Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
Release.endoclab.pt
Clinical Chemistry 50:91650 –1655 (2004)
Hyperaldosteronism: Ratio of Plasma Aldosterone
to Renin Concentration Determined by Fully
Frank Holger Perschel,1* Rudolf Schemer,3 Lysann Seiler,4 Martin Reincke,4
Jaap Deinum,5 Christiane Maser-Gluth,6 David Mechelhoff,1 Rudolf Tauber,1 and
Background: The ratio of plasma aldosterone concen- between 298 and 6756 (pmol/L)/(ng ⅐ mL؊1 ⅐ h؊1) and tration to plasma renin activity (PAC/PRA) is the most PAC/PRC ratios between 105 and 2328 pmol/mU. common screening test for primary hyperaldosteronism Whereas PAC or PRC showed broad overlap between (PHA), but it is not standardized among laboratories. PHA patients and volunteers, the PAC/PRC ratio indi- We evaluated new automated assays for the simulta- cated distinct discrimination of these two groups at a neous measurement of PAC and plasma renin concen- cutoff of 71 pmol/mU. tration (PRC). Conclusion: The PAC/PRC ratio offers several practical Methods: We studied 76 healthy normotensive volun- advantages compared with the PAC/PRA screening teers and 28 patients with confirmed PHA. PAC and method. The present study offers preliminary evidence PRC were measured immunochemically in EDTA that it may be a useful screening test for PHA. Further plasma on the Nichols Advantage® chemiluminescence studies are required to validate these results, especially analyzer, and PRA was determined by an activity assay. in hypertensive cohorts. Results: In volunteers, PAC varied from 33.3 to 1930 2004 American Association for Clinical Chemistry pmol/L, PRA from 1.13 to 19.7 ng ⅐ mL؊1 ⅐ h؊1 (0.215 ng ⅐ mL؊1 ⅐ h؊1 ؍ 1 pmol ⅐ L؊1 ⅐ s؊1), and PRC from 5.70
Primary hyperaldosteronism (PHA)7 is recognized as the
to 116 mU/L. PAC/PRA ratios ranged from 4.35 to 494
most common endocrine form of secondary hypertension
(pmol/L)/(ng ⅐ mL؊1 ⅐ h؊1) and PAC/PRC ratios from 0.69
[see, e.g., Refs. (1– 6 )] with an estimated prevalence be-
to 71.0 pmol/mU. In PHA patients, PAC ranged from 158
tween 5% and 15% in the hypertensive population (7 ). to 5012 pmol/L, PRA from 0.40 to 1.70 ng ⅐ mL؊1 ⅐ h؊1,
Because diagnosis of PHA facilitates effective therapy,
and PRC from 0.80 to 11.7 mU/L. PAC/PRA ratios were
extended screening including normokalemic patients iswidely accepted (7–9 ).
The most common screening test for PHA is the ratio
of plasma aldosterone concentration to plasma renin
Clinical Chemistry and Pathobiochemistry and 2 Endocrinology, Diabe-
tes, and Nutritional Medicine, Charite´-Universita¨tsmedizin Berlin, Campus
activity (PAC/PRA) (7, 9 ). Because the measurement of
PRA requires special preanalytical prerequisites, is time-
3 Nichols Institute Diagnostics, Bad Vilbel, Germany. 4
consuming, and shows poor interlaboratory reproducibil-
Department of Internal Medicine II, University of Freiburg, Freiburg,
ity (10 –12 ), this strategy is not well recommended for
5 Department of Medicine, University Medical Center Nijmegen, Nijme-
screening of hypertensive patients in primary care cen-
ters. The lower limit of detection varies among the differ-
6 Department of Pharmacology, Ruprecht-Karls-University of Heidelberg,
*Address correspondence to this author at: Institut fu¨r Klinische Chemie
und Pathobiochemie, Charite´-Universita¨tsmedizin Berlin, Campus BenjaminFranklin, Hindenburgdamm 30, D-12200 Berlin, Germany. Fax 49-30-8445-
7 Nonstandard abbreviations: PHA, primary hyperaldosteronism; PAC,
4152; e-mail frank.perschel@charite.de.
plasma aldosterone concentration; PRA, plasma renin activity; PRC, plasma
Received February 23, 2004; accepted June 18, 2004.
renin concentration; RLU, relative light unit(s); APA, aldosterone-producing
Previously published online at DOI: 10.1373/clinchem.2004.033159
adenoma; and IHA, idiopathic hyperaldosteronism. Clinical Chemistry 50, No. 9, 2004
ent PRA assays; therefore, the effect on the PAC/PRA
concentrations, respectively, yielded renin values be-
ratio and the resulting cutoff values for PHA can be
dramatic (12 ). The validity and usefulness of the PAC/PRA ratio for screening for PHA has therefore been
Limits of detection and functional sensitivity. The limits of
detection, defined as the means plus 3 SD in two series of
Recently developed immunoassays for measurement
20 runs of the sample diluent, were 0.013 and 0.094
of circulating renin in plasma (PRC) may overcome this
mU/L, respectively. The functional sensitivity, defined as
limitation. However, studies evaluating these assays with
the sample renin concentration at which the CV for four
regard to the diagnosis of PHA are rare (16, 17 ). An
series of five assay runs is Ͻ20%, was 2.65 mU/L; 1 mU/L
additional problem is that the proposed cutoff values
is equivalent to 0.6 ng/L (18, 19 ).
published to date are derived from measurements of
The aldosterone assay on Nichols Advantage is a
aldosterone in either plasma (2, 3, 6, 11, 13, 15, 17 ) or se-
competitive one-site immunometric assay that uses a
rum (1, 4, 16 ) and are based on different assays. Because
biotinylated monoclonal antibody bound to streptavidin-
both PRA and PRC are measured in plasma and because
coated magnetic particles. Acridinium-ester-labeled aldo-
a simple screening test should be done from only a single
sterone competes with sample aldosterone for the limited
specimen, aldosterone should also be measured in plasma.
amount of biotinylated antibody. The cross-reactivity to
We therefore compared the “new” ratio between plasma
any steroid hormones is negligible. According to the
aldosterone concentration and plasma renin concentration
manufacturer’s package insert, the assay has an analytical
(PAC/PRC) with the established PAC/PRA screening test
sensitivity of 33.3 pmol/L, and the dynamic range is
in patients with PHA and in healthy volunteers to evalu-
0 –3330 pmol/L. The within-run imprecision (CV) at 119,
ate its clinical and diagnostic significance.
228, 547, 835, and 1990 pmol/L is 14.0%, 5.4%, 4.1%, 4.4%,and 2.9%, respectively. The total CV at 119, 228, 547, 835,
and 1990 pmol/L is 18.6%, 8.5%, 5.2%, 6.3%, and 4.9%,
respectively. Addition and dilution study results are
The PAC and PRC were measured on a fully automated
between 88% and 110%. Parallelism results are between
chemiluminescence analyzer (Nichols Advantage®; Ni-
91% and 116%. A method comparison with a commer-
chols Institute Diagnostics). This system incorporates sen-
cially available RIA gave a correlation coefficient of 0.96
sitive acridinium ester detection technology in combina-
and a slope of 1.04; 1 pmol/L is equivalent to 0.36 ng/L.
tion with magnetic particles as solid phase. Samples,
PRA was measured as described previously (10, 11 ).
reagents, and magnetic particles are pipetted into dispos-
The intraassay variation of this assay was 3.9% at 11.7
able cuvettes and incubated at 37 °C until the reaction is
ng ⅐ mLϪ1 ⅐ hϪ1; the interassay variation was 3.6% at 11.0
stopped by a washing step, and the emitted light is
ng ⅐ mLϪ1 ⅐ hϪ1 and 6.2% at 3.29 ng ⅐ mLϪ1 ⅐ hϪ1, respec-
measured in relative light units (RLU). The system is
tively. The detection limit was 0.40 ng ⅐ mLϪ1 ⅐ hϪ1 (0.215
calibrated by a two-point recalibration against a stored
ng ⅐ mLϪ1 ⅐ hϪ1 ϭ 1 pmol ⅐ LϪ1 ⅐ sϪ1).
All laboratory testing was done by qualified staff of the
PRC was measured with the Nichols Advantage Direct
Charite´. The study was not performed as a blind study.
ReninTM assay. This two-site immunometric assay uses an
Data analysis and estimation of cutoff values by ROC
acridinium-ester-labeled monoclonal antibody, a second
curve analysis were done with the Analyze-It software
biotinylated monoclonal antibody, and streptavidin-
coated magnetic particles. To avoid prorenin activationduring the assay, the incubation time is limited to 30 min
at 37 °C. This assay is calibrated to the WHO reference
We tested 76 healthy, normotensive volunteers [employ-
material (National Institute for Biological Standards and
ees and students of the Charite´; 23 males (age range, 22–75
years) and 53 females (age range, 16 – 69 years)], who were
In an evaluation study (18 ) this PRC assay showed the
not taking any relevant medications. Smoking and use of
oral contraceptives were not exclusion criteria. Bloodsamples were drawn in an upright sitting posture. Precision. The intraassay variation for three samples with
The patients studied included 28 patients with con-
various concentrations of renin was 1.7–5.3%. Interassay
firmed PHA [16 males and 12 females; mean (SD) age, 51
variation in seven samples with renin concentrations from
(13.1) years; age range, 26 –72 years]: 9 patients had
10 to 466.5 mU/L was between 2.7– 8.2%.
aldosterone-producing adenomas (APAs), 18 had idio-pathic hyperaldosteronism (IHA), and 1 patient had glu-
Accuracy. Dilution of four plasma samples with the sam-
cocorticoid-suppressible hyperaldosteronism. The charac-
ple diluent gave parallel lines whose slopes did not differ.
teristics of these PHA patients are summarized in Table 1.
Renin measurements in two series of mixtures prepared
The screening of our patients was done according to a
from two plasma samples with low and high renin
generally accepted protocol (7–9 ), in which plasma aldo-
Perschel et al.: Rapid Screening Test for PHA
Table 1. Characterization of 28 patients with confirmed PHA.aa For details on test protocols, see Quinkler et al. (8 ) and Young (12 ). Only specific medications, which were used after confirmatory and differential diagnostic tests,
were given. Most patients with IHA needed additional antihypertensive drugs. b Saline infusion test: ϩ, plasma aldosterone Ͼ230 pmol/L (Ͼ85 ng/L) after 2 L of isotonic saline; ND, not done. c 24-h Urinary aldosterone: ϩ, urinary aldosterone Ͼ39 nmol/day and urinary sodium Ͼ200 mmol/day; ND, not done; NU, not usable (urinary sodium Ͻ200
d Posture test: 2, decrease in plasma aldosterone; 1, increase in plasma aldosterone; NU, not useable because of concomitant increase in serum cortisol. e CT, computed tomography; MRT, magnetic resonance tomography; Spiro., spironolactone; GSH, glucocorticoid-suppressible hyperaldosteronism; Dexa.,
f CT or MRT: ϩ, unilateral tumor; Ϫ, no tumor. g Adrenal vein sampling: lateral., lateralization; ND, not done; NU, not usable because of unsuccessful catheterization. h Glucocorticoid-suppressible hyperaldosteronism was confirmed by genetic testing.
sterone was measured with a commercially available RIA
was done routinely in the outpatient clinics of the depart-
(not with the new immunometric assay) and had to be
ments of endocrinology at the Universities of Freiburg
Ͼ416 pmol/L (150 ng/L). The ratio between PAC and
PRA had to be Ͼ555 (pmol/L)/(ng ⅐ mLϪ1 ⅐ hϪ1) [Ͼ(200
For this evaluation study, separate blood samples were
drawn from all PHA patients in an upright sitting posi-
Diagnosis was confirmed by successful surgery (all
tion at 0800. The results presented in Tables 2– 4 and Fig.
APAs), pathologic saline infusion test (7–9 ), and in-
1 are from this standardized blood sampling. Although
creased 24-h urinary aldosterone excretion on a high-
several authors have recommended PAC/PRA screening
sodium diet (12 ) (for details see Table 1). Seven of the 28
without discontinuing hypertensive medications (20 –22 ),
patients were normokalemic [mean (SD) serum potas-
our study protocol for the evaluation of PAC/PRC was
sium, 3.4 (0.5) mmol/L; range, 2.0 – 4.3 mmol/L]. Systolic
the following: Most of the patients were on antihyperten-
blood pressure was between 140 and 220 mmHg [mean
sive therapy, but -blockers, angiotensin-converting en-
(SD), 179 (21) mmHg]; diastolic blood pressure was be-
zyme inhibitors, angiotensin antagonists, and diuretics
tween 80 and 140 mmHg [mean (SD), 104 (12.5) mmHg].
were stopped for at least 3 days and spironolactone for at
The described characterization of the PHA patients
least 4 weeks before blood sampling. Clinical Chemistry 50, No. 9, 2004
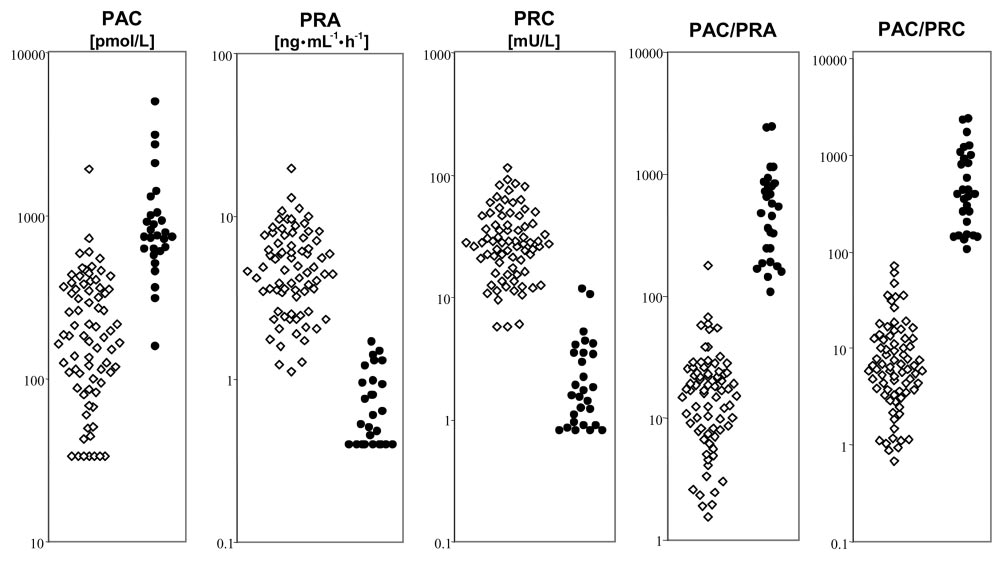
Fig. 1. PAC, PRA, PRC, and the resulting PAC/PRA and PAC/PRC ratios for 76 healthy volunteers and 28 patients with PHA.
The data points for PAC, PRA, PRC, and the ratios are plotted logarithmically; ᭛, healthy volunteers; F, patients with PHA.
ROC analysis (Table 3) showed the superiority of the
evaluation of pac assay on nichols advantage
ratios compared with PAC, PRA, and PRC alone. The
The intraassay imprecision (CV) at concentrations of 114,
PAC/PRC ratio performed at least as well as the PAC/
566, and 1906 pmol/L was 8.2%, 4.1%, and 4.4%, respec-
PRA ratio for differentiating PHA patients from healthy
tively. The interassay CV at 128, 611, and 1956 pmol/L
volunteers. With respect to the requirements of a screen-
was 20%, 6.6% and 4.2%, respectively.
ing test, we evaluated the cutoff values at a sensitivity of
The linearity on dilution was evaluated in two samples
with concentrations of 525 and 1141 pmol/L. The mea-sured concentrations were 76 –100% of the expected. Par-
allelism in two samples of different concentrations was
Because PHA is a common cause of secondary hyperten-
sion and its diagnosis can lead to cure or improvement of
Calibration stability was evaluated with eight different
calibrations. The CV was 3.0% for calibrator A (mean of60 127 RLU) and 3.2% for calibrator B (mean of 23 062
Table 2. PAC, PRA, PRC, and the resulting PAC/PRA and
RLU). The analytical sensitivity was 25 pmol/L.
PAC/PRC ratios for 76 healthy volunteers and 28 patients
All methods tested (Fig. 1 and Table 2) differed signifi-
cantly between PHA patients and healthy volunteers.
Whereas single measurements of PAC, PRA, or PRC
concentrations showed broad overlap between both
groups, the ratios PAC/PRA and PAC/PRC provided
distinct discrimination between these two groups.
PRC and PRA showed good correlation [Pearson re-
gression coefficient (r) ϭ 0.72]. Because the same PAC
values served for calculation of the ratios, PAC/PRC and
PAC/PRA correlated similarly (r ϭ 0.73). As expected,
differences occurred more frequently at the ends of lower
renin concentration and activity ranges near the detection
Perschel et al.: Rapid Screening Test for PHA
confirmed the assay specifications given by the manufac-
Table 3. Calculated cutoff values and resulting specificity
with respect to 100% sensitivity to differentiate patients
Because this is the first study with a fully automated
system and only two studies with manual PRC assays for
screening for PHA have been published to date (16, 17 ),
the comparison of our data with data from the literature is
limited. Trenkel et al. (16 ) suggested a cutoff value of 50
(aldosterone measured in serum by RIA, expressed in
ng/L; PRC measured by IRMA, expressed in ng/L),
which corresponds to 83 when using the units in Table 2
(PAC expressed in pmol/L, PRC in mU/L). Ferrari et al. (17 ) recommended a cutoff of 150 (aldosterone measuredin plasma by RIA, expressed in ng/L; PRC measured by
hypertension (APA) or targeted pharmacotherapy (IHA),
IRMA, expressed in ng/L) corresponding to 90 when
validated and cost-effective routine screening protocols
using the units in Table 2. Our data analysis (Tables 2 and
3; Fig. 1) produced a tentatively proposed cutoff value of
At present, the most common screening test is the ratio
71. Subsequent studies including essential hypertensive
between serum or plasma aldosterone (PAC) and PRA.
cohorts may necessitate readjustment, although there is
Because several authors have determined PAC/PRA cut-
good concordance with the recommendations made by
offs to screen for PHA (1–9 ), this procedure is widely
Trenkel et al. (16 ) and Ferrari et al. (17 ).
accepted as the best validated screening protocol. How-
Although the simultaneous measurement of PAC/PRC
ever, simultaneous measurement of PAC and PRA has
in plasma samples from 28 patients with known PHA
some disadvantages: The method for measuring PRA
showed no overlap with healthy volunteers (Fig. 1), there
requires cooling of the specimen during transport and
are certain limitations to our study: The PAC/PRC ratio
storage, is time-consuming, and shows weak interlabora-
seems to be superior to the PAC/PRA ratio. Although
tory reproducibility (10 –12 ). Because aldosterone is usu-
the PAC/PRA ratio of our PHA patients in the initial
ally measured in serum, determination of the PAC/PRA
outpatient characterization was clearly above the cutoff
ratio requires an additional, simultaneously drawn, blood
value of 555 (pmol/L)/(ng ⅐ mLϪ1 ⅐ hϪ1) [200 (ng/L)/
tube. In addition, PAC, PRA, and the PAC/PRA ratio
(ng ⅐ mLϪ1 ⅐ hϪ1)], the standardized reexamination of
show large intra- and interpatient variations in patients
these patients by use of a second blood sample showed
with PHA (15 ); therefore, several authors have cast doubt
that some patients would have failed this diagnostic
on the validity and sensitivity of the PAC/PRA ratio
criterion. Our proposed cutoff value (Table 3), which was
chosen to achieve a 100% sensitivity with the new auto-
Alternative screening procedures that overcome these
mated assay, was therefore somewhat lower than the
disadvantages seem to be necessary. Measurement of PRC
values recommended in the literature. In addition, some
instead of PRA may reduce some preanalytical and ana-
patients with confirmed PHA had PACs in the standard-
lytical problems and, therefore, improve intra- and inter-
ized reexamination that were Ͻ414 pmol/L (150 ng/L)
laboratory reproducibility (23, 24 ). Major advantages of
and therefore would also fail the second diagnostic crite-
the new PAC and PRC assays evaluated in our study
include the ease and performance of the test (no cooling,
Because there is no doubt in the correct characteriza-
a single plasma sample, and good interlaboratory repro-
tion of our patients as having PHA, we have two expla-
ducibility because the assays are automated) and the
nations for these findings: (a) a recent study by Tanabe et
rapid availability of results (automated immunochemilu-
al. (15 ) has demonstrated high intraindividual variability
minometric assays), which is a prerequisite for extensive
of PAC, PRA, and the PAC/PRA ratio in patients with
screening of hypertensive patients for PHA.
PHA; and (b) we measured plasma aldosterone with the
The performance of the new PAC assay was evaluated
new immunochemiluminometric assay, these data show
with a preliminary reagent lot. However, our results
that each PAC and PRC assay requires separate validationof cutoff values.
Evaluating diagnostic tests in a group of patients
Table 4. Proposed cutoff values for the PAC/PRC ratio
already known to have the disease and in a group of
with different units used in the literature.
healthy volunteers can lead to overestimation of diagnos-
tic accuracy (25 ). Thus, our data necessarily need to be
complemented by further studies in hypertensive cohorts,
e.g., in groups of patients with essential hypertension and
The clinical conditions necessary for testing of the
PAC/PRC or PAC/PRA ratios, such as discontinuing
Clinical Chemistry 50, No. 9, 2004
drug therapy, recording of dietary sodium intake, or time
8. Quinkler M, Lepenies J, Diederich S. Primary hyperaldosteronism.
of day for sampling, are not yet sufficiently standardized,
Exp Clin Endocrinol Diabetes 2002;110:263–71.
which contributes to the different published cutoff values
9. Montori VM, Young WF Jr. Use of plasma aldosterone concentra-
and complicates the use of the screening test in clinical
tion-to-plasma renin activity ratio as a screening test for primaryaldosteronism. A systematic review of the literature. Endocrinol
routine. An adequate standardization that meets general
Metab Clin North Am 2002;31:619 –32.
10. Oelkers W, Diederich S, Bahr V. Diagnosis and therapy surveil-
lance in Addison’s disease: rapid adrenocorticotropin (ACTH) test
In summary, our results suggest that the simultaneous
and measurement of plasma ACTH, renin activity, and aldoste-
measurement of PAC and PRC with automated immuno-
rone. J Clin Endocrinol Metab 1992;75:259 – 64.
chemiluminometric assays may be useful in screening for
11. Oelkers W, Diederich S, Bahr V. Primary hyperaldosteronism
PHA. Nevertheless, subsequent studies are required for
without suppressed renin due to secondary hypertensive kidneydamage. J Clin Endocrinol Metab 2000;85:3266 –70.
further comparison of the PAC/PRC ratio vs the PAC/
12. Young WF Jr. Primary aldosteronism: management issues. Ann
PRA ratio used for screening at present. These studies will
have to deal with the following questions: (a) Because we
13. Montori VM, Schwartz GL, Chapman AB, Boerwinkle E, Turner ST.
tested only for the differentiation of patients from normo-
Validity of the aldosterone-renin ratio used to screen for primary
tensive volunteers, has the PAC/PRC ratio similar sensi-
aldosteronism. Mayo Clin Proc 2001;76:877– 82.
tivities for screening of large hypertensive populations?
14. Schwartz GL, Chapman AB, Boerwinkle E, Kisabeth RM, Turner ST.
Prospective studies are needed. (b) Is the newly devel-
Screening for primary aldosteronism: implications of an increased
oped assay for PAC really a method that offers reliable
plasma aldosterone/renin ratio. Clin Chem 2002;48:1919 –23.
15. Tanabe A, Naruse M, Takagi S, Tsuchiya K, Imaki T, Takano K.
results if performed by different laboratories in clinical
Variability in the renin/aldosterone profile under random and
routine? (c) How is the PAC/PRC ratio influenced by
standardized sampling conditions in primary aldosteronism. J Clin
clinical conditions, especially drug effects? Regardless of
Endocrinol Metab 2003;88:2489 –94.
the answers to these questions, we expect that the new
16. Trenkel S, Seifarth C, Schobel H, Hahn EG, Hensen J. Ratio of
ratio method will evolve as a rapid and easily performed
serum aldosterone to plasma renin concentration in essential
hypertension and primary aldosteronism. Exp Clin EndocrinolDiabetes 2002;110:80 –5.
17. Ferrari P, Shaw SG, Nicod J, Saner E, Nussberger J. Active renin
versus plasma renin activity to define aldosterone-to-renin ratio for
We would like to acknowledge J. Wilde for statistical
primary aldosteronism. J Hypertens 2004;22:377– 81.
calculations and P. Exner, R. Go¨ber, K. Hanusa, and M.
18. De Bruin RA, Bouhuizen A, Diederich S, Perschel FH, Boomsma F,
Schro¨dter for excellent technical assistance.
Deinum J. Validation of a new rapid renin assay. Clin Chem;inpress.
19. Simon D, Hartmann DJ, Badouaille G, Caillot G, Guyenne TT,
1. Fardella CE, Mosso L, Gomez-Sanchez C, Cortes P, Soto J, Gomez
Corvol P, et al. Two-site direct immunoassay specific for active
L, et al. Primary hyperaldosteronism in essential hypertensives:
renin. Clin Chem 1992;38:1959 – 62.
prevalence, biochemical profile, and molecular biology. J Clin
20. Gallay BJ, Ahmad S, Xu L, Toivola B, Davidson RC. Screening for
primary aldosteronism without discontinuing hypertensive medi-
2. Loh KC, Koay ES, Khaw MC, Emmanuel SC, Young WF Jr.
cations: plasma aldosterone-renin ratio. Am J Kidney Dis 2001;
Prevalence of primary aldosteronism among Asian hypertensive
patients in Singapore. J Clin Endocrinol Metab 2000;85:2854 –9.
21. Seifarth C, Trenkel S, Schobel H, Hahn EG, Hensen J. Influence of
3. Calhoun DA, Nishizaka MK, Zaman MA, Thakkar RB, Weissmann
antihypertensive medication on aldosterone and renin concentra-
P. Hyperaldosteronism among black and white subjects with
tion in the differential diagnosis of essential hypertension and
resistant hypertension. Hypertension 2002;40:892– 6.
primary aldosteronism. Clin Endocrinol (Oxf) 2002;57:457– 65.
4. Mosso L, Carvajal C, Gonzalez A, Barraza A, Avila F, Montero J, et
22. Mulatero P, Rabbia F, Milan A, Paglieri C, Morello F, Chiandussi L,
al. Primary aldosteronism and hypertensive disease. Hypertension
et al. Drug effects on aldosterone/plasma renin activity ratio in
primary aldosteronism. Hypertension 2002;40:897–902.
5. Lim PO, MacDonald TM. Primary aldosteronism, diagnosed by the
23. Cartledge S, Lawson N. Aldosterone and renin measurements.
aldosterone to renin ratio, is a common cause of hypertension.
Clin Endocrinol (Oxf) 2003;59:427–30.
24. Morganti A, Pelizzola D, Mantero F, Gazzano G, Opocher G,
6. Stowasser M, Gordon RD, Gunasekera TG, Cowley DC, Ward G,
Piffanelli A, on behalf of the Italian Multicenter Study for Standard-
Archibald C, et al. High rate of detection of primary aldosteronism,
ization of Renin Measurement. Immunoradiometric versus enzy-
including surgically treatable forms, after ‘non-selective’ screening
matic renin assay: results of the Italian Multicenter Comparative
of hypertensive patients. J Hypertens 2003;21:2149 –57.
Study. J Hypertens 1995;13:19 –26.
7. Young WF Jr. Minireview: primary aldosteronism-changing con-
25. Lijmer JG, Mol BW, Heisterkamp S, Bonsel GJ, Prins MH, van der
cepts in diagnosis and treatment. Endocrinology 2003;144:
Meulen JHP, et al. Empirical evidence of design-related bias in
studies of diagnostic tests. JAMA 1999;282:1061– 6.
MEDICAL INFORMATION FORM Emergency Contact Information In case of a medical emergency, the ACU Champions Sports Camps staff will contact the Emergency Contact(s) you designate below First Contact Name ____________________________________________ Relationship _________________ Home Phone ___________________ Cell Phone ___________________ Work Phone __________________ Address ___
LITHIUM ION BATTERIES: INDIVIDUAL DATA SHEET CGR17500 CGR17500: Cylindrical Model Discharge Characteristics Charge Conditions: Constant voltage/constant current, 4.2 V, 550 mA (max.), 2 hours, 20˚C. Discharge Conditions: Constant current up to 3.0V at 20˚C. Charge Conditions: Constant voltage/constant current, 4.2 V, 550 mA (max.), 2 hours, 20˚C. Discharge Conditions: Con
 Clinical Chemistry 50, No. 9, 2004
Fig. 1. PAC, PRA, PRC, and the resulting PAC/PRA and PAC/PRC ratios for 76 healthy volunteers and 28 patients with PHA.
Clinical Chemistry 50, No. 9, 2004
Fig. 1. PAC, PRA, PRC, and the resulting PAC/PRA and PAC/PRC ratios for 76 healthy volunteers and 28 patients with PHA.