Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
Newsletter
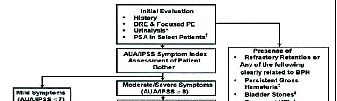
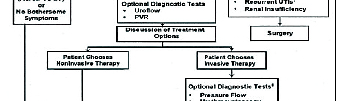
A NOTE FROM DR. THREATT Men with irritative as well as obstructive symptoms
should be evaluated for incomplete emptying. Use caution when prescribing anticholinergics (Detrol,
This is volume 2 of our newsletter; the focus will be Vesicare, Enablix, etc.) as these medications can result
on benign prostatic hypertrophy (BPH). This issue will in urinary retention. Checking a urine flow rate and a
provide you with current information on the evaluation post void residual is usually adequate. In diabetics and
and treatment of BPH from watchful waiting to surgical patients with neurogenic bladders (stroke, spinal cord
injury) urodynamics are usually helpful in directing
EDUCATION CORNER
management. Below is a helpful algorithm to use when managing
Lower urinary tract symptoms (LUTS)/BPH include, patients with BPH.
frequency, urgency, hesitancy, nocturia, incomplete emptying, weak urine stream, and post void dribbling. These symptoms occur in 25% of men older than 40 years of age and 33% of men older than 65 years of age. BPH is a progressive condition. Men 60 to 69 years of age with moderate LUTS have a 13% 10 year cumulative risk of urinary retention. The AUA Symptom index score (same as the International Prostate Symptom Score [IPSS]) is an important part of evaluating men with BPH. It is also important in grading the progression of disease or improvement after initiating therapy. The scale is comprised of 7 questions assessing both obstructive and irritative voiding complaints, and each question is graded on a scale of 1 to 5 depending on severity or frequency. IPSS scores of 0 to 7 are classified as mild, 8 to 19 as moderate and 20 to 35 as severe lower urinary tract symptoms (LUTS). Included in the scale is also a bother score graded 1 WATCHFUL WAITING
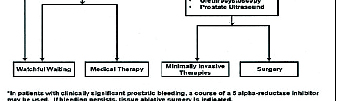
to 5; this allows the patient to rate the impact of the Men with low bothersome scores who don’t have a
disease process on their quality of life. Patients with history of urinary tract infections, renal dysfunction, or
mild to moderate LUTS and low bother scores should urinary retention are best treated in this manner. The
be treated with watchful waiting. Patients with high progression of BPH tends to be slow, and some patients
bother scores and/or high AUA index scores should be will actually have an improvement in their IPSS score
considered for treatment or further evaluation.
over time without intervention. Conservative treatment
The PSA and digital rectal exam are also important often includes decreasing fluid intake, eliminating or
in the evaluation of men with LUTS. Recently in the limiting caffeine, alcohol, salt and spicy foods.
medical literature the PSA has demonstrated a greater PHYTOTHERAPY
correlation with BPH. Please keep in mind that you The two most common herbals for prostate health are
will frequently encounter patients with low PSA’s and Serenoa repens (Saw Palmetto) and Pygeum africanum
severe BPH. The same holds true for men with very (Red stinkwood or African Plum).
large prostates and low IPSS scores. There are now A Meta analysis of randomized trials using Saw Palmetto
by Boyle et al (2859 patients enrolled) showed an
increase of 2.71mls/sec in peak flow rates compared to
A recent study compared the gold standard TURP to
0.5ms/sec in the placebo arm. There was also a decrease
microwave therapy. The TURP peak urinary flow rates
in nocturia by 1.19 events compared to 0.69 for placebo.
increased from 9.3ml/s to 19.1ml/s. The TUMT arm
An older Meta analysis showed that Saw Palmetto’s
improved from a pre-treatment flow rate of 9.3ml/
efficacy approached that of Finasteride (Proscar).
s to 15.1 ml/s. Patient’s subjective scores were also
The efficacy of Pygeum africanum is being evaluated
slightly better for the conventional TURP. Multiple
currently in a NIH longitudinal study (complimentary
studies have concluded that Microwave therapy is
and alternative medicine trial [CAMUS]). No study to
a solid option for BPH but is not equivalent to the
date with a placebo arm has been performed.
conventional TURP. TUMT is an excellent choice
for patients when pharmacotherapy has failed or
The AUA guideline committee believes that all 4
is contra-indicated, and the risks and morbidity of
alpha blockers (Alfuzosin, Doxazosin, Tamsulosin, and
Terazosin) are equally effective causing on average a
4 to 6 point improvement in the AUA symptom score.
Many clinicians feel the selective alpha-blockers
management. The introduction of the laser allows
Flomax and Uroxatrol are more effective than the
a different energy for achieving the same endpoint.
non selective. The rates of retrograde ejaculation are
The results of several prospective studies comparing
highest with Flomax. Uroxatral has a higher incidence
Electrocautery to laser TURP showed similar efficacy.
of hypotension in the selective alpha-blocker group.
Improvement in symptom score and increased peak
The alpha-blockers have a short onset of action but do
flow rates were equivalent. Voiding outcomes at 12
little to reduce the incidence of acute urinary retention.
months in both modalities were comparable.
Therefore they typically loose there benefit over time in
The benefits of the laser TURP over electrocautery is,
reduced risk of TUR syndrome, decreased irritative
voiding symptoms, less postoperative bleeding
Proscar and Avodart are the 2 drugs in this class. They
along with fewer electrolyte abnormalities.
work best in patients with large prostate glands > 40cc.
Electrocautery provides a tissue specimen for
These drugs tend to take 3 to 6 months before patients
pathology along with a shorter operative time.
see significant improvement in bother score; however their greatest benefit is in reducing the incidence of
EMERGING TREATMENTS
Our office is conducting two clinical trials on novel
therapies for BPH. One trial involves a one-time
The MTOPS study demonstrated combining an alpha
injection of medicine directly into the transitional
-blocker with a 5 alpha-reductase inhibitor worked
zone of the prostate. The other trial involves
better than either one alone at reducing not only the
a medication taken by mouth that has a new
AUA index score but slowing disease progression and
mechanism of action that addresses the prostate
MICROWAVE THERAPYThe first Microwave therapy (TUMT) was performed in
UPCOMING TOPICS
1982 for prostate cancer. In 1985 high-risk BPH patients
were treated. Currently TUMT is an option at most
stages of BPH. Microwave therapy works by heating
3. Renal, Bladder, Prostate, Testicular Cancer
the prostate adenoma while simultaneously cooling
There are a number of devices on the market with
varying efficacy. I have been fortunate to use four
machines and the Prolief system dilates and heats the
prostate during treatment and has provided the best
results. The procedure takes 45 minutes to 1 hour in
the office and requires only local anesthesia. Patients
typically bring something to read or music to listen to
Actas II Congreso Andaluz de Neuropsicología Autor/es: Salguero Alcañiz, María Pilar; Lorca Marín, José Andrés; Alameda Bailén, José Ramón. Título: Independencia funcional del conocimiento numérico léxico y la representación de la cantidad: evidencia de doble disociación. Introducción: En este trabajo se estudia el procesamiento numérico y el cálculo en dos pa
• They are more direct and give more and better context than indirect reports from professionals • They commonly describe the impact on people’s lives, which clinicians rarely note • Indirect and direct reports complement each other, generating multicultural knowledge • Knowledge of ADRs and their importance accumulates faster • Patients become active pa
 A NOTE FROM DR. THREATT Men with irritative as well as obstructive symptoms
A NOTE FROM DR. THREATT Men with irritative as well as obstructive symptoms