Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
Pubs.sciepub.com
American Journal of Pharmacological Sciences, 2013, Vol. 1, No. 5, 74-79 Available online at http://pubs.sciepub.com/ajps/1/5/1 Science and Education Publishing DOI:10.12691/ajps-1-5-1
Pharmacokinetics of Indomethacin in Chronic Migraine Patients after Withdrawal from the Overused Combination of Indomethacin, Prochlorperazine and Caffeine Anna Ferrari1,*, Diego Pinetti1, Daniela Gallesi1, Alfio Bertolini1, Grazia Sances2, Emilio Sternieri1
1Division of Toxicology and Clinical Pharmacology, Headache and Drug Abuse Inter-Department Research Centre, University of
2Headache Unit, IRCCS C. Mondino, University of Pavia, Pavia, Italy
*Corresponding author: anna.ferrari@unimore.it
Received January 13, 2013; Revised September 20, 2013; Accepted September 23, 2013 Abstract Indomethacin, in combination with prochlorperazine and caffeine (IPC), is often overused by migraine patients who develop medication-overuse headache. Indomethacin clearance is slower in chronic migraine patients overusing IPC combination than in migraine patients only occasionally taking it. The objective of this study was to verify if indomethacin reduced clearance reverted to normal values after withdrawal of the overused IPC combination. Therefore, we repeated the study of indomethacin pharmacokinetics in 9 female chronic migraine patients after 3 months from inpatient withdrawal treatment from IPC combination overuse. The IPC combination (indomethacin 50 mg, prochlorperazine 8 mg, caffeine 150 mg) habitually taken was administered by rectal route to each patient. Blood samples were drawn before dosing and at the following post-dose times: 0.5, 1, 2, 3, 4, and 6 h. Indomethacin concentrations were measured by HPLC method. We found that 4 of 9 patients (group A) who were still overusing the combination and suffering from daily headache had still high indomethacin concentrations after 6 hours, therefore showing a slow elimination of the drug. Instead, in the 5 patients (group B) who had discontinued overuse of IPC combination after withdrawal treatment, indomethacin concentrations after 6 hours were significantly lower than those measured before withdrawal (P < 0.05, Student’s t-test for paired data), and also than those observed in group A (P < 0.05, ANOVA and Newman-Keuls’test). Hence, by suspending IPC abuse indomethacin clearance reverts to normal values and this is associated with an improvement of migraine. Instead, the higher plasma levels of indomethacin in patients who continue IPC abuse do not solve migraine and might support medication-overuse headache. Keywords: indomethacin, pharmacokinetics, chronic migraine, medication-overuse headache, drug combinations Cite This Article: Anna Ferrari, Diego Pinetti, Daniela Gallesi, Alfio Bertolini, Grazia Sances, and Emilio Sternieri, “Pharmacokinetics of Indomethacin in Chronic Migraine Patients after Withdrawal from the Overused Combination of Indomethacin, Prochlorperazine and Caffeine.” American Journal of Pharmacological Sciences 1, no. 5 (2013): 74-79. doi: 10.12691/ajps-1-5-1.
treatment, according to the guidelines by the Italian Society for the Study of Headaches at the third level
1. Introduction
of recommendation, when triptans, which are first recommended, result ineffective against nausea and
Indomethacin, an indole acetic acid derivative [1-(P-
vomiting. It is instead not recommended if migraine
chlorbenzoyl)-5-methoxy-2 methylindole-3-acetic acid],
attacks have a medium/high frequency, because of the
structurally related to serotonin, is a potent non-selective
potential risk of overuse In spite of this, a large
inhibitor of cyclooxygenases, with central analgesic
number of chronic daily headache patients who overuse
properties In Italy, it is one of the most used drugs for
IPC combination are referred to the Headache Centre of
acute headache treatment, in a fixed combination with
the University of Modena, Italy These patients
prochlorperazine and caffeine, which is available on the
reported that this medication was initially an
market in oral (tablets: indomethacin 25 mg, extraordinarily effective antimigraine drug, but then, year prochlorperazine 2 mg, caffeine 75 mg) and rectal
by year, they had to increase daily dosages and intake
(suppositories: indomethacin 50 mg, prochlorperazine 8
frequency gradually, sometimes up to true abuse, because
mg, caffeine 150 mg; mild suppositories: indomethacin 25
of a gradual reduction in its effectiveness (both in the
mg, prochlorperazine 4 mg, caffeine 75 mg) formulations.
intensity and duration of the effect). At the same time,
This combination (IPC) is indicated for acute headache
American Journal of Pharmacological Sciences
their headache turned into chronic daily headache. We
2. Patients and Methods
supposed that this gradual reduction in the effectiveness of IPC combination was related to an accelerated elimination
2.1. Subjects
of its components and, consequently, to plasma levels insufficient for therapeutic effects. We therefore studied
We studied again the kinetics of indomethacin after
the pharmacokinetics of each component of this giving IPC combination to 9 female subjects (all medication in migraine patients occasionally taking it and
Caucasian) suffering from chronic migraine and
in chronic migraine patients overusing it Contrary to
medication-overuse headache according to ICDH-II
our hypothesis, the elimination of the components of IPC
classification criteria 3 months after withdrawal
combination is not accelerated in overusing subjects:
treatment from overuse (7-10 days of hospitalization with
indomethacin clearance is instead reduced and its half-life
standardized treatment; at discharge, a prophylactic
longer in chronic migraine patients overusing this
treatment with amitriptyline in the oral dosage of 30-60
combination than in episodic migraine patients only
mg/day was prescribed to every patient). Before
occasionally taking it. On the other hand, there are no
withdrawal treatment, all these patients had only been
significant differences in the kinetics of caffeine and
overusing IPC combination for at least one year, taking
prochlorperazine between subjects occasionally taking
daily one or more suppositories of this medication,
IPC combination and patients overusing These
containing indomethacin 50 mg, prochlorperazine 8 mg,
results suggest that in chronic migraine patients overusing
and caffeine 150 mg. In these patients, the diagnosis of
IPC combination, just indomethacin high concentrations
headache at the onset was migraine without aura. In time,
could have sustained and perpetuated medication-overuse
their migraine became chronic. In each patient, the
kinetics of indomethacin had already been studied before
The objective of our study was therefore to verify if the
withdrawal treatment the follow-up, 3 months later,
reduced systemic indomethacin clearance found in 4 of these patients (group A) had relapsed into daily use of patients overusing IPC combination disappeared once
one or more suppositories of IPC combination and still
overuse was discontinued. Hence, we studied again the
suffered from daily headache, while 5 patients (group B)
kinetics of indomethacin in the same patients who had
had a reduced headache frequency and were taking IPC
been previously studied, 3 months after withdrawal
combination only occasionally and with full effectiveness
treatment from overuse, and we analysed if there were
. The frequency of drug intake was recorded in
differences in the kinetics of indomethacin, following IPC
the diaries that patients kept until the follow-up. Informed
combination administration, between patients who had
consent was obtained from each subject, following the
steadily discontinued overuse, with a clear improvement
description of the study’s procedures and objectives. The
in their headache, and those who had instead relapsed into
study was approved by the ethical committees of Modena
overuse and whose headache was still chronic.
and Pavia and it was conducted in compliance with the declaration of Helsinki, latest version.
Table 1. Patients’ characteristics (mean+S.D.; range in brackets)
a P < 0.05 vs. after withdrawal, group B before and after withdrawal (ANOVA and Newman-Keuls’test) b P < 0.05 vs. group B after withdrawal (ANOVA and Newman-Keuls’test) c P < 0.05 vs. group B after withdrawal (ANOVA and Newman-Keuls’test)
No patient was a smoker, had kidney or liver
2.2. Procedures
dysfunction or was taking drugs able of causing drug-drug interactions with the components of IPC combination. In
Experimental sessions were conducted at the in-patient
particular, no patient was taking other drugs known as
ward of the Headache Centres of Modena and Pavia
inducers or inhibitors of cytochrome P450 2C9 (CYP2C9)
University Hospitals. Under medical surveillance, the IPC
All patients complained of gastrointestinal troubles,
combination habitually taken (indomethacin 50 mg,
two patients of group A were taking lansoprazole 30
prochlorperazine 8 mg, and caffeine 150 mg) was rectally
mg/day, and three (one in group A and two in group B)
administered to each patient, at 7 AM, after overnight
were taking antihypertensive agents (lisinopril, fasting. Patients were maintained in supine position for the candesartan, amiloride/hydrochlorothiazide). At the time
subsequent 30 minutes. Venous blood samples were
of the experimental session, patients did not present acute
drawn from an indwelling cannula into heparinized tubes,
diseases, according to histories and physical and before dosing and at the following post-dose times: 0.5, laboratory evaluations (blood chemistry, blood count,
1.0, 1.5, 2.0, 3.0, 4.0, and 6.0 hours. Samples were
immediately centrifuged, and kept at –20o C until the time
American Journal of Pharmacological Sciences
of assay. Indomethacin concentrations were measured on
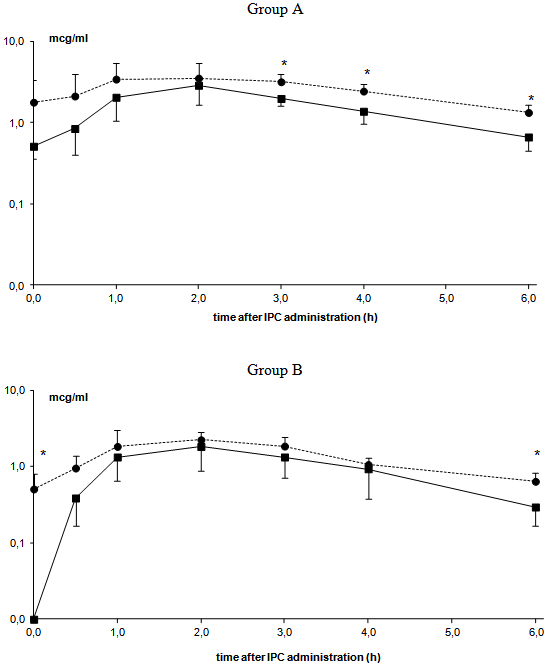
even when repeated after 3 months, in spite of the wide
deproteinized serum, by means of a slightly modified
inter-individuals variations observed above all in group A,
reversed-phase high-pressure liquid chromatographic and in the first 2 hours. After withdrawal treatment from (HPLC) meth A detailed description of the method
overuse of IPC combination, plasma indomethacin levels
had decreased at all times of the curve, both in group A and B, but only patients in group B, who had steadily
2.3.Analysis of the Data and Statistical
discontinued overuse and whose headache had
Evaluation
consequently improved, did not have measurable concentrations at baseline. Patients in group A, who were
Pharmacokinetic parameters were calculated by means
still overusing the combination (even if less than before)
of the P K Solutions 2.0 program (Non compartmental
and suffering from daily headache, had still high
pharmacokinetics data analysis, Summit Research indomethacin concentrations (even if much lower than Services, Montrose, CO, USA). The following parameters
before) after 6 hours, therefore showing a slow
were determined for indomethacin: Cmax, peak plasma
elimination of the drug. In patients of group B, who had
concentration (maximum observed plasma concentration)
discontinued overuse of IPC combination after withdrawal
(µg/ml); Tmax, time to peak plasma concentration (hr); t1/2,
treatment, indomethacin concentrations after 6 hours were
half-life clearance, time for concentration to diminish by
significantly lower than those measured before withdrawal
one-half (hr); MRT, mean residence time, time for 63.2%
(P < 0.05, Student’s t-test for paired data) and also than
of administered dose to be eliminated (hr); AUC0→t,
those observed in group A (P < 0.05, ANOVA and
cumulative area under the plasma concentration time
curve, only using observed data points (µg-hr/ml);
Before withdrawal treatment from overuse of IPC
AUC0→∞, total AUC, computed using data points combination, pharmacokinetic parameters of extrapolated to infinity (µg-hr/ml); Vd, apparent volume
of distribution, based on AUC∞ and clearance rate
significant differences between groups A and B (Student’s
normalized by weight (ml/Kg); Cl, systemic clearance,
t-test for unpaired data). After withdrawal from overuse,
the kinetics of indomethacin was still unchanged in
All data were expressed as mean ± S.D. When
patients of group A, who at the 3-months follow-up
appropriate, Student’s t-test for paired and unpaired data,
resulted to have relapsed into overuse of IPC combination
and ANOVA, followed by Newman-Keuls post hoc
(Student’s t-test for paired data). Instead, patients of group
testing, were performed to assess statistical difference
B, whose headache had improved after discontinuing
between the groups. A level of P < 0.05 was considered
overuse, had faster indomethacin elimination than before
(P < 0.05, Student’s t-test for paired data) and also faster clearance than patients of group A, who were still overusing the combination (P < 0.05, ANOVA and
3. Results
Newman-Keuls’test), as it was shown by the statistically significant increase of clearance and by the reduction,
The plasma time course of indomethacin levels,
even if not statistically significant, in t1/2, AUC0-t, and
following administration of one IPC suppository
AUC0-∞, in the absence of Tmax and Vd.
, had a similar pattern in the same group of patients,
Table 2. Pharmacokinetic parameters (estimated by non-compartmental method) of indomethacin following rectal administration of IPC combination (indomethacin 50 mg, prochlorperazine 8 mg, caffeine 150 mg) in 9 chronic migraine patients before and after 3 months from in- patient withdrawal from the overused IPC combination (Group A: patients who relapsed into overuse; Group B: patients who steadily discontinued overuse)
ml/hr/Kg a P < 0.05 vs before (Student’s t-test for paired data) b P < 0.05 vs group A before (ANOVA and Newman-Keuls’test) c P < 0.05 vs group B before, group A before and after (ANOVA and Newman-Keuls’ test)
American Journal of Pharmacological SciencesFigure 1. Plasma levels (mean ± S. D.) of indomethacin in patients of group A (upper panel) and of group B (bottom panel) before (●) and after (■) withdrawal from the overused IPC combination (statistical differences between mean levels: * P < 0.05, Student’s t-test for paired data)
hours, t1/2 2-11 hours, Cl 0.44 to 109 ml/min/kg, Vd 411-450 ml/kg)and comparable to those calculated in
4. Discussion
migraine patients only occasionally taking IPC combination (Tmax 1.62 ± 0.7 hours, t1/2 1.27 ± 0.4 hours,
Delayed indomethacin elimination, that we observed in
Cl 130.90 ± 30.2 ml/min/kg, Vd 235.31 ± 69.3 ml/Kg)
patients with chronic migraine overusing IPC combination
Notably, the normalization of the kinetics of indomethacin
(containing indomethacin 50 mg, prochlorperazine 8 mg,
in patients of group B, who had definitively suspended
and caffeine 150 mg), was reversible once overuse was
discontinued. Indomethacin clearan increased
improvement in migraine, which turned from daily into
significantly in these patients (group B), passing from
occasional, reducing its mean frequency to 6 ± 1.58 days
64.05 ± 30.16 ml/hr/Kg during overuse to 123.98 ± 39.91
per month. The high and sustained levels of indomethacin
ml/hr/Kg after steadily discontinuing overuse of IPC
, observed in patients of group A, both at
combination. All pharmacokinetic parameters of baseline (as likely residual of previous assumptions) and 6 indomethacin, calculated in subjects in group B after
hours after IPC administration, were instead associated
withdrawal from overuse of IPC combination, were
with overuse and chronic migraine. This pattern of plasma
consistent with published data obtained following indomethacin concentrations was certainly the administration of therapeutic dosages of indomethacin to
consequence of several and repeated daily intakes of IPC
healthy volunteers and rheumatic patients (Tmax 1 to 4
American Journal of Pharmacological Sciences
combination, since repeated doses of indomethacin tend to
of headache, and overused medication. We did not study
accumulate Moreover, indomethacin undergoes
the kinetics of all three components of IPC combination,
enterohepatic circulation In patients overusing IPC
because the disposition of caffeine and prochlorperazine is
combination, a higher and continual enterohepatic unchanged in migraine patients overusing IPC circulation could have caused reduced indomethacin
clearance. This modified disposition of indomethacin did
The present is one of the few studies on the kinetics of
not depend on metabolic characteristics of the patients
an acute migraine medication during overuse, apart from
studied. No patient, neither in group A nor B, suffered
from hepatic or kidney failure, or was taking medications
unrestricted use of ergotamine is often associated with
capable of inducing or inhibiting CYP2C9-mediated
ergotamine medication-overuse headach frequent use
of IPC combination can lead to reduced effect and dosage
Since a relationship between indomethacin plasma
escalation in trying to control headache. Hence, plasma
levels and degree of pharmacological effect has been
indomethacin levels which stayed higher than those in the
reported chronic migraine patients overusing IPC
therapeutic range for a long time [proposed therapeutic
combinations should steadily be free from headache.
concentration is 1 µg/mldid not resolve the headache
Instead, these patients said to have had to take more and
but, on the contrary, might have sustained medication-
more IPC combinations over time, because this overuse headache. On the other hand, in patients who only medication had become less and less effective against
occasionally took IPC combination after withdrawal
their migraine. Some patients of group A took up to 8
treatment, headache improved, the effectiveness of this
doses a day of IPC combination, that is, 400 mg/day of
medication was restored, indomethacin levels were lower
indomethacin, the double of the maximal therapeutic daily
dosage of 200 mg. This apparently paradoxical effect of
IPC combination is a widely used drug for acute
the overuse of IPC combination in migraine treatment
treatment of migraine attacks In our opinion, it is
(higher concentrations of indomethacin associated with
important to warn patients using this medication, and
reduced effectiveness) can be explained considering the
physicians prescribing it, that, even if IPC combination is
unique features of indomethacin, different from those of
composed of low dosages of three active principles,
the other NSAIDs. Indomethacin causes cerebral overuse of this medication might induce rebound vasoconstriction, which is rapid in onset and resolution,
headache and sustain medication-overuse headache.
closely related to plasma concentrations The mechanism of vasoconstriction induced by indomethacin is not fully understood. The other NSAIDs have been
Declaration of Interest
shown to have no effects on cerebral blood flowMoreover, the most common dose-dependent CNS
adverse reaction to indomethacin is headache. It has been attributed to compensatory vasodilatation that follows vasoconstriction In some cases, especially in the
References
morning, headache may be so severe to require discontinuation of the dr These peculiar [1] Hu XH, Tang HW, Li QS, Huang XF. Central mechanism of
indomethacin analgesia. Eur J Pharmacol 1994;263:53-7.
pharmacological properties are similar to those of
[2] Italian Society for the Study of Headaches. Ad Hoc Committee for
ergotamine and could support the ability of
the diagnostic and therapeutic guidelines for migraine and cluster
indomethacin to induce rebound headache, headache as a
toxic reaction, and, as a consequence, medication-overuse
[3] Ferrari A, Pasciullo G, Savino G, Cicero AFG, Ottani A, Bertolini
headache. In addition, caffeine contained in the IPC
A, Sternieri E. Headache treatment before and after the consultation of a specialized centre: a pharmacoepidemiology
combination can increase the antimigraine effect of
indomethacin, potentiating vasoconstriction but, at the
[4] Ferrari A, Savino G, Gallesi D, Pinetti D, Bertolini A, Sances G,
same time, it may contribute to the risk of inducing
et al. Effect of overuse of the antimigraine combination of
headache as a symptom of toxicity and withdrawal
indomethacin, prochlorperazine and caffeine (IPC) on the disposition of its components in chronic headache patients.
Ergotamine, triptans, and also indomethacin share some
characteristics, such as structural similarity to serotonin,
[5] Headache Classification Subcommittee of the International
the capacity of blocking neurogenic inflammation in
Headache Society. The International Classification of Headache
meningeal tissue, and vasoconstrictive properties, even if
Disorders, 2nd edition. Cephalalgia 2004;24 Suppl 1:9-160.
with a different degree of selectivity for blood vessels
[6] Nakajima M, Inoue T, Shimada N, Tokudome S, Yamamoto T,
Kuroiwa Y. Cytochrome P4502C9 catalyzes indomethacin O-
Furthermore, indomethacin is the only NSAID
demethylation in human liver microsomes. Drug Metab Dispos
reported to be effective in the treatment of cluster
[7] Avgerinos A, Malamataris S. High performance liquid
sumatriptan. We think that migraine patients overusing
chromatographic determination of indomethacin in human plasma and urine. J Chromatogr 1989;495:309-13.
IPC combination can develop a state of physical
[8] Normann G, Streiner D. Biostatistics. The bare essentials. 2nd Ed.
dependency on this medication. The condition looks like
Ontario, Canada: B.C. Decker Inc., 2000:1-162.
ergotamine dependency, which is characterized by an
[9] Emori HW, Paulus H, Bluestone R, Champion DG, Pearson C.
irresistible and predictable daily use of ergotamine as the
Indomethacin serum concentrations in man. Ann Rheum Dis
only mean of alleviating rebound headach
Our results have the limitation of having been obtained
Holt LPJ, Hawkins CF. Indomethacin: studies of absorption and of the use of indomethacin suppositories. Br Med J 1965;1:1354-6.
in a small number of patients, which, however, represent a homogeneous group for demographic characteristics, kind
American Journal of Pharmacological Sciences
[11] Hvidberg E, Lausen HH, Jansen JA. Indomethacin: plasma
[22] Helleberg L. Clinical pharmacokinetics of indomethacin. Clin
concentrations and protein binding in man. Eur J Clin Pharmacol
[23] Asmark H, Lundberg PO, Olsson S. Drug-related headache.
[12] Alvan G, Orme M, Bertillsson L, Ekstrand R, Palmer L.
Pharmacokinetics of indomethacin. Clin Pharmacol Ther
[24] Saper JR, Jones JM. Ergotamine tartrate dependency: features and
possible mechanisms. Clin Neuropharmacol 1986;9:244-56.
[13] Kuang C, Yeh KC. Pharmacokinetic overview of indomethacin
[25] Matthew RJ, Wilson WH. Caffeine consumption, withdrawal and
and sustained-release indomethacin. Am J Med 1985;79:3-12.
cerebral blood flow. Headache 1985;25:305-9.
[14] Schuster V, von Stockhausen HB, Seyberth HW. Effects of highly
[26] Silberstein SD, McCrory DC. Ergotamine and dihydroergotamine:
overdosed indomethacin in a preterm infant with symptomatic
history, pharmacology and efficacy. Headache 2003;43:144-66.
patent ductus arteriosus. Eur J Pediatr 1990;149:651-3.
[27] Jhee SS, Shiovitz T, Crawford AW, Cutler NR. Pharmacokinetics
[15] Duggan DE, Hooke KF, Noll RM, Kwan CK. Enterohepatic
and pharmacodynamics of the triptan antimigraine agents: a
circulation of indomethacin and its role in intestinal irritation.
comparative review. Clin Pharmacokinet 2001;40:189-205.
[28] Buzzi MG, Sakas DE, Moskovitz MA. Indomethacin and
[16] Rodrigues AD. Impact of CYP2C9 genotype on pharmacokinetics:
acetylsalicylic acid block neurogenic plasma protein extravasation
are all ciclooxygenase inhibitors the same? Drug Metab Dispos
in rat dura madre. E J Pharmacol 1989;165:252-8.
[29] Geaney DP. Indomethacin-responsive episodic cluster headache. J
[17] O’Donovan DJ, Fernandes CJ, Nguyen NY, Adams K, Adams JM.
Neurol Neurosurg Psychiatry 1983;46:860-1.
Indomethacin therapy for patent ductus arteriosus in premature
[30] Klimek A. Indomethacin-responsive episodic cluster headache. J
infants: efficacy of a dosing strategy based on a second-dose peak
Neurol Neurosurg Psychiatry 1984;47:1058-9.
plasma indomethacin level and estimated plasma indomethacin
[31] Buzzi MG, Formisano R. A patient with cluster headache
responsive to indomethacin: any relationship with chronic
[18] Nilsson F, Bjorkman S, Rosén I, Messeter K, Nordstrom CH.
paroxysmal hemicrania? Cephalalgia 2003;23:401-4.
Cerebral vasoconstriction by indomethacin in intracranial
[32] Anghileri E, Toso V, Perini F. Acute myocardial infarction after
hypertension. Anesthesiology 1995; 83:1283-92.
sumatriptan administration for cluster headache. Neurol Sci
[19] Nitter WH, Johnsen LF, Eriksen M. Acute effects of indomethacin
on cerebral blood flow in man. Pharmacology 1995;51:48-55.
[33] Ala-Hurula V, Myllyla V, Hokkanen E. Ergotamine abuse: results
[20] Imberti R, Fuardo M, Bellinzona G, Pagani M, Langer M. The use
of ergotamine discontinuation with special reference to the plasma
of indomethacin in the treatment of plateau waves: effects on
concentrations. Cephalalgia 1982;2:189-95.
cerebral perfusion and oxygenation. J Neurosurg 2005;102:455-9.
[34] Tfelt-Hansen P, Paalzow L. Intramuscular ergotamine: plasma
[21] Rasmussen M, Paulsen PH, Treiber A, Delahaye S, Tankisi A,
levels and dynamic activity. Clin Pharmacol Ther 1985;37:29-35.
Cold GE, et al. No influence of the endothelin receptor antagonist
[35] Hoy SM, Scott LJ. Indomethacin/prochlorperazine/caffeine: a
bosentan on basal and indomethacin–induced reduction of cerebral
review of its use in the acute treatment of migraine and in the
blood flow in pigs. Acta Anaesthesiol Scand 2003;47:200-7.
treatment of episodic tension-type headache. CNS Drugs 2011; 24: 343-58.
Pilot RCT of SSRI vs Bupropion: Effects on Suicidal Behavior, Ideation and Mood in MDD with Past Attempt or Current Ideation Michael F. Grunebaum; Steven Ellis; Naihua Duan; Ainsley Burke;This poster is presented in columns for online reading. You may also see the poster in it Pilot RCT of SSRI vs Bupropion: Effects on Suicidal Behavior, Ideation and Mood in MDD with P
The Journal of Specialised Translation The ethical dimension of translation revision. An empirical study. Alexander Künzli, Stockholm University, Department of French, Italian and Classical Languages, Sweden ABSTRACT This paper investigates translation revision using think-aloud protocols. Ten professional translators were asked to think aloud while revising three draft transl
 American Journal of Pharmacological Sciences
Figure 1. Plasma levels (mean ± S. D.) of indomethacin in patients of group A (upper panel) and of group B (bottom panel) before (●) and after (■)
American Journal of Pharmacological Sciences
Figure 1. Plasma levels (mean ± S. D.) of indomethacin in patients of group A (upper panel) and of group B (bottom panel) before (●) and after (■)