Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
Portalqualis.com.br
Asymptomatic Babesiosis in a Child With Hepatoblastoma
Angela Rech, MD, Christina Matzenbacher Bittar, MD, Cláudio Galvão de Castro Jr., MD, MsC,Kenia Rosário Azevedo, MD, Rodrigo Pires dos Santos, MD, Adão Rogério Leal Machado, MD, MsC,Gilberto Schwartsmann, MD, PhD, Luciano Goldani, MD, PhD, and
Babesiosisisatickborneillnesscausedbytheredbloodcell
parasite Babesia sp.1 Recent studies have shown that Ba-besia can persist asymptomatically for long periods2 and canbe acquired from sources other than ticks, such as blood trans-fusions.3 The first report of a human case of Babesia (Babesiabovis) infection occurred in Yugoslavia in 1956.4 A case ofhuman babesiosis was described in an adult in Brazil.5
CASE REPORT
A 2-year-old boy was referred to us in September 2002
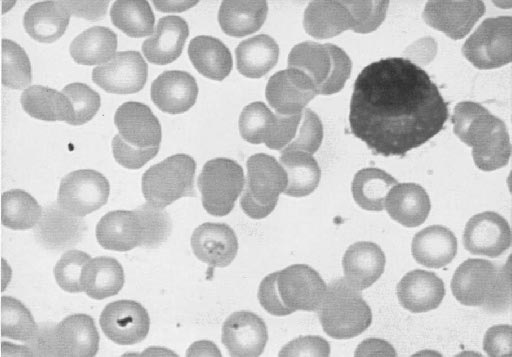
with a fetal hepatoblastoma with pulmonary metastasis. Mi-croscopic examination of blood smears revealed red blood cellinclusions consistent with Babesia microti (Fig. 1). The familyreported no previous contacts with wild animals, no priorblood transfusions, and no recent travel. The patient was
FIGURE 1. Peripheral blood with red blood cells showing in-
placed on antibiotic treatment with clindamycin. Posttreat-
clusions consistent with Babesia microti (ן1,000).
ment evaluation showed no evidence of babesiosis in the pe-ripheral blood. He was then started on chemotherapy using a
immunocompromised patients.3 Our patient presented with an
combination of cisplatin, carboplatin, and doxorubicin. The tu-
asymptomatic form of babesiosis and a moderate degree of
mor was completely resected in March 2003 but relapsed lo-
parasitemia, which was diagnosed by incidental observation of
cally 2 months after surgery. The family refused further treat-
the presence of parasites. Confirmatory tests such as PCR or
ment and the patient was provided with palliative therapy.
ELISA were not performed in this patient. Malaria could bemisdiagnosed as babesiosis, but the endemic region of this dis-
DISCUSSION
ease starts more than 1,500 km north of our state. Physicians
As babesiosis is not a common disease in Brazil, it is
should be aware of babesiosis, even in a region with no previ-
possible that some cases have been misdiagnosed or not re-
ously reported cases. This is particularly relevant when treat-
ported. In the past decade, cases of babesiosis in humans have
ing immunocompromised patients, who may have severe
been reported with increasing frequency, especially in the
northeastern United States.6 Most cases of B. microti infectionare relatively asymptomatic in the immunocompetent host. In
REFERENCES
contrast, babesiosis can be a severe and life-threatening infec-
1. Hatcher JC, Greenberg PD, Antique J, et al. Severe babesiosis in Long
tion, especially in splenectomized, HIV-positive, and other
Island: Review of 34 cases and their complication. Clin Infect Dis. 2001;32:1117–1127.
2. Krause P, Spielman A, Telford III Sr, et al. Persistent parasitemia after
Received for publication June 2, 2003; accepted August 1, 2003.
acute babesiosis. N Engl J Med. 1998;339:160–165.
3. Dobroszycki J, Herwaldt B, Boctor F, et al. A cluster of transfusion-
From the Pediatric Oncology Unit, Clinical Pathology Unit, and Medical On-
associated babesiosis cases traced to a single asymptomatic donor. JAMA.
cology Unit, Hospital de Clínicas de Porto Alegre, Universidade Federal
do Rio Grande do Sul, Porto Alegre, Brazil.
4. Steketee RW, Eckman MR, Burgess E, et al. Babesiosis in Wisconsin.
Reprints: Angela Rech, MD, Hospital de Clinicas de Porto Alegre, Pediatric
Oncology Unit, Rua Ramiro Barcelos 2350,3 leste, 90035-003 Porto
5. Alecrim I, Pinto B, Avila T, et al. Registo do primeiro caso de infecção
Alegre, RS, Brazil (e-mail: arech@hcpa.ufrgs.br or angelrech@ig.
humana por Babesia sp no Brazil. Rev Patol Trop. 1983;12:11–29.
6. Mylonakis E. When to suspect and how to monitor babesiosis. Am Fam
Copyright 2004 by Lippincott Williams & Wilkins
Physician. 2001;63:1969–1974. J Pediatr Hematol Oncol • Volume 26, Number 3, March 2004
Donation after Brainstem Death Donor Optimisation Extended Care Bundle Trust / Regional collaborative / CCN logo Patient Name______________________ Date of Birth______________ Priorities to address are 1. Assess fluid status and correct hypovolaemia with fluid boluses Fluids and metabolic management 2. Introduce vasopressin infusion where required introduce flow monitoring 1. A
Economic Evaluation of ASCOT-BPLA: Antihypertensive treatment with an amlodipine-based regimen is cost-effective compared to an atenolol-based regimen Peter Lindgren, Martin Buxton, Thomas Kahan, et al. Updated information and services can be found at: Published online October 4, 2007 in advance of the print journal. Email alerting Receive free email alerts when new articles cite this

 Asymptomatic Babesiosis in a Child With Hepatoblastoma
Angela Rech, MD, Christina Matzenbacher Bittar, MD, Cláudio Galvão de Castro Jr., MD, MsC,
Kenia Rosário Azevedo, MD, Rodrigo Pires dos Santos, MD, Adão Rogério Leal Machado, MD, MsC,
Gilberto Schwartsmann, MD, PhD, Luciano Goldani, MD, PhD, and
Babesiosisisatickborneillnesscausedbytheredbloodcell
parasite Babesia sp.1 Recent studies have shown that Ba-
besia can persist asymptomatically for long periods2 and canbe acquired from sources other than ticks, such as blood trans-fusions.3 The first report of a human case of Babesia (Babesiabovis) infection occurred in Yugoslavia in 1956.4 A case ofhuman babesiosis was described in an adult in Brazil.5
CASE REPORT
Asymptomatic Babesiosis in a Child With Hepatoblastoma
Angela Rech, MD, Christina Matzenbacher Bittar, MD, Cláudio Galvão de Castro Jr., MD, MsC,
Kenia Rosário Azevedo, MD, Rodrigo Pires dos Santos, MD, Adão Rogério Leal Machado, MD, MsC,
Gilberto Schwartsmann, MD, PhD, Luciano Goldani, MD, PhD, and
Babesiosisisatickborneillnesscausedbytheredbloodcell
parasite Babesia sp.1 Recent studies have shown that Ba-
besia can persist asymptomatically for long periods2 and canbe acquired from sources other than ticks, such as blood trans-fusions.3 The first report of a human case of Babesia (Babesiabovis) infection occurred in Yugoslavia in 1956.4 A case ofhuman babesiosis was described in an adult in Brazil.5
CASE REPORT