Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
Impact of depression on treatment effectiveness and gains maintenance in social phobia: a naturalistic study of cognitive behavior group therapy
EFFECTIVENESS AND GAINS MAINTENANCE IN SOCIAL
PHOBIA: A NATURALISTIC STUDY OF COGNITIVE
Sofi Marom, Ph.D.,1Ã Eva Gilboa-Schechtman, Ph.D.,2 Idan M. Aderka, M.A.,2 Abraham Weizman, M.D.,1
Background: The impact of depression on cognitive behavioral group therapy(CBGT) for social phobia (SP) in a naturalistic outpatient setting was examinedafter treatment termination and at 1-year follow-up. Methods: Consecutive SPoutpatients (N 5 219) were diagnosed using a structured interview. CBGT wasprovided in 18 1.5-hr weekly sessions. At pretreatment and posttreatmentquestionnaires and clinician ratings were administered. Self-report measureswere obtained at 1-year follow-up. The main outcome measure was the LiebowitzSocial Anxiety Scale. Results: CBGT was found to be effective in reducing bothsocial anxiety (effect size 5 1.23) as well as depression (effect size 5 0.94). Individuals with generalized social phobia (GSP) and individuals with specificsocial phobia (SSP) differed in their presenting psychopathology and in theirresponse to CBGT. Among treatment completers, 44% GSPs and 37% SSPsachieved at least 50% improvement, and 44% GSPs and 87% SSPs reporteddistress and functioning within the normal range at the end of treatment. AmongSPs diagnosed with major depressive disorder (MDD) at the onset of treatment,SP symptoms aggravated during the follow-up period, whereas SPs not diagnosedwith MDD experienced a further alleviation of SP symptoms during follow-up. CBGT provided in a public clinic to non-selected, mostly unmedicated andcomorbid patients, is an effective treatment for the majority of SP sufferers. Conclusions: MDD at the onset of CBGT was not associated with poorertreatment response, but predicted exacerbation of SP symptoms followingtreatment termination. Depressed SPs may need additional intervention tomaintain CBGT gains. SSPs may benefit from less intensive CBGT than GSPs. Depression and Anxiety 0:1–12, 2009.
Key words: social phobia; cognitive behavioral therapy; depression;co-morbidity; treatment outcome
ÃCorrespondence to: Sofi Marom Ph.D., Anxiety Disorders andBehavior Therapy Unit, Outpatient Department, Geha MentalHealth Center, P.O. Box 102, Petah-Tikva 49100, Israel. E-mail: ehud@barak.net.il
Received for publication 4 February 2007; Revised 23 July 2007;
Anxiety Disorders and Behavior Therapy Unit, Outpatient
Department, Geha Mental Health Center, Tel-Aviv University,Tel-Aviv, Israel
2Psychology Department, Bar-Ilan University, Ramat-Gan,
Published online in Wiley InterScience (www.interscience.wiley.
treatment outcome for the former group.[17,18] Exam-
ining the differential response of GSPs and SSPs to
ocial phobia (SP) is the third most common
CBGT is the second goal of this study.
psychiatric disorder, with an estimated lifetime pre-
Using pretreatment level of depression to predict
valence rate of 7–13% in western countries.[1] SP
CBGT outcome resulted in inconclusive results. For
usually starts in childhood or adolescence and is
instance,[19] found that individuals with SP and
typically comorbid with other axis-I disorders, parti-
comorbid depression had more severe SP symptoms
cularly anxiety and mood disorders.[2,3] In the absence
than individuals with SP alone. However, the degrees
of treatment, SP is a chronic lifelong disorder with
of improvement and rates of improvement were similar
little spontaneous remission course.[4] The DSM-IV-
for both groups. This suggests that despite being a
TR[5] distinguishes between generalized social phobia
graver condition, comorbidity with depression does not
(GSP) and non-generalized or specific social phobia
affect the course of treatment or the response to
(SSP) subtypes. GSP is characterized by fear of
treatment. In a similar vain,[20] concluded that depres-
multiple social situations, whereas SSPs fears are
sion has no detrimental effect on treatment or
circumscribed to a small number of situations.
improvement during treatment of SP. In contrast,
Randomized controlled trials have repeatedly de-
other studies found that depression was related to
monstrated that SP can be successfully treated with
dropping out during treatment and to diminished
either pharmachotherapy or cognitive behavioral ther-
improvement during treatment.[15, 21] and [22] also
apy [CBT].[6,7] One of the most widely studied variants
found higher levels of depression to be predictive of
of CBT—group CBT (CBGT)—has received robust
diminished gains at outcome. Importantly, no study has
empirical support.[8–10] In spite of the well-established
yet examined that patient characteristics predict the
therapeutic effects of CBGT in SP, no single study
maintenance of treatment gains. The examination of
examined these effects in a naturalistic setting, with a
the effects of depression at the onset of CBGT on both
large sample size and an extended follow-up.[11]
treatment outcome and treatment gains maintenance is
conducted a treatment outcome study in SP using a
large (n 5 387) sample, and so did[12] (n 5 295). However, both studies were randomized double-blindplacebo-controlled trials, by which the virtue of their
design limit the generalization of their findings tonaturalistic settings. In addition, the lack of follow-up
assessments in the Davidson et al.’s[12] study precludes
Upon contacting the outpatient clinic (T0), patients were
any conclusions regarding gains maintenance. Other
interviewed using the Mini International Neuropsychiatric Inter-
studies investigated the treatment of SP in more
view.[23] The data concerning all participants were gathered as a part
naturalistic settings. For instance,[13] compared treat-
of routine clinical practice and were used for the purpose of this study
ment of SP in a research unit with the same treatment
(the procedure was approved by the Institutional Review Board of theGeha Mental Health Center).
in an independent private practice and found no
The interval between the intake (T0) and the first treatment
differences in outcome between the settings. However,
session (T1) averaged 4.8 months (SD 5 1.2). CBGT was conducted
this study included a moderate sample size (50–60 per
by a Ph.D.-level clinical psychologist and a co-therapist (a psychiatry/
condition) and follow-up was conducted only 3 months
psychology resident). There were 18 weekly sessions of 1.5-hr
after termination of treatment. Another important
duration. The treatment protocol was based on the protocols of [24]
naturalistic study was conducted by,[14] who examined
and the theoretical writings of [25] The protocol included (a)
217 participants undergoing treatment in naturalistic
psychoeducation about SP; (b) exposure to feared social situations,
settings and reported results comparable to controlled
(c) reduction of safety behaviors, (d) cognitive restructuring, (e)
trials. However, patients were assessed only up to 6
instruction on external focus of attention, and (f) social skills training.
weeks after treatment termination. To sum, many
A typical session was divided into three parts: theoretical introduc-tion, in vivo exposure to feared social situations (e.g. reading in front
recent studies examined various aspects of the general-
of the group), and cognitive work. Homework was assigned weekly
izability and maintenance of CBGT, but none com-
and included in vivo exposure and self-administered cognitive
bined naturalistic setting, large sample size, and
restructuring. Each member of the treatment group took part in
extended follow-up assessment. This combination is
three to six in-session exposure exercises during the course of the
entire treatment, involving situations that are commonly stressful to
The existing data are also limited with respect to
most individuals with SP. Weekly homework assignments typically
CBGT’s differential treatment effects for the two
included exposure corresponding to the participants’ unique fears.
subtypes of SP. GSPs begin treatment more impaired
Participants comprised 21 CBT groups. Number of participants per
than SSPs and some studies suggest that patients with
group ranged between six and 20 with a mean of 10.8 (SD 5 4.3).
SSP are more responsive to CBGT—than are GSPs,[15]
During the last session (T2) patients were assessed using the samemeasures as at intake.
whereas other studies found a similar degree of
Drop-out was defined as (a) a premature cessation of participating
improvement in the two groups.[16,17] Clearly, if GSPs
in CBGT, that is, nonparticipation in the last session or (b) absence
begin treatment more impaired than SSPs, similar
from six or more CBGT sessions. No additional sessions (i.e.
degree of improvement lead to a worse end-of-
‘‘booster sessions’’) were conducted after termination of CBGT.
Approximately, 1 year after termination (T3) all participants who
Both patient and clinician versions of the Clinical Global
completed CBGTreceived questionnaires by mail and were requested
Impressions-Improvement Scale [CGI-I][33] were administered at
T2 to assess participants’ improvement. The CGI-I is a single itemassessing the degree of change in a person’s distress, on a 7-pointscale, such that 1 represents the greatest improvement and 7
represents a significant worsening. The Clinical Global Impres-
Two hundred ninety-three consecutive outpatients seeking treat-
sions-Severity scale [CGI-S][33] was used at T1 and T2 to assess
ment for SP at an anxiety disorders clinic of a regional mental health
participants’ global clinical condition. The CGI-S is a single
center in the greater Tel-Aviv area were assessed between 1998 and
item assessing severity of ‘‘illness’’ using a 7-point Likert scale
2002. The outpatient clinic provides treatment services free of charge.
ranging from ‘‘normal’’ to ‘‘very severely ill’’, and has good reliability
Participants were either self-referred or referred by a medical doctor
or mental health professional. Sixty-four individuals (22%) opted not
Depression was assessed by the Montgomery and Asberg Depres-
to participate in treatment. They cited interference with work/study,
sion Rating Scale [MADRS][35] at T1 and T2. The MADRS is a 10-
and/or participation in an active pharmacological or psychological
item scale in which each item is rated on a scale of 0 (no evidence of
treatment as their primary reasons for nonparticipation.
symptom) to 6 (pervasive evidence). The MADRS has good reliability
Inclusion criteria for study participation were: (a) a current
scores[36] and is sensitive to change during treatment.[35]
diagnosis of SP according to the DSM-IV; (b) a minimum ofa 1-year duration of SP; (c) primary diagnosis of SP, that is, in cases
with comorbidity, SP was deemed as the most distressing andclinically significant condition among the comorbid disorders; (d)
Descriptive analyses. Measures of a continuous nature
stable pharmacotherapy, that is, participants receiving a pharmaco-
were compared using independent t tests. Measures of categorical or
logical treatment who were taking a stable medication for at least 3
proportionate nature were compared between groups using w2 tests.
months before the beginning of CBGT; and (e) age between 18 and
Bonferroni correction was used when computing multiple compar-
60 years. Exclusion criteria were: (a) past or present diagnosis of
psychotic state and schizophrenia; (b) another psychotherapeutic
Efficacy analyses. We used multiple analysis of variance
treatment during CBGT, and (c) change in medication status during
(MANOVA) to check treatment efficacy. Dependant variables were
the CBGT. Ten individuals were excluded due to the above criteria.
the self-report measures used, and independent variables were Time
Thus, at the onset of treatment the sample included 219 individuals.
(i.e. before treatment, after treatment, and follow-up) and Subtype
It is important to note that none of the participants were excluded
(GSP versus SSP, or depressed versus nondepressed participants).
due to severity of SP. Moreover, participants were aware of group size
Multiple regression was used when predictors were continuous.
Diagnoses were determined by the Mini International Neuropsy-
chiatric Interview and were conducted by Ph.D.-level clinical
psychologists or experienced graduated psychology students trained
in their administration. The sub-diagnosis of GSP was based onDSM-IV criteria. Participants were diagnosed as suffering from GSP
Table 1 shows demographic, diagnostic, and
if they demonstrated fears and avoidance in most social situations. If
symptom severity levels for the complete sample. Out
participants demonstrated anxiety or avoidance pertaining to one
of the 219 participants at T1, 177 (80.8%) met
or two specific social situations (e.g. public speaking, eating in
diagnostic criteria for GSP and 42 (19.2%) met criteria
public), they were diagnosed as suffering from SSP.
for SSP. The majority of the sample (56.2%) received
A pilot study (n 5 20), conducted before the beginning of this
one or more additional DSM-IV diagnoses: 32.4%
study, examined the interviewers’ diagnostic validity and reliability bycomparing their diagnosis to those of a senior psychologist and a
suffered from exactly one additional anxiety disorder,
senior psychiatrist. The k coefficient was .92.
8.7% suffered from two or more additional anxietydisorders, 12.3% were diagnosed as having majordepressive disorder (MDD), and 11% were diagnosed
The main outcome measure used in this study was the Liebowitz
Pre-CBGT severity of SP, as measured by the LSAS,
Social Anxiety Scale [LSAS].[26] This study used the self-report
significantly correlated with pre-CBGT severity of
version of the LSAS, which has been shown to have high internal
depression as measured by the MADRS (r 5 0.40,
consistency, strong convergent, and discriminant validity, and high
Po0.001) and with the number of comorbid disorders
test–retest reliability.[27,28] The Hebrew version of the self-report
(r 5 0.18, Po0.01). Participants using psychotropic
LSAS has been validated in previous research.[29] Outcome was
drugs pre-CBGT and during CBGT (n 5 51) scored
measured by changes in LSAS scores between pretreatment (T1) and
significantly higher on the pre-CBGT LSAS compared
posttreatment (T2), and maintenance of gains was measured by
with non-medicated participants [81.1(22.6) versus
changes in LSAS scores between posttreatment (T2) and 1-year
68.6(23.6), respectively, t(203) 5 À3.32, Po0.01].
Changes in the degree of impairment in work, social, and family
areas were assessed using the Sheehan Disabilities Scale [SDS][30] at
T1, T2, and T3. The SDS evaluates the degree of impairment inwork, social, and family areas on a 10-point Likert scale. Reliability
Participants completed the LSAS twice before the
and construct validity of the SDS are high[31] and it has strong
beginning of treatment: at their initial interview (T0)
correlations with symptoms of social anxiety, depressive symptoms,
and at their first session (T1). The average waiting
and quality of life among individuals with SP.[32]
period for treatment was 4.8 months (SD 5 1.2). The
TABLE 1. Demographic, diagnostic, and illness severity characteristics of GSPs and SSPs pre-CBGT: percentageor mean (standard deviation)
an 5 165. bn 5 38. cRemains significant following Bonferroni correction. GSPs, generalized social phobics; SSPs, specific social phobics; SP, social phobia; CBGT, cognitive behavioral group treatment.
LSAS scores at the two time points were almost
elevated levels of depression compared with comple-
identical [70.5 (SD 5 24.1) and 70.4 (SD 5 20.0) for T0
ters. No significant differences were found on any
and T1, respectively] and the correlation between these
other demographic or clinical characteristics.
two pre-CBGT LSAS scores was highly significant(r 5 0.82, Po0.001). These results mirror earlierfindings implying that SP symptoms no not subsidein the absence of treatment:[29] found test–retest
reliability of the LSAS to be 0.87–0.91 over 7 weeks
Table 2 shows pre-CBGT, post-CBGT, and follow-
and[27] found it to be r 5 83, Po0.01 over a period of 3
up scores for GSPs and SSPs. To examine treatment
effectiveness in GSP and SSP, we conducted a 2(Time:pre-CBGT versus post-CBGT) Â 2(Subtype: GSP
versus SSP) MANOVAs with Time as a within-subjectfactor,and Subtype as a between subject factor.
The clinical characteristics of SSPs were significantly
Dependent variables were LSAS, SDS, MADRS, and
milder compared with GSPs (see Table 1). SSPs had a
later age of onset [t(201) 5 À5.60, Po0.001], and fewer
The main effect of Time was significant (Wilks’
comorbid diagnoses [w2(1) 5 5.20, Po0.05]. In addi-
l 5 0.36, Po0.001) indicating that post-CBGT scores
tion, a significantly higher percentage of SSP partici-
were significantly lower than pre-CBGT scores on all
pants were married [w2(1) 5 4.26, Po0.05]. SSPs
scored significantly lower than GSPs on all severity
Po0.001; SDS: F(1, 149) 5 171.6, Po0.001; MADRS;
measures: LSAS [t(148) 5 À19.55, Po0.01], SDS
[t(216) 5 À5.98, Po0.01], MADRS [t(216) 5 À5.02,
149) 5 203.8, Po0.001]. The effect size (ES; Cohen’s
Po0.01], and CGI-S [t(214) 5 À7.28, Po0.01].
d) of CBGT (on LSAS scores) was 1.23. A main effectfor Subtype was also found (Wilks’ l 5 0.64, Po0.001)
indicating that GSPs had higher scores than SSPs on
Fifty-six participants (25.6%) dropped out of treat-
all dependant variables [LSAS: F(1, 149) 5 82.7,
ment. More men dropped out of treatment compared
Po0.001; SDS: F(1, 149) 5 30.3, Po0.001; MADRS:
with women [w2(1) 5 4.57, Po0.05] and more medica-
F(1, 149) 5 13.3, Po0.001; CGI-S; F(1, 149) 5 33.8,
tion users dropped out of treatment compared with
Po0.001]. We also examined the possible effect of
nonmedication users [w2(1) 5 4.3, Po0.05]. It is
medication on treatment outcome. Medication use did
important to note that drop-outs did not differ from
not affect LSAS scores at T2 [t(164) 5 À1.48, P 5 0.14,
completers on MADRS scores [P40.05, ns (not
ns], nor did it affect improvement during treatment
significant)] indicating that drop-outs did not have
TABLE 2. Clinical measures among GSP and SSP completers of CBGT [presented as either means and (standarddeviations)/or percentages]
aNumber of cases varies due to missing data. GSPs, generalized social phobics; SSPs, specific social phobics; LSAS, Liebowitz Social Anxiety Scale; SDS, Sheehan Disabilities Scale; MADRS,Montgomery and Asberg Depression Rating Scale; CGI, Clinical Global Impression Severity of Illness; RCI, reliable change index. Good end-state, LSASo50 and SDSo3, and MADRSo8. See results for statistical analysis.
A significant Time  Subtype interaction was found
functioning compared to GSPs (79.3 versus 42.7%,
(Wilks’ l 5 0.86, Po0.001), but when further explored
w2(1) 5 11, Po0.001). As SSPs began treatment less
was found to be significant only on LSAS and MADRS
impaired than did GSPs, their absolute gains, although
scores [F(1, 217) 5 13.8, Po0.001; F(1, 217) 5 4.9,
smaller than those of GSPs, led to a better final good
Po0.05; for LSAS and MADRS, respectively]. On the
end-state. Importantly, no GSPs and 17.1% of SSPs fit
SDS and CGI-S no interaction was identified (both
the definition of good end-state functioning before
Fo1). The interaction on LSAS and MADRS scores
treatment (see Table 2). Even though 17.1% of SSPs
was such that GSPs exhibited greater reductions in SP
met requirements for good end-state before treatment,
and depressive symptoms compared to SSPs. The ESs
significantly more SSPs (79.3%) reached good end-
of CBGT (on LSAS scores) were 1.54 for GSPs and
1.16 for SSPs. The ESs of CBGT (on MADRS scores),
were 1.00 for GSPs, 0.64 for SSPs, and 0.94 for the
We used[41] reliable change index to assess recovery
and improvement in treatment based on means and
The majority of participants who completed treat-
standard deviations reported by.[28] According to
ment (63.2% of GSPs and 60.0% of SSPs) improved by
recommendations by,[41] we set the criterion for
at least 30% on the LSAS, and 43.6% of GSPs and
recovery to be two standard deviations above the mean
36.7% of SSPs improved at least by 50% on the LSAS.
of the functional population [LSAS scores lower than
Severity of SP as assessed by the LSAS at termination
38.9 indicated recovery, see].[28] Percentages of indivi-
of CBGT was aggravated in 6.4%, and in 6.6% of the
duals achieving improvement and recovery are re-
participants the improvement was o10%.
ported in Table 2 (for completer analysis) and in
Good end-state functioning was conceptualized as
Table 3 [for intent-to-treat (ITT) analysis].
return to nonpathological levels of distress[37] andoperationalized as LSAS o50, SDS o3 and MADRAS
o12. These three cutoff points were chosen because
they were found to be 1 SD above the average scores of
Of 163 CBGT completers, 95 (58.3%) completed
nonanxious and nondepressed individuals and therefore
1-year follow-up assessment. Table 2 presents data on
well within the normal range [for LSAS scores in Israel,
follow-up assessment for GSPs and SSPs.
see[38] for SDS scores,[39] for MADRS scores].[40]
To examine changes between termination (T2) and
According to this definition, at the end of CBGT,
follow-up (T3), we conducted a 2(Time: post- versus
significantly more SSPs reached good end-state
follow-up) Â 2(Subtype: GSP versus SSP) MANOVA
TABLE 3. Clinical measures of intent-to-treat sample using last-observation-carried-forward [presented as eithermeans and (standard deviations)/or percentages]
GSPs, generalized social phobics; SSPs, specific social phobics; LSAS, Liebowitz Social Anxiety Scale; SDS, Sheehan Disabilities Scale; MADRS,Montgomery and Asberg Depression Rating Scale; CGI, Clinical Global Impression Severity of Illness; RCI, reliable change index. Good end-state 5 LSASo50 and SDSo3, and MADRSo8. See results for statistical analysis.
As expected, GSPs had higher scores than SSPs onboth LSAS [F(1, 93) 5 15.6, Po0.001], and SDS [F(1,93) 5 8.2, Po0.01].
EFFECTS OF DEPRESSION ON TREATMENTOUTCOME AND GAINS MAINTENANCE
In our sample, 23 participants were diagnosed with
past MDD; 27 with current MDD; 24 with dysthymia;two were diagnosed as having both MDD (past orcurrent) and dysthymia. Both past MDD and dysthy-mia did not have significant effects on treatmentoutcome, on improvement during treatment, and ongains maintenance (all P 40.05).
Current MDD did not have a significant effect
on most treatment outcome measures. Specifically,SPs with current MDD did not differ from SPs with-
Figure 1. LSAS means for GSPs and SSPs. LSAS, Liebowitz
out current MDD on LSAS at T2 [t(164) 5 À1.59,
Social Anxiety Scale; GSP, generalized social phobia; SSP,
P 5 0.11, ns], or CGI-S at T2 [t(159) 5 À1.37,
specific social phobia; T1, pretreatment; T2, posttreatment;
P 5 0.17, ns]. However, SPs with current MDD
reported higher levels of impairment on the SDScompared
with Time as a within-subject factor, and Subtype as a
[t(163) 5 À2.36, Po0.05]. To further explore this
between-subject factor. Dependent variables were
difference, we examined the effect of current MDD
LSAS and SDS scores. Main effects for both Time
on each area of impairment included in the SDS. SPs
(Wilks’ l 5 0.93, Po0.05), and Subtype (Wilks’
with current MDD had greater impairments at work
l 5 0.86, Po0.01) were found suggesting a further
[F(1, 162) 5 7.17, Po0.01] compared with SPs without
decrease of SP severity. No significant Time  Subtype
current MDD, but no differences were found in the
interaction was found (Wilks’ l 5 0.98, P 5 0.461, ns).
social or family areas (both P40.05). In addition,
At T3, both LSAS and SDS scores were significantly
current MDD did not have an adverse effect on
lower than at T2 [F(1, 93) 5 5.0, Po0.05, F(1,
the improvement during treatment (pre-scores minus
93) 5 5.8, Po0.05, for LSAS and SDS, respectively],
post-scores) as measured by LSAS [t(164) 5 0.06,
indicating additional, albeit minor, improvement of
P 5 0.95, ns], SDS [t(162) 5 0.16, P 5 0.87, ns], or
symptoms following treatment termination (see Fig. 1).
CGI-S [t(159) 5 À0.52, P 5 0.61, ns]. As expected,
mentioned effects of current MDD are due to anycomorbidity, or due to its depression component per se,we examined whether comorbidity with anxiety dis-orders would generate the same pattern of results. Weused a 2(Time: post-tx versus follow-up)  2(AnxietyComorbidity: none versus comorbid anxiety) MANO-VA with Time as a within-subject factor, and AnxietyComorbidity as a between-subject factor. In addition,current MDD was a covariate. Dependent variableswere LSAS and SDS scores. Results indicated no maineffect for Anxiety Comorbidity and no Time  AnxietyComorbidity interaction (all P40.05). Anxiety Comor-bidity did not significantly affect maintenance of gains,as opposed to Current MDD.
When analyzed as a continuous variable using
Figure 2. LSAS means for participants with MDD and without
regression analysis, depression (but not SP symptoms)
MDD. LSAS, Liebowitz Social Anxiety Scale; History of
at the onset of treatment predicted exacerbation of SP
Depression, past or current MDD, major depressive disorder
at follow-up. Specifically, baseline MADRS scores
or dysthymia; T1, pretreatment; T2, posttreatment; T3 5 1-year
predicted SP symptom aggravation between posttreat-
ment and follow-up, whereas baseline LSAS scores didnot (MADRAS: T1-b 5 À0.23, Po0.05, but LSAS:T1-b 5 À0.15, P 5 0.17, ns).
current MDD had a positive effect on improvement ofdepressive
[t(151) 5 À3.34, Po0.01] (i.e. SPs with current MDD
Table 3 contains clinical measures for the intent-to-
showed more improvement in depressive symptoms
treat (ITT) sample using the last-observation-carried-
compared with SPs without current MDD).
forward procedure. We repeated the effectiveness
Next, we examined the effect of current MDD on
analyses and follow-up analyses using the ITT sample.
gains maintenance. A repeated measures MANOVA
Results were identical to those reported for the
with Time (post-tx vs. follow-up) as a within-subject
completer sample. However, in the ITT sample only
variable and Current MDD as between-subject variable
33.3% of GSPs and 26.2% of SSPs had more than 50%
revealed a significant Time  Current MDD interac-
decrease in LSAS scores at termination of treatment. At
tion (Wilks’ l 5 0.85, Po0.01), and a main effect for
follow-up 35.6% of GSPs and 47.6% of SSPs had more
Current MDD (Wilks’ l 5 0.88, Po0.01). The main
effect of Current MDD was found to be significant forboth LSAS [F(1, 93) 5 7.8, Po0.01] and SDS [F(1,93) 5 12.6, Po0.01] measures. As expected, SPs with
current MDD reported higher social anxiety and
This study investigated the impact of depression on
impairment compared with SPs without current MDD.
effectiveness of CBGT for SP in a large naturalistic
The Time  Current MDD interaction was found to
sample. Completers were also assessed 1 year after
be significant on both LSAS scores [F(1, 93) 5 14.9,
treatment termination and potential predictors of gains
Po0.001]; and on SDS scores [F(1, 93) 5 9.5, Po0.01]
separately. The interaction was such that on bothmeasures, the scores of SPs with current MDDsignificantly increased from termination to follow-up
[t(12) 5 À2.2, Po0.05], whereas SPs without current
MDD experienced a further alleviation of their
In a recent paper,[42] proposed and tested seven
symptoms [t(82) 5 3.4, Po0.01; Fig. 2].
criteria for distinguishing between efficacy (explana-
To check whether this effect of current MDD on
tory) studies and effectiveness (pragmatic) studies.
maintenance of gains was not due to current MDD
Efficacy studies are conducted in ideal conditions with
being correlated with comorbidity with other anxiety
high internal validity, whereas effectiveness studies are
disorders, we repeated the above analysis with anxiety
conducted under ‘‘real world’’ conditions emphasizing
comorbidity as a covariate. Results were identical in
external validity. The first criterion for an effectiveness
nature: a significant main effect for current MDD was
(naturalistic) study is treating or examining populations
found (Wilks’ l 5 0.87, Po0.01), and a significant
in primary clinical settings. As our clinic is located in a
Time  Current MDD interaction was found (Wilks’
primary clinical setting and offers treatment free of
l 5 0.85, Po0.01). The significant current MDD effect
charge, we believe the first criterion is satisfied. The
remained even after controlling for comorbidity of
second criterion is less stringent eligibility. In this
other anxiety disorders. To examine if the above-
study, only 10 individuals were excluded as a result of
our exclusion criteria. The inclusion/exclusion ratio
also mirror those reported by,[20] who found no
was 21.9, meaning that one person was excluded for
detrimental effects of depression on treatment outcome
every 22 that were included. This ratio is much higher
and on improvement during treatment. Again, con-
than in other studies (e.g. [43] with an inclusion/
sistent with our results,[20] also found that among
exclusion ratio of 2) and therefore fulfills the criterion
depressed individuals, depression declined during
of less stringent eligibility. Our study also fulfills the
treatment but remained elevated compared with non-
criterion of measuring health outcomes as the SDS and
depressed individuals. These results can be understood
CGI are used, and the criteria of long study duration,
when considering the interplay between anxiety and
adequate sample size, and ITT analysis. The only
depression during treatment of SP.[47] reported that
criterion that our study does not fulfill is the
during CBGT, changes in anxiety account for 91% of
measurement of adverse events during treatment. To
changes in depression, but changes in depression
sum, our study fulfils six out of seven criteria of
account for only 6% of changes in anxiety. These data
effectiveness studies and is much closer to the
suggest that depression reduction is primarily an
naturalistic prototype than to the randomized con-
outcome of social anxiety reduction among individuals
with SP, and that focally treating SP results in a
The mean LSAS score of our sample (70.5) was high,
or higher than the mean scores in clinical controlled
However, our results are at odds with several other
trials in the literature. For instance,[44] aggregated
studies investigating the interplay between depression
results from four clinical SP samples and found an
and social anxiety during treatment. For instance,[15]
average LSAS score of 67.2 before treatment. In
found that depression was a predictor of diminished
another study by[27], the average LSAS score among
improvement during treatment. A possible reason for
175 diagnosed but untreated participants was 69.1.
this discrepancy may be that the outcome measures
These data suggest that the present sample, which is
used by[15] were mainly self-reports of performance in
naturalistic in nature, is comparable to samples reported
behavioral tasks compared to questionnaires assessing
in clinical randomized studies in terms of SP severity.
both anxiety and avoidance used in this study. In arecent study,[21] found lower improvement rates fordepressed individuals. However, a diagnosis of MDD
was an exclusion criterion in the[21] study and may have
restricted the range of depressive symptoms examined.
The majority of SPs completing CBGT experienced
In our sample, the ES for anxiety was 1.54 for GSPs
a clinically significant improvement at the end of
and 1.16 for SSPs, and ESs for depression were 1.00 for
treatment, and these effects were maintained at 1-year
GSP and 0.64 for SSP. These ESs for SP symptoms
follow-up. In our naturalistic sample, participants
were somewhat larger than those reported in previous
improved irrespective of baseline severity of SP and
meta-analyses [0.80–0.90 in [48–50]]. Our ESs were also
irrespective of comorbidity of SP with other anxiety or
higher than those reported in naturalistic settings by[14]
mood disorders. Thus, even SPs with serious comor-
(0.71–0.88 for SP measures) and by[13] (1.0–1.2 for SP
bidity of anxiety and depression can markedly benefit
measures). When compared with other group treat-
from CBGT. It is important to note that our study
ments our ESs were also high [e.g. [51]—0.53–0.60 for
contained a naturalistic control condition. The waiting
SP measures, [52]—0.56 for SP measures]. However,
period for treatment averaged 18 weeks, a duration
our ESs were lower than those reported in recent
similar to the active treatment length. During this
controlled treatment outcome studies using individual
period, participants’ SP symptoms remained un-
format [e.g. 2.14 in[43] 2.63 in[45]].
changed. Thus, the improvement in treatment cannot
Despite these relatively large ESs, it is somewhat
sobering to realize that only about 50% GSPs
Although CBGT focally targeted social anxiety,
completing the treatment reached good end-state
participants exhibited a significant simultaneous de-
functioning. If we take into account the ITT sample,
crease in depressive symptoms at treatment termina-
this figure goes down to approximately 35%. This
tion. Several studies found a similar therapeutic effect
general pattern of considerable improvement during
e.g.[45,46] Namely, CBGT for SP resulted in improve-
treatment on one hand, and marked residual sympto-
ment in a wide range of distress symptoms. In addition,
matology on the other, has been found in previous
depressed individuals were identical to nondepressed
research[12]. When using reliable change index criter-
individuals at treatment completion on all measures but
ia[41] results were similar: 56% of completers achieved
one (higher impairment at work, as measured by a
significant improvement and 52% were categorized as
subscale of the SDS). In other words, depression did
recovered. When considering the ITT sample only
not have a detrimental effect on treatment outcome,
43% achieved significant improvement and 41% were
nor did it affect the degree of improvement during
categorized as recovered. These rates are very similar
treatment. These results are in line with,[19] who found
to the ones reported by[14] in a naturalistic setting: 56%
that comorbid depression does not result in differential
reliably improving and 57% categorized as recovered.
rates of improvement during CBGT of SP. Our results
Our rates of improvement are also slightly higher than
the ones reported by[51]: 36–44% of patients achieving
groups included 50–100% more participants than
reliable improvement on SP measures after group
groups in recent studies [e.g. [58]—6–8 participants;
treatment. Therefore, our results are comparable with
[51]—4–7 participants]. Perhaps, this may have caused
other naturalistic and group treatments.
participants to withdraw prematurely from CBGT. Third, our higher attrition rate may be due to a stricter
definition of dropping out (e.g. lack of participation inthe final session counted as a drop-out due to
Consistent with the literature, our data show that
procedural reasons). Fourth, ours was a naturalistic
GSP and SSP subgroups differed on most demographic
setting with a minimal exclusion rate and hence it
and on most psychopathology measures: GSPs had an
probably reflects a more realistic public outpatient–-
earlier age of onset; they presented graver indices of SP
and depression at pretreatment and posttreatment; and
Participants who dropped out of CBGT did not
had a higher prevalence of both anxiety and mood
differ from completers of CBGT on any demographic
disorders [for similar findings, see].[3,53] Taken to-
or clinical measure (including symptoms of SP and
gether, these findings are consistent with the notion
depression) except for a higher percentage of men and
that GSP and SSP are distinct nosological cate-
medication users among drop-outs. This indicates that
our sample of completers is likely to be representative
Although both GSP and SSP participants improved
of treatment seeking SPs. A similar conclusion was
significantly, a higher percentage of SSP participants,
reached by,[59] who compared drop-outs to treatment
compared with GSP participants, reported symptoms
completers in CBGT for SP and found only minor
in the nonclinical range at termination of CBGT. Put
differences between the two groups. They conclude
differently, although there was a substantial improve-
that it is unlikely that drop-outs pose a serious threat to
ment from pretreatment for the majority of partici-
external validity in CBGT for SP. Regrettably, the
pants, a large portion of GSPs retained residual
dropout participants in our sample were not assessed at
symptomatology that did not constitute a return to
the time of their early termination, so it is not clear
normal mental health and functioning. It is important
whether their dropping out was associated with an
to note that more GSPs (61.8%) improved compared
adequate improvement or aggravation of symptoms.
with SSPs (30.0%) but that less GSPs (44.1%) were
Obviously, more frequent assessments along the course
considered recovered compared to SSPs (86.7%). This
of CBGT would partially resolve this issue.
pattern of results is due to the fact that GSPs weremore impaired than SSPs at the onset of treatment. Many GSPs were able to achieve greater improvement
during treatment on the one hand but not sufficient
Sixty-three percent of completers of CBGT re-
improvement to be categorized as recovered on the
sponded to the follow-up questionnaires. No differ-
other. SSPs improved less but were closer to the
ences were detected between follow-up responders and
definition of recovery to begin with, and so achieved
nonresponders on any measure, rendering the respon-
recovery more easily. These findings suggest that GPSs
ders representative of CBGT completers. Many studies
may require more intensive, individual, and prolonged
have found that most participants extend treatment
interventions (either psychological and psychopharma-
gains over follow-up periods [e.g.].[45,51,57,60] In con-
cological) than do SSPs. However, SSPs might benefit
gruence with these studies, completers of our CBGT
from a concise group format, in which a more targeted,
maintained or improved the gains measured at
less extended, and hence less costly course of therapy is
termination of CBGT at a 1-year follow-up. The
maintenance and even augmentation of the treatmentresponse following CBGT represents an advantage
over pharmachotherapy to SP, which is associated with
The attrition rate in our study was somewhat higher
a significant likelihood of relapse when the drug is
than the average attrition reported in the literature
[25.6 versus 18.6% in a meta-analysis of 21 CBT
Our study is the first to examine the influence of
studies].[48] However, many nonnaturalistic studies
depression at intake on the maintenance of gains
report similar attrition rates [e.g. [55]—reporting a
during extended follow-up periods. Indeed, we found
22% attrition rate for an exposure condition;[56]—
that although depression did not affect the degree of
reporting a 31% attrition rate;[57]—reporting a 25%
improvement at CBGT termination, it significantly
attrition rate]. In this study, several factors might be
interfered with the maintenance of treatment gains. In
responsible for raising the attrition rate above the rate
fact, MDD was a better predictor of gains maintenance
common in controlled studies [yet maintaining it well
than comorbid anxiety or SP severity at intake. Several
within the attrition rates of naturalistic studies].[14]
mechanisms may be responsible for this pattern. First,
First, our relatively long CBGT course (18 sessions)
it is possible that the increase in social anxiety
might have increased the difficulty to complete
symptoms is due to the reoccurrence of another
treatment and thus increased attrition. Second, our
depressive episode in depression-prone participants.
The occurrence of a depressive episode is typically
Acknowledgments. The authors thank I. Gelern-
associated with an increase in social isolation, which in
ter M.A. and Prof. Y. Benjamini, from the Statistical
turn may increase symptoms of social anxiety. Second,
Laboratory, Sackler School of Mathematics, Tel Aviv
it may be that comorbid depression and SP represents a
University, for the statistical consultation, and Gadi
more severe type of mental disorder,[21] and therefore
Presburger, Ph.D., and Yael Vaknin, Ph.D., and Dan
individuals afflicted by it are more susceptible to full or
Raveh, Ph.D., for their help in data collection.
partial relapse. Indeed, individuals with comorbidMDD present a more severe clinical picture at the
onset of CBGT than do nondepressed individuals. Although depressed SPs may be capable of modifying
1. Furmark T. Social phobia: overview of community surveys. Acta
their social behavior and regulatory strategies while in
active CBGT, the presumed rigidity of their cognitive
2. Chartier MJ, Walker JR, Stein MB. Considering comorbidity in
schemas might interfere with the implementation of
social phobia. Soc Psychiatry Psychiatr Epidemiol 2003;
newly learned skills after termination.
3. Kessler RC, Stein MB, Berglund P. Social phobia subtypes in the
National Comorbidity Survey. Am J Psychiatry 1998;155:613–619.
4. deWit DJ, Ogborne A, Offord DR, MacDonald K. Antecedents
Our study suffered from several limitations. First,
of the risk of recovery from DSM-III-R social phobia. Psychol
treatment gains were not assessed blindly and were
American Psychiatric Association. Diagnostic and statistical
comprised of self-report measures and clinician ratings.
manual of mental disorders, Fourth Edition, Text Revision.
Self-report instruments may be susceptible to partici-
Washington, DC: American Psychiatric Association; 2000.
pants’ and clinicians’ expectations regarding improve-
6. Blanco C. Evidence-based pharmacotherapy of social anxiety
ment. Future studies should make use not only of self-
disorder. CNS Spectr 2005;10:10–11.
report and clinician ratings, but also of behavioral and
7. Radomsky AS, Otto MW. Cognitive behavioral therapy for social
implicit measures. Second, only data pertaining to
anxiety disorder. The Psychiatr Clin N Am 2001;24:805–815.
social anxiety and depression were collected. Our
8. Heimberg RG, Becker RE. Treatment of social fears and
knowledge of treatment outcome would be enhanced
phobias. New York: Guilford Press; 2002.
if additional parameters of psychological distress (e.g.
9. Hofmann SG, Bo¨gels SM. Recent advances in the treatment of
measures of anxiety) as well as broader measures of
social phobia: introduction to the special issue. J CognPsychother 2006;20:3–5.
interpersonal functioning (e.g. satisfaction with inter-
10. Turk CL, Heimberg RG, Hope DA. Social anxiety disorder. In:
personal relationships, cognitions, and attitudes per-
Barlow DH, editor. Clinical handbook of psychological dis-
taining to one’s social functioning) were assessed.
orders, 3rd ed. New York: The Guilford Press; 2001.
Third, in this study we lack the knowledge regarding
11. Blomhoff S, Haug TT, Helstro¨m K, Holme I, Humble M,
the main life events and (possibly) additional therapeu-
Madsbu HP, Wold JE. Randomized controlled general practice
tic interventions that may have occurred between
trial of sertraline, exposure therapy and combined treatment in
treatment termination and follow-up. Such data would
generalized social phobia. Br J Psychiatry 2001;179:23–30.
be important in furthering our understanding regard-
12. Davidson JR, Foa EB, Huppert JD, Keefe FJ, Franklin ME,
ing the factors contributing to changes in emotional
Compton JS, Zhao N, Connor KM, Lynch TR, Gadde KM.
distress following treatment termination.
Fluoxetine, comprehensive cognitive behavioral therapy, andplacebo in generalized social phobia. Arch Gen Psychiatry2004;61:1005–1013.
13. Gaston JE, Abbott MJ, Rapee RM, Neary SA. Do empirically
supported treatments generalize to private practice? A bench-
CBGTwas an effective treatment for chronic SP, and
mark study of a cognitive-behavioural group treatment pro-gramme for social phobia. Br J Clin Psychol 2006;45:33–48.
its therapeutic gains were maintained and even slightly
14. Lincoln TM, Rief W, Hahlweg K, Frank M, von Witzleben I,
improved at a 1-year follow-up. CBGTwas found to be
Schroeder B, Fiegenbaum W. Effectiveness of an empirically
effective in individuals with comorbid disorders. SSPs
supported treatment for social phobia in the field. Behav Res
present a more benign clinical picture than do GSPs on
most measures of psychopathology. More SSPs reached
15. Chambless DL, Tran GQ, Glass CR. Predictors of response to
good-end state functioning than GSPs. It appears that
cognitive-behavioral group therapy for social phobia. J Anxiety
SSPs could benefit from a shorter and more focused
CBGT. GSPs, in contrast, may need a longer course of
16. Hope DA, Herbert JD, White C. Diagnostic subtype,
CBGT, and smaller groups than ours, which could
avoidant personality disorder, and efficacy of cognitive behavioral
include additional components such as an individual
group therapy for social phobia. Cogn Ther Res 1995;19:399–417.
treatment or booster sessions. In addition, individuals
17. Turner SM, Beidel DC, Wolff PL, Spaulding S, Jacob RG.
suffering from both SP and depression experience an
Clinical features affecting treatment outcome in social phobia.
aggravation in SP symptoms after treatment termina-
tion, and may need follow-up treatment to prevent
18. Brown EJ, Heimberg RG, Juster HR. Social phobia subtype and
exacerbation of their symptoms at long term.
avoidant personality disorder: effect on severity of social phobia,
impairment, and outcome of cognitive-behavioral treatment.
37. Feeny NC, Zoellner LA, Foa EB. Treatment outcome for
chronic PTSD among female assault victims with borderline
19. Erwin BA, Heimberg RG, Juster H, Mindlin M. Comorbid
personality characteristics: a preliminary examination. J Personal
anxiety and mood disorders among persons with social anxiety
disorder. Behav Res Ther 2002;40:19–35.
38. Iancu I, Levin J, Hermesh H, Dannon P, Poreh A, Ben-Yehuda Y,
20. Joormann J, Kosfelder J, Schulte D. The impact of comorbidity
Kaplan Z, Marom S, Kotler M. Social phobia symptoms:
of depression on the course of anxiety treatments. Cogn Ther
prevalence, sociodemographic correlates, and overlap with
specific phobia symptoms. Compr Psychiatry 2006;47:399–405.
21. Ledley DR, Huppert JD, Foa EB, Davidson JRT, Keefe FJ, Potts
NLS. Impact of depressive symptoms on the treatment of
depressive disorders and their comorbidity: effect on central
nervous system noradrenergic function. Biol Psychichiatry 2004;
22. Scholing A, Emmelkamp PMG. Prediction of treatment out-
40. Von-Knorring AL, Olsson GI, Thomsen PH, Lemming OM,
come in social phobia: a replication. Behav Res Ther 1999;
Hulten A. A randomized, double-blind, placebo-controlled study
of citalopram in adolescents with major depressive disorder. J
23. Sheehan DV, Lecrubier Y, Sheehan KH, Amorim P, Janavs J,
Clin Psychopharmacol 2006;26:311–315.
Weiller E, Hergueta T, Baker R, Dunbar GC. The Mini
41. Jacobson NS, Truax P. Clinical significance: a statistical approach
International Neuropsychiatric Interview (M.I.N.I.): the devel-
to defining meaningful change in psychotherapy research. J
opment and validation of a structured diagnostic psychiatric
Consult Clin Psychol 1991;59:12–19.
interview for DSM-IV and ICD-10. J Clin Psychiatry 1998;
42. Gartlehner G, Hansen RA, Nissman D, Lohr KN, Carey KS. A
simple and valid tool distinguished efficacy from effectiveness
24. Heimberg RG, Juster HR, Hope DA, Mattia JI. Cognitive-
studies. J Clin Epidemiol 2006;59:1040–1048.
behavioral group treatment: description, case presentation, and
43. Clark DM, Ehlers A, McManus F, Hackmann A, Fennell M,
empirical support. In: Stein MB, editor. Social phobia: clinical
Campbell H, Flower T, Davenport C, Louis B. Cognitive
and research perspectives. Washington, DC: American Psychia-
therapy versus fluoxetine in generalized social phobia: a
randomized placebo-controlled trial. J Consult Clin Psychol
25. Clark DM, Wells A. A cognitive model of social phobia. In:
Heimberg RG, Liebowitz MR, Hope DA, Schneier FR, editors.
44. Heimberg RG, Horner HR, Juster SA, Safran SA, Brown FR,
Social phobia: diagnosis, assessment, and treatment. New York:
Liebowitz MR. Psychometric properties of the Liebowitz Social
Anxiety Scale. Psychol Med 1999;29:199–212.
26. Liebowitz MR. Social phobia. Mod Probl Pharmacopsychiatry
45. Clark DM, Ehlers A, Hackmann A, McManus F, Fennell M,
Grey N, Waddington L, Wild J. Cognitive therapy versus
27. Baker SL, Heinrichs N, Kim HJ, Hofmann SG. The Liebowitz
exposure and applied relaxation in social phobia: a randomized
Social Anxiety Scale as a self-report instrument: a preliminary
controlled trial. J Consult Clin Psychol 2006;74:568–578.
psychometric analysis. Behav Res Ther 2002;40:701–715.
46. Haug TT, Blomhoff S, Hellstrom K, Holme I, Humble M,
28. Fresco DM, Coles ME, Heimberg RG, Liebowitz MR, Hami S,
Madsbu HP, Wold JE. Exposure therapy and sertraline in social
Stein MB, Goetz D. The Liebowitz Social Anxiety Scale: a
phobia: 1-year follow-up of a randomized controlled trial. Br J
comparison of the psychometric properties of self-report and
47. Moscovitch DA, Hofmann SG, Suvak MK, In-Albon T.
Mediation of changes in anxiety and depression during treatment
29. Levin JB, Marom S, Gur S, Wechter D, Hermesh H.
Psychometric properties and three proposed subscales of a self-
of social phobia. J Consult Clin Psychol 2005;73:945–952.
report version of the Liebowitz Social Anxiety Scale translated
48. Federoff IC, Taylor S. Psychological and pharmacological
into Hebrew. Depress Anxiety 2002;16:143–151.
treatments for social phobia: a meta-analysis. J Clin Psycho-
30. Sheehan D. The anxiety disease. New York: Scribner; 1983.
31. Leon AC, Olfson M, Portera L, Farber L, Sheehan DV.
49. Feske U, Chambless DL. Cognitive behavioral versus exposure
Assessing psychiatric impairment in primary care with the
only treatment for social phobia: a meta-analysis. Behav Ther
Sheehan Disability Scale. Int J Psychiatry Med 1997;27:93–105.
32. Hambrick JP, Turk CL, Heimberg RG, Schneier FR, Liebowitz
50. Gould RA, Buckminster S, Pollack MH. Cognitive-behavioral
MR. Psychometric properties of disability measures among
and pharmacological treatment for social phobia: a meta-analysis.
patients with social anxiety disorder. J Anxiety Disord 2004;
Clin Psychol Sci Pract 1997;4:291–306.
51. Stangier U, Heidenreich T, Peitz M, Lauterbach W, Clark DM.
33. Guy W. ECDEU Assessment Manual for Psychopharmacology,
Cognitive therapy for social phobia: individual versus group
Revised. Rockville: US Dept of Health, Education and Welfare
therapy. Behav Res Ther 2003;41:991–1007.
52. Mo¨rtberg E, Karlsson A, Fyring C, Sundin O
34. Dahlke F, Lohaus A, Gutzmann H. Reliability and clinical
cognitive-behavioral group treatment (CBGT) of social phobia:
concepts underlying global judgments in dementia: implications
a randomized controlled study. J Anxiety Disord 2006;
for clinical research. Psychopharmacol Bull 1992;28:425–432.
35. Montgomery SA, Asberg MA. A new depression scale
53. Brown TA, Cambell LA, Lehman CL, Grisham GR, Mancill RB.
designed to be sensitive to change. Br J Psychiatry 1979;
Current and lifetime comorbidity of the DSM-IV anxiety and
mood disorders in a large clinical sample. J Abnorm Psychol
36. Davidson J, Turnbull CD, Strickland R, Miller R, Graves K. The
Montgomery-Asberg Depression Scale: reliability and validity.
54. Hook J, Valentiner D. Are specific and generalized social phobias
Acta Psychiatr Scand 1986;74:544–548.
qualitatively distinct? Clin Psychol Sci Pract 2002;9:379–395.
55. Smits JA, Powers MB, Buxkamper R, Telch MJ. The efficacy of
59. Hofmann SG, Suvak M. Treatment attrition during group
videotape feedback for enhancing the effects of exposure-based
therapy for social phobia. J Anxiety Disord 2006;20:961–972.
treatment for social anxiety disorder: a controlled investigation.
60. Liebowitz MR, Heimberg RG, Schneier FR, Hope DA, Davis S,
Holt CS, Goetz D, Juster HR, Lin SH, Bruch MA, Marshall RD,
56. Herbert JD, Gaudiano BA, Rheingold AA, Myers VH, Dalrym-
Klein DF. Cognitive-behavioral group therapy versus phenelzine
ple K, Nolan EM. Social skills training augments the effective-
in social phobia: long term outcome. Depress Anxiety
ness of cognitive behavioral group therapy for social anxiety
disorder. Behav Ther 2005;36:125–138.
61. Blanco C, Raza MS, Schneier FR, Liebowitz MR. The evidence-
57. Otto MW, Smiths JA, Reese HE. Cognitive-behavioral therapy
based pharmacological treatment of social anxiety disorder. Int J
for the treatment of anxiety disorders. J Clin Psychiatry
Clin Neuropsychopharmacol 2003;6:427–442.
62. Montgomery SA, Nil R, Du¨rr-Pal N, Loft H, Boulenger JP. A
58. Rosser S, Erskine A, Crino R. Pre-existing antidepressants
24-Week randomized, double-blind, placebo-controlled study of
and the outcome of group cognitive behaviour therapy for social
escitalopram for the prevention of generalized social anxiety
phobia. Aust N Z J Psychiatry 2004;38:233–239.
disorder. J Clin Psychiatry 2005;66:1270–1278.
VIII SEMANA C&T CEFET-MG/CÂMPUS DIVINÓPOLIS Data: 17 de Outubro de 2012 Horário: 13h00 às 21h00 APRESENTAÇÕES ORAIS Número de Inscrição - Título do Projeto Composição da Banca 007-Estimativa das forças/tensões atuantes entre garras de robôs manipuladores de precisão e peças sensíveis sendo 010-Estudo dos esforços na manipulação por robôs de pr
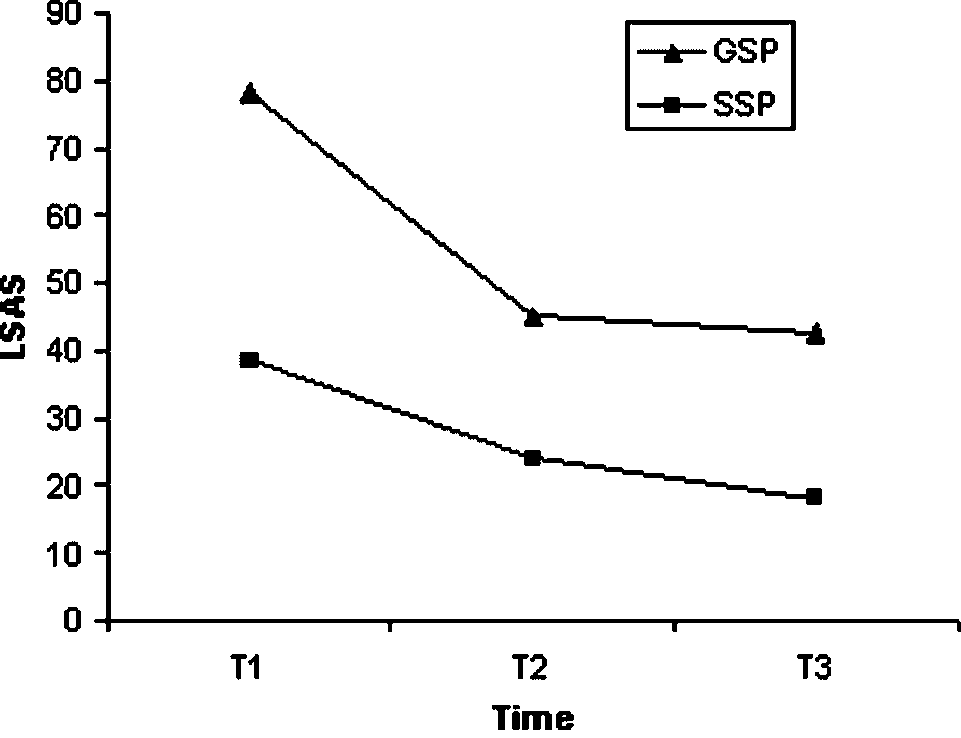 TABLE 3. Clinical measures of intent-to-treat sample using last-observation-carried-forward [presented as eithermeans and (standard deviations)/or percentages]
GSPs, generalized social phobics; SSPs, specific social phobics; LSAS, Liebowitz Social Anxiety Scale; SDS, Sheehan Disabilities Scale; MADRS,Montgomery and Asberg Depression Rating Scale; CGI, Clinical Global Impression Severity of Illness; RCI, reliable change index. Good end-state 5 LSASo50 and SDSo3, and MADRSo8.
TABLE 3. Clinical measures of intent-to-treat sample using last-observation-carried-forward [presented as eithermeans and (standard deviations)/or percentages]
GSPs, generalized social phobics; SSPs, specific social phobics; LSAS, Liebowitz Social Anxiety Scale; SDS, Sheehan Disabilities Scale; MADRS,Montgomery and Asberg Depression Rating Scale; CGI, Clinical Global Impression Severity of Illness; RCI, reliable change index. Good end-state 5 LSASo50 and SDSo3, and MADRSo8.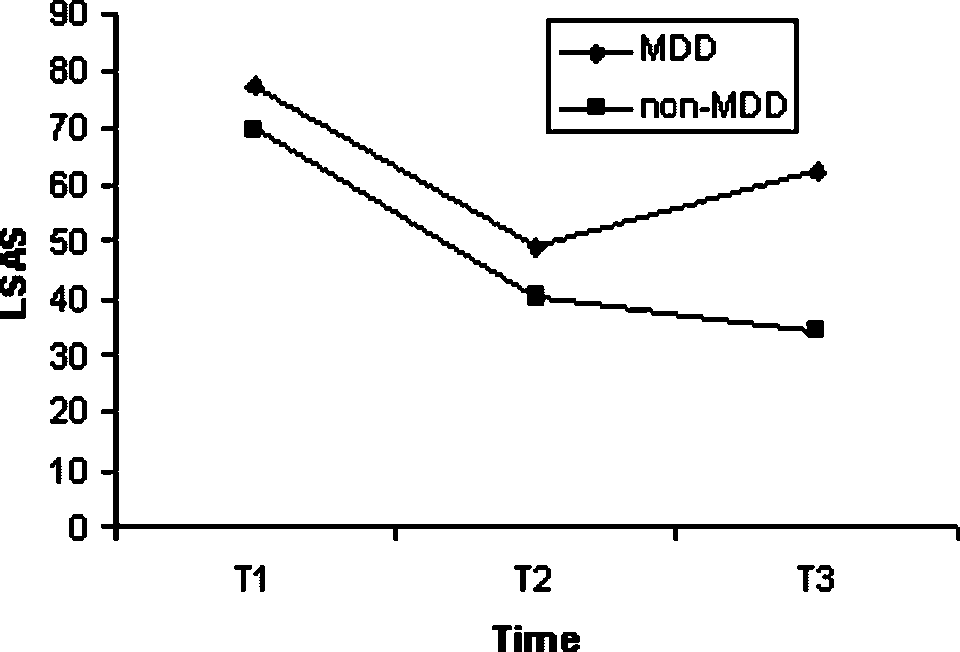 mentioned effects of current MDD are due to anycomorbidity, or due to its depression component per se,we examined whether comorbidity with anxiety dis-orders would generate the same pattern of results. Weused a 2(Time: post-tx versus follow-up)  2(AnxietyComorbidity: none versus comorbid anxiety) MANO-VA with Time as a within-subject factor, and AnxietyComorbidity as a between-subject factor. In addition,current MDD was a covariate. Dependent variableswere LSAS and SDS scores. Results indicated no maineffect for Anxiety Comorbidity and no Time  AnxietyComorbidity interaction (all P40.05). Anxiety Comor-bidity did not significantly affect maintenance of gains,as opposed to Current MDD.
mentioned effects of current MDD are due to anycomorbidity, or due to its depression component per se,we examined whether comorbidity with anxiety dis-orders would generate the same pattern of results. Weused a 2(Time: post-tx versus follow-up)  2(AnxietyComorbidity: none versus comorbid anxiety) MANO-VA with Time as a within-subject factor, and AnxietyComorbidity as a between-subject factor. In addition,current MDD was a covariate. Dependent variableswere LSAS and SDS scores. Results indicated no maineffect for Anxiety Comorbidity and no Time  AnxietyComorbidity interaction (all P40.05). Anxiety Comor-bidity did not significantly affect maintenance of gains,as opposed to Current MDD.