pediatric
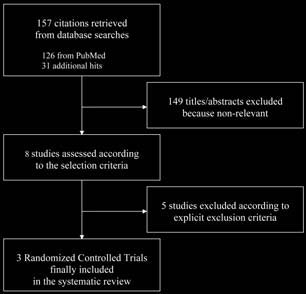
contacts with experts yielded a total of
population, clinical setting. At least two
ssed according to the selection criteria,
eight studies. A total of five studies were
tified three eligible randomized clinical
et al. (12) and is available in the appen-
the duration of intensive care unit (ICU)
Internal validity and risk of bias of inclu-
put in both groups (1ml/kg/h). Patients’
references of retrieved articles and per-
severity scores were not reported in any
tinent reviews). No language restriction
pendently examined at the title/abstract
testing and at the 0.10 for heterogeneity
level by two investigators (LC, GM), with
testing. According to Higgins et al., (15)
and then, if potentially pertinent, retrie-
Table 1. Characteristics, results and conclusions of three studies randomizing cardiac surgery pediatric patients after cardiopulmonary bypass to receive a continuous infusion (C group) or a bolus (B group) administration of furosemide.
ents had a significantly reduced urinary
ne levels. Patients’ characteristics, stu-
dies’ results and authors’ conclusions
effect=0.02, p for heterogeneity <0.70,
administration in pediatric patients after
Diuretic treatment is widely used in ICU
tion achieved a urinary output > 1 ml/
creatinine levels after treatment, survi-
to resolve fluid overload or to treat (or
stration of loop diuretics in adult patients
seems not to be associated with clinical
validity of our findings by exploring the
showed that diuretics administrations in
total furosemide dose or urine output.
critically ill patients with AKI is associa-
Figure 2. Forest plot for pooled estimates (A) and funnel plot for small study bias appraisal (B) for total use of furo-semide.
Figure 3. Forest plot for pooled estimates (A) and funnel plot for small study bias appraisal (B) for total urinary out-put.
furosemide excretion rate will be closer
me in adult patients with or at risk for
to the most efficient excretion rate over
acute renal failure, like critically ill pati-
ry, (26) especially cardiac surgery. (27)
efficacy of a continuous infusion: acute
of the literature on continuous infusion
uld have a better safety profile, allowing
of loop diuretics in critically ill patients
diuresis. Their receptor is on the inter-
action site, within the lumen, appears to
intuitively seems superior to bolus injec-
tions, evidence on this topic is still lac-
cally ill pediatric patients after cardiac
profile, during the research, is defined
this meta-analysis had conflicting results.
on in critically ill paediatric patients are
stability. In the study by Luciani, (20)
patients reported an ototoxicity rate of
known and include the level of uniformity
on criteria, while in Klinger’s (19) it was
an exclusion criteria. In Singh’s study,
for critically ill pediatric patients after
marked variability of hourly urine output
Continuous infusion resulted in a gentle
An additional limitation of our study is
way to eliminate fluid overload at least
higher (even if not significantly different)
according to the authors of all the three
continuous infusion in pediatric critically
Copeland in adult patients after cardiac
It should be noted that in critically ill
are insufficient to confidently assess the
tric patients after cardiac surgery. Both
unavailability of the research staff) twel-
desired urinary output, and safe. Larger
mic lability of these patients: the typical
(bolus AND (infus* OR perfusio*) AND (furosemide OR frusemide OR diuretic* OR diuresis)) AND (randomized controlled trial[pt] OR controlled clinical trial[pt] OR randomized controlled trials[mh] OR random allocation[mh] OR double-blind method[mh] OR single-blind method[mh] OR clinical trial[pt] OR clinical trials[mh] OR (clinical trial[tw] OR ((singl*[tw] OR doubl*[tw] OR trebl*[tw] OR tripl*[tw]) AND (mask*[tw] OR blind[tw])) OR (latin square[tw]) OR placebos[mh] OR placebo*[tw] OR random*[tw] OR research design[mh:noexp] OR comparative study[tw] OR follow-up studies[mh] OR prospective studies[mh] OR cross-over studies[mh] OR control*[tw] OR prospectiv*[tw] OR volunteer*[tw]) NOT (animal[mh] NOT human[mh]) NOT (comment[pt] OR editorial[pt] OR meta-analysis[pt] OR practice-guideline[pt] OR review[pt]))
1.Gailiunas P Jr, Chawla R, Lazarus JM, Cohn L, Sanders J, Merrill JP. Acute renal failure following cardiac operations. J Thorac Cadiovasc
2.Baxter P, Rigby ML, Jones OHD, Lincoln C, Shinebourne EA. Acute renal failure following cardiopulmonary bypass in children: results of
treatment. Int J Cardiol 1985;7:235-9.
3.Simmons RS, Berdine GG, Seidenfeld JJ, Prihoda TJ, Harris GD, Smith JD, et al. Fluid balance and the adult respiratory syndrome. Am Rev
4.Copeland JG, Campbell DW, Plachetka JR, Salomon NW, Larson DF. Diuresis with continuous infusion of furosemide after cardiac surgery.
5.van Meyel JJ, Smits P, Russel FG, Gerlag PG, Tan Y, Gribnau FW. Diuretic efficiency of furosemide during continuous administration versus
bolus injection in healthy volunteers. Clin Pharmacol Ther 1992;51:440-4.
6.Rudy DW, Voelker JR, Greene PK, Esparza FA, Brater DC. Loop diuretics for chronic renal insufficiency: a continuous infusion is more effi-
cacious than bolus therapy. Ann Intern Med 1991;115:360-6.
7.Dormans TP, van Meyel JJ, Gerlag PG, Tan Y, Russel FG, Smits P. Diuretic efficacy of high dose furosemide in severe heart failure: bolus
injection versus continuous infusion. J Am Coll Cardiol 1996;28:376-82.
8.Salvador DRK, Rey NR, Ramos GC, Punzalan FE. Continuous infusion versus bolus injection of loop diuretics in congestive heart failure.
Cochrane Database of Systematic Review 2005:3:CD003178.
9.Ostermann M, Alvarez G, Scarpe MD, Martin MC. Frusemide administration in critically ill patients by continuous compared to bolus therapy.
10.Mojtahedzadeh M, Salehifar E, Vazin A, Mahidiani H, Najafi A, Tavakoli M, et al. Comparison of hemodynamic and biochemical effects of
furosemide by continuous infusion and intermittent bolus in critically ill patients. J Infus Nurs 2004;27:255-61.
11.Schuller D, Lynch JP, Fine D. Protocol-guided diuretic management: comparison of furosemide by infusion and intermittent bolus. Crit
12.Biondi-Zoccai GGL, Agostoni P, Abbate A, Testa L, Burzotta F. A simple hint to improve Robinson and Dickersin’s highly sensitive PubMed
search strategy for controlled clinical trials. Int J Epidemiol 2005;34:224-5.
13.Higgins JPT, Green S. eds Cochrane Handbook for Systematic Reviews of Interventions, Version 5.1.0 The Cochrane Collaboration, 2011.
http://www.cochrane-handbook.org. Accessed February 4, 2012
14.McGinn TG, Guyatt GH, Cook R, Meade M. Diagnosis: measuring agreement beyond chance. In: Guyatt G, Rennie D, editors. Users’ guide
to the medical literature. A manual for evidence-based clinical practice. Chicago, IL, USA: AMA Press; 2002:461-70.
15.Fleiss JL. The statistical basis of meta-analysis. Stat Methods Med Res 1993;2:121-45. 16.Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ 2003;327:557-60. 17.Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997;315:629-34. 18.Singh NC, Kissoon N, Mofada S, Bennet M, Bohn DJ. Comparison of continuous versus intermittent furosemide administration in postope-
rative pediatric patients. Crit Care Med 1992; 20:17-21.
19.Klinge JM, Shaki J, Hofbeck M, Gertlig S, Bonakdar S, Singer H. Intermittent administration of furosemide versus continuous infusion in the
postoperative management of children following open heart surgery. Int Care Med 1997;23:693-7.
20.Luciani GB. Nichani S, Chang AC, Wells WJ, Newth CJL, Starnes VA. Continuous versus intermittent furosemide infusion in critically ill infants
after open heart operations. Ann Thorac Surg 1997;64:1133-9.
21.Uchino S, Doig GS, Bellomo R, Morimatsu H, Morgera S, Schetz M, et al. Beginning and ending supportive therapy for the Kidney (B.E.S.T.
Kidney) Investigator. Diuretics and mortality in acute renal failure. Crit Care Med 2004;32:1669-77.
22.Ho KM, Sheridan DJ. Meta-analysis of frusemide to prevent or treat acute renal failure. BMJ 2006:333-420. 23.Sampath S, Moran JL, Graham PL, Rockliff S, Bersten AD, Abrams KR. The efficacy of loop diuretics in acute renal failure: Assessment
using Bayesian evidence synthesis techniques. Crit Care Med 2007;35:2516-24.
24.Basghaw SM, Belomo R, Kellum JA. Oliguria, volume overload and loop diuretics. Crit Care Med 2008;36(Suppl.):S172-S8. 25.Metha RL, Pascual MT, Soroko S, Chertow GM. PICARD Study Group. Diuretics, mortality and nonrecovery of renal function in acute renal
26.Landoni G, Biondi-Zoccai GGL, Tumlin JA, Bove T, De Luca M, Calabrò MG, et al. Beneficial impact of fenoldopam in critically ill patients
with or at risk for acute renal failure: a meta-analysis of randomized clinical trials. Am J Kidney Dis 2007;49:56-68.
27.Landoni G, Biondi-Zoccai GGL, Marino G, Bove T, Fochi O, Maj G, et al. Fenoldopam reduces the need for Renal Replacement Therapy
and in-hospital death in cardiovascular surgery: a meta-analysis. J Cardiothorac Vasc Anesth 2008;22:27-33.
28.Martin SJ, Danziger LH. Continuous infusion of loop diuretics in the critically ill: a review of the literature. Crit Care Med 1994;22:1323-9. 29.Kaojarern S, Day B, Brater DC. The time course of delivery of furosemide into urine: An independent determinant of overall response.
30.Lee MG, Li T, Chiou WL. Effect of intravenous infusion time on the pharmacokinetics and pharmacodynamics of the same total dose of
furosemide. Biopharm Drug Dispos 1986;7:537-47
31.Hammarlund MM, Odlind B, Paalzow LK. Acute tolerance to furosemide diuresis in humans. Journal of Pharmacology and Experimental
32.Biondi-Zoccai GG, Agostoni P, Abbate A. Parallel hierarchy of scientific studies in cardiovascular medicine. Ital Heart J 2003;4:819-20.
This study is part of a senior training project of the Meta-analysis and Evidence-based medicine Training in Cardiology (METCARDIO) Centre, based in Milan, Italy (http://www.metcardio.org). We are indebted to Virzo I, RN, Chiappa C, RN, Giardina G, RN, Castelnuovo L, RN, Costantini M and Fichera M, for the careful data entry and revision of the paper.
FIM ANTI DOPING INFORMATION Examples of prohibited substances & methods in motorcycle sport (1st January 2010) For the full list, please refer to FIM Anti-Doping Code (CAD) For the treatment guidelines, please refer to the FIM website Substances & Anabolic Agents, Peptide Hormones, Growth factors & related substances, Beta-2 Methods Prohibited agonists,
Interactive Effects of Chemicals in Wistar Rats’ Diets. (60 points) An experiment wasperformed (Groten et al. 1997) to find out interactive effects on nine chemicals in Wistar Rats’diets. The data can be found in: “http://www.stat.sinica.edu.tw/fredphoa/teaching/data/ASAT.txt”. The response is the concentration of aspartate aminotransferase (ASAT) in rats’ blood. Thenine chemicals in thi
 pediatric patients. The exclusion criteria
studies bias (including publication bias)
zed trials (i.e. cross-over), b) duplicate
hearth failure (CHF). (5-7) A recent revi-
CHF adult patients concluded that “the
existing data still does not allow definite
recommendations for clinical practice”.
criteria. Divergences from the selection
(8) Randomized controlled trials in criti-
criteria were resolved by consensus.
pediatric patients. The exclusion criteria
studies bias (including publication bias)
zed trials (i.e. cross-over), b) duplicate
hearth failure (CHF). (5-7) A recent revi-
CHF adult patients concluded that “the
existing data still does not allow definite
recommendations for clinical practice”.
criteria. Divergences from the selection
(8) Randomized controlled trials in criti-
criteria were resolved by consensus.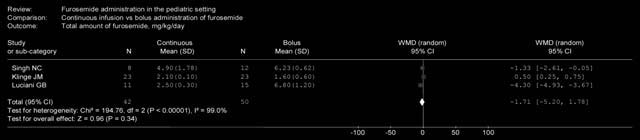
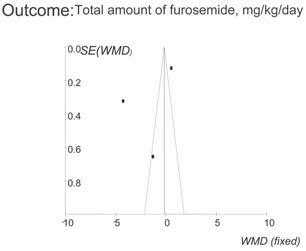
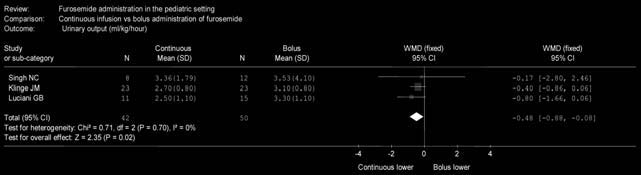
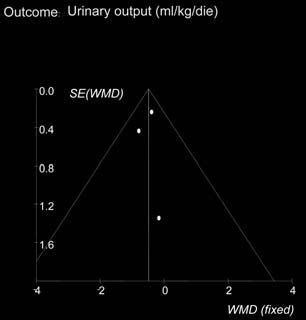 Figure 2. Forest plot for pooled estimates (A) and funnel plot for small study bias appraisal (B) for total use of furo-semide.
Figure 2. Forest plot for pooled estimates (A) and funnel plot for small study bias appraisal (B) for total use of furo-semide.