Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
New patient packet
SOUTHERN PAIN & ANESTHESIA CONSULTANTS
DATE: ________________ PATIENT NAME: _______________________________________________________ ADDRESS: _____________________________________________________________ CITY: _______________________ STATE:_________ ZIP CODE: _____________ HOME PHONE: ________________________ CELL PHONE:__________________ DATE OF BIRTH: ___________________________ AGE:______________________ SOCIAL SECURITY #: __________________________________________________ REFERRED BY: ________________________________________________________ EMPLOYER: _______________________________ PHONE:___________________ ADDRESS: _____________________________________________________________ CITY: ___________________________________ STATE: ______________________ RELATIVE OR FRIEND NOT RESIDING WITH YOU NAME: ____________________________________PHONE:____________________ ADDRESS: _____________________________________________________________ CITY: __________________________STATE: ____________ ZIP: _______________ WHO WILL BE RESPONSIBLE FOR PAYMENT? NAME: ______________________________PHONE: _________________________ ADDRESS: ____________________________________________________________ CITY:_________________________STATE: ____________ ZIP: _______________ IS THIS WORK RELATED? YES___________ NO_____________ Southern Pain and Anesthesia Consultants, LLC PAIN ASSESSMENT TOOL Today’s Date_________________________ Name_______________________________ Sex: Male / Female Date of Birth____________________ Age_______ Height _________ Weight __________ Referring Physician____________________________________________________________ Primary Care Physician________________________________________________________ Other Treating Physicians (i.e. Cardiologist)_______________________________________ Pain Problem / Reason for medical visit?__________________________________________ Other Medical Conditions (Past Medical History) ______________________________________________________________________________ ______________________________________________________________________________ ______________________________________________________________________________ __________________________________________________________________________ List all previous Surgeries (year and surgeon if known) ________________________________________________________________________ ______________________________________________________________________ _______________________________________________________________________ _______________________________________________________________________ Social History Occupation______________________________________________________________
Currently Working? (circle one) YES NO If NO, last date of work_______________
Disabled? When___________________ Why_________________________________
Do you Smoke? YES NO # of packs per day?________ # years a smoker?__________
Single / Married (#of years ______) / Divorced / Widow / # of Children______________
What is your highest level of education? _____________________________________
Do you use . . . marijuana / cocaine / heroin ?
Family History of…. (Circle all that apply)
Diabetes Cancer High Blood Pressure High Cholesterol Other______
Write a current list of all medications (dose and strength) including over-the- counter medications and the doctor who prescribes them. __________________________________________________________________ __________________________________________________________________ __________________________________________________________________ __________________________________________________________________ _______________________________________________________________________ Drug Allergies _____________________________________________________________________________ LOCATION Where is your pain located? ______________________________________________________________________________ ___________________________________________________________________________ Mark the exact location (s) of your pain on the following diagram How long have you experienced this pain? ______ Less than 6 months _____ 6 months to 1 year ______ 1-2 years
Other? ____________________________________________________________ Date that the pain first occurred? _____________________________________ Did any of the following cause your pain? (Check all that apply) ___________Automobile Accident ___________Work or Industrial Accident ___________Surgery
___________Being struck by an object ___________Other – explain:_________________________________________
If your pain is related to an accident, please indicate the . . .
Date of Injury __________________________
Place of Injury__________________________
Are you currently involved in litigation? (Is a lawyer involved because of the injury?)
Name of Attorney ______________________________________________
Address of Attorney_____________________________________________
_____________________________________________
Telephone of Attorney___________________________________________
______________________________________________
Does your pain prevent you from working? YES Are you currently off of work because of your pain problem?
If Yes, how long have you been off of work?____________________
Are you applying for or receiving any of the following benefits? CHOOSE THE FACE THAT BEST DESCRIBES HOW YOU FEEL Use the above scale to answer these questions: At present how would you rate your pain? ___________ The worst it gets is_____________ The best it gets is______________ How often do you experience your pain? (Please circle.) <25% of the time 50% of the time How do you describe your pain? (Circle all that apply.) Burning What activities cause or INCREASE the pain? (Circle all that apply) Laying
Physical Activities______________________________________________________ Job Activities__________________________________________________________ Other________________________________________________________________ Do any of the following help to RELIEVE your pain? (Circle all that apply) Laying
Other____________________________________________________ Have you tried any of the following to improve your pain problem? __________ Exercise Program
__________ Acupuncture/Acupressure __________ Chiropractic Treatment __________ Psychological evaluation __________ Nerve Blocks / Injections / Trigger points / Botox / Facet Injections Describe_________________________________________________ Do you experience any of the following items because of you pain?
(Check all that apply)
_____Increased temperature or warmth _____Decreased temperature or coolness _____Change in sweat pattern.
Has your pain affected any of the following? (Please circle)
How are you dealing with the pain? ________________________________________________________________________ ______________________________________________________________________ Do you ever think of hurting yourself? If so, what is your plan? _______________________________________________________________________ _______________________________________________________________________
When did you first see a medical professional for your current problem? Who have you seen?_______________________________________________________________ _______________________________________________________________________ Have you had any of the following tests? (Check all that apply) _____ X-rays
When__________Where______________________
When__________Where______________________
When__________Where______________________
_____Myelogram When__________Where______________________ _____Bone scan
When__________Where______________________
When__________Where______________________
Circle all medications that you have taken to try to improve your pain. Anti-inflammatory Medication: Tylenol (acetaminophen), Aleve (naprosyn), Daypro(oxaprozin),
Feldene, Lodine (etodolac), Voltaren, Ansaid, Relafen (nabumetone), Arthrotec, Vioxx,
Celebrex, Bextra, Mobic (meloxicam), Advil (ibuprofen), Motrin, Oruvail (ketoprofen), Indocin
(indomethacin), Feldene (piroxicam), Clinoril (sulindac), aspirin, Dolobid, Salsalate, diclofenac,
Antidepressant / Anti-anxiety Medication: Elavil (amitriptyline), Doxepin (sinequan), Pamelor
(nortriptyline), Effexor (venlafaxine), Paxil (paroxetine), Prozac (fluoxetine), Zoloft (sertraline),
Seroquel, BuSpar (Buspirone), Celexa(citalopram), Lexapro (escitalopram), Wellbutrin
(Bupropion), Cymbalta (duloxetine), Remeron (mirtazapine), Trazodone (Desyrel)
Migraine Medication: Imitrex, Axert, Relpax, Amerge, Maxalt, Zomig, Cafergot, Midrin,
Benzodiazepine Medication: Ativan (lorazepam), Valium (diazepam), Xanax (alprazolam)
Pain Medication: Lortab, Lorcet, Vicodin, Norco, Zydone, Percodan, Percocet, Oxycodone,
Roxicodone, Hydrocodone, Tramadol, Tylenol#3, Tylox, Darvocet(propoxyphene), Demerol,
Morphine, OxyContin, MS Contin, MSIR, Duragesic Patches(Fentanyl), Dilaudid, Kadian,,
Avinza, Methadone, Xodol, Tylenol #4, Actiq, Ultracet, Ultram, Opana, Fioricet, Fiorinal,
Muscle Relaxers: Soma (carisoprodol), Robaxin (methocarbamol), Flexeril (cyclobenzaprine),
Skelaxin, Zanaflex (tizanidine), Baclofen (lioresal), Dantrium(dantrolene), Parafon Forte
(chlorzoxazone), Norflex (orphenadrine), Valium (diazepam), Quinine
Neurontin (gabapentin), Topamax (topiramate), Gabitril,
Zonegran, Lamictal (lamotrigine), Tegretol, Dilantin, Lyrica
Sleep Aids: Ambien (zolpidem), Sonata, Lunesta, Rozeram, chloral hydrate, Restoril (temazepam)
Other Medications: _____________________________________________________________________________ Past Medical History Do you have or have you ever been diagnosed with any of the following Medical Conditions? (Circle all that apply)
Psychiatric Illness (i.e. Schizophrenia)
IBS (Irritable Bowel Syndrome) Crohn’s Disease
History Substance Abuse (marijuana, cocaine, etc.)
Cancer-Type / Year Diagnosed? __________________ (Radiation / Chemotherapy) Are you taking any blood thinners (Aspirin, Plavix, BC Powder, Etc.)? YES NO Goals for therapy ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ Comments ________________________________________________________________________ _______________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________
NOTICE OF PRIVACY PRACTICES (MEDICAL)
This notice describes how medical information about you may be used and disclosed and how you can get
access to this information. Please review it carefully.
The Health Insurance Portability Act of 1996 (“HIPAA”) is a federal program that requires that all
medical records and other individually identifiable health information used or disclosed by us in any form, whether electronically, on paper, or orally, are kept properly confidential. This Act gives you, the patient, significant new rights to understand and control how your health information is used. “HIPAA” provides penalties for covered entities that misuse personal health information.
As required by “HIPAA”, we have prepared this explanation of how we are required to maintain the
privacy of your health information and how we may use and disclose your health information. We may use and disclose your medical records only for each of the following purposes: treatment, payment and health care operations. • Treatment means providing, coordinating, or managing health care and related services by one or
more health care providers. An example of this would include a physical exam.
• Payment means such activities as obtaining reimbursement for services, confirming coverage, billing
or collection activities, and utilization review. An example of this would be sending a bill for your visit to your insurance company for payment.
• Health care operations include the business aspects of running our practice, such as conducting quality assessment and improvement activities, auditing functions, cost-management analysis, and customer service. An example would be an internal quality assessment review.
We may also create and distribute de-identified health information by removing all references to individually identifiable information.
We may contact you to provide appointment reminders or information about treatment alternatives or other health-related benefits and services that may be of interest to you.
Any other uses and disclosures will be made only with your written authorization. You may revoke such
authorization in writing and we are required to honor and abide by that written request, except to the extent that we have already taken actions relying on your authorization. You have the following rights with respect to your protected health information, which you can exercise
by presenting a written request to the Privacy Officer:
• The right to request restrictions on certain uses and disclosures of protected health information,
including those related to disclosures to family members, other relatives, close personal friends, or any other person identified by you.
We are, however, not required to agree to a requested restriction. If we do agree to a restriction, we
must abide by it unless you agree in writing to remove it.
• The right to reasonable requests to receive confidential communications of protected health information from us by alternative means or at alternative locations
• The right to inspect and copy your protected health information.
• The right to amend your protected health information.
• The right to receive an accounting of disclosures of protected health information.
• The right to obtain a paper copy of this notice from us upon request.
We are required by law to maintain the privacy of your protected health information and to provide you with notice of our legal duties and privacy practices with respect to protected health information.
This notice is effective as of April 15, 2003 and we are required to abide by the terms of the Notice of Privacy Practices currently in effect. We reserve the right to change the terms of our Notice of Privacy Practices and to make the new Notice provisions effective for all protected health information that we maintain. We will post and you may request a written copy of a revised Notice of Privacy Practices from this office.
You have recourse if you feel that your privacy protections have been violated. You have the right to file
a written complaint with our office, or with the Department of Health and Human Services, Office of Civil Rights, about violations of the provisions of this notice or the policies and procedures of our office. We will not retaliate against you for filing a complaint. Please contact us for more information: Southern Pain & Anesthesia Consultants, LLC Paul J. Hubbell, III, M.D. 2701 Lake Villa Dr. Ste. A Metairie, La 70002 118 Village Street Suite A Slidell, LA 70458 For more information about HIPAA or to file a complaint: The U.S. Department of Health and Human Services Office of Civil Rights 200 Independence Avenue, S.W. Washington, D.C. 20201 (202)619-0257 (877)696-6775
NOTICE OF PRIVACY PRACTICES ACKNOWLEDGEMENT
Southern Pain & Anesthesia Consultants, LLC
I understand that, under the Health Insurance Portability & Accountability Act of 1996 (“HIPAA”), I have certain rights to privacy regarding my protected health information. I understand that this information can and will be used to:
• Conduct, plan and direct my treatment and follow-up among the multiple health care providers who may be involved in that treatment directly and indirectly.
• Obtain payment from third-party payers. • Conduct normal health care operations such as quality assessments and physician certifications.
I have received, read and understand your Notice of Privacy Practices containing a more complete description of the uses and disclosures of my health information. I understand that this organization has the right to change its Notice of Privacy Practices from time to time and that I may contact this organization at any time at the address listed above to obtain a current copy of the Notice of Private Practices.
I understand that I may request in writing that you restrict how my private information is used or disclosed to carry out treatment, payment or health care operations. I also understand you are not required to agree to my requested restrictions, but if you do agree then you are bound to abide by such restrictions.
Patient Name: ____________________________________________________________________ Relationship to Patient: _________________________________________________________________ Signature:____________________________________________________________________________ Date:________________________________________________________________________________
I attempted to obtain the patient’s signature in acknowledgment on this Notice of Privacy Practices Acknowledgment, but was unable to do so as documented below: Date:
______________________________________________________________________
Initials: ______________________________________________________________________ Reason: ______________________________________________________________________
SOUTHERN PAIN & ANESTHESIA CONSULTANTS, LLC Paul J Hubbell, III, M.D. Edwin G. Hyde, M.D.
Metairie: 504-887-7207 Slidell : 985-643-4144 Fax: 504-889-1868
AUTHORIZATION FOR RELEASE OF CONFIDENTIAL INFORMATION I, ______________________________________ DOB:____/ ____/ ____HEREBY AUTHORIZE _______________________________________ADDRESS _____________________________ PH ____________________ FACILITY RELEASING RECORDS To Release to: Southern Pain & Anesthesia Consultants, LLC
THE INFORMATION INDICATED BELOW WITH REGARD TO SERVICES PROVIDED TO ME FOR THE FOLLOWING PURPOSE: __X__ FOR TREATMENT WITH DOCTOR __X__ FOR PROCESSING OF MY INSURANCE __X__ FOR APPLICATION FOR INSURANCE __X__ OTHER, SPECIFY: treatment at the hospital by any affiliates
REPORTS TO BE FURNISHED: ___Diagnosis (Also drug or alcohol abuse) ___ Consultations ___ Physicians Progress notes ___ Physician’s orders ___ H & P Exam reports ___ Lab & x-ray reports ___ Discharge Summary ___ Treatment Plan ___ Verbal Reports ___ Other : complete financial and billing records for each individual treating physician, as well for the facility and any affiliates.
1. This authorization shall expire 30 months from the date shown below, unless revoked sooner. 2. I may refuse to sign this authorization and it is strictly voluntary. 3. I have the right to revoke this authorization at any time. I understand that I must do so in writing and present the written revocation to the covered entity and Requestor. I understand that the revocation will not apply to information that has already been released to the authorization. 4. I have the right to receive a copy of this form after I sign it. 5. My treatment, payment, enrollment or eligibility for benefits may not be conditioned on signing this authorization. 6. The information used or disclosed pursuant to the authorization may be subject to redisclosure by the recipient and no longer protected.
Signature of Patient: _____________________________________________________ Date: ____/ ____/ ____ ______________________________________________________________________ Date: ____/ ____/ ____ Signature of Parent, Guardian or Legal Representative _________________________________________________ Nature of Relationship
Card Test INTENDED USE coated membrane and a pad containing the antibody-dyeThe One Step Cocaine/Benzoyl Ecgonine assay is a rapid,conjugate in a protein matrix containing a 0.1 % sodium azide. qualitative, competitive binding immunoassay for thedetermination of benzoyl ecgonine in human urine. The test MATERIALS REQUIRED, BUT NOT PROVIDED provides only preliminary data which sho
Patient Name: ________________________________________________________ NEW PATIENT MEDICAL HISTORY FORM -07/2010 Are you Right handed Left Handed both/ambidextrous Your family doctor is ___________________their office is in the city and state of ______________ What caused your pain? CAR ACCIDENT WORKERS COMP OTHER _______________ Please draw on the figure where the pain

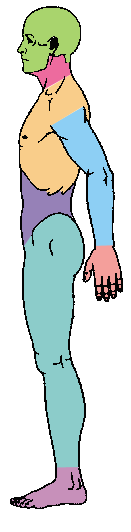
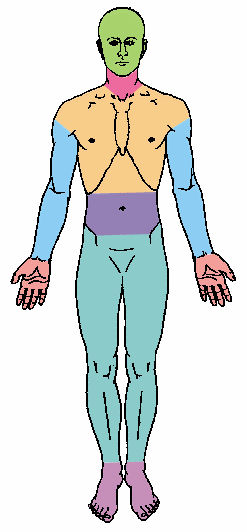
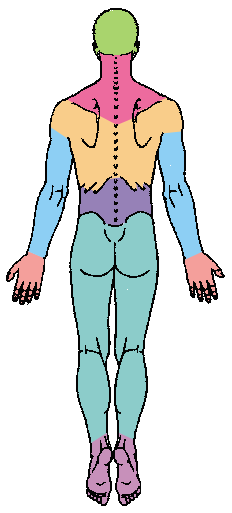 LOCATION
LOCATION 




