Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
Ocr document
Alzheimer's & Dementia 2 (2006) 314-321
Factors associated with use of medications with potential to impair
cognition or cholinesterase inhibitors among Alzheimer's
Edward D. Huey,*, Joy L. Taylor,C, Pauline Luu, John Oehlert, Jared R. Tinklenberg
"Cognitive Neuroscience Section, National Institute of Neurological disorders and Stroke, Building 10, Room 5C205, MSC 1440, National Institutes ~f bStanfordlVA Alzheimer's Center, Palo Alto, CA, USA cSierra-Pacific MIRECC, Palo Alto, CA, USA "Stanjord University Department of Psychiatry, Stanford, CA, USA
--------------------------------------------------------------
Background: The aim of this study was to use a signal detection method to examine the prevalence
of, and patient characteristics associated with, medication with potential to impair cognition and
cholinesterase inhibitor use in patients with Alzheimer's disease.
Methods: A cross-sectional study was conducted of 1,954 patients with a diagnosis of probable or
possible Alzheimer's disease. Concurrent medications were measured, specifically; (I) a medication
with potential to impair cognition or (2) a cholinesterase inhibitor. Predictor variables included age,
gender, ethnic group, education, age of symptom onset, number of prescriptions, number of medical
diagnoses, Mini-Mental State Examination (MMSE), Blessed-Roth Dementia Rating Scale
(BRDRS), probable versus possible AD diagnosis.
Results: Fifteen percent of the Alzheimer's disease patients were on a medication with potential to
impair cognition, and 44% were on a cholinesterase inhibitor. Patient characteristics associated with
the prescription of a medication with potential to impair cognition included total number of
prescription medications, low education, low MMSE, older age, reported lack of vitamin use, and
more medical diagnoses. Patient characteristics associated with the prescription of a cholinesterase
inhibitor included reported use of vitamins, the total number of prescription medications, fewer
medical diagnoses, lower age of symptom onset, and higher education.
Conclusions: Determining the patient characteristics associated with the prescription of a medi-
cation with potential to impair cognition can help clinicians identify patients who are at risk for
drug-related morbidity. Patient characteristics unassociated with dementia appear to influence the
prescription of cholinesterase inhibitors. Signal detection analysis is well suited to this type of
@ 2006 The Alzheimer's Association. All rights reserved.
Alzheimer's disease; inappropriate medications; cholinesterase inhibitors; Beers criteria; signal detection;
receiver operating characteristic analysis
total US population, they consume more than 25% of all
prescription medications and can have increased rates of
Inappropriate medication use, especially in the elderly,
adverse effects [I]. One of the challenges in this area has
has been a topic of increasing concern. Although older
been to develop criteria for inappropriate medication use.
AmLricans (aged 65 years and older) account for 13% of the
Although lists of potentially inappropriate medications can-
not capture all of the complex factors that are involved in
clinical decision making, they can be useful in gauging
potentially inappropriate medication use. The most studied
1552-5260/06/$ -see front matter 11) 2006 The Alzheimer's Association. All rights reserved
E. D. Huey et al. / Alzheimer's & Dementia 2 (2006) 314-321
of these is the Beers list of explicit criteria for inappropriate
Our second objective was to examine the prevalence of,
prescribing in older patients. These criteria, first published
and patient characteristics associated with, the prescription
in 1991 [2] and updated in 1997 [3] and 2003 [4] were
of cholinesterase inhibitors in AD patients. Few studies
originally developed for nursing home patients. However,
have examined the complex factors involved in the prescrip-
they have been used to evaluate patients in board and care
tion of a therapeutic agent. During the period of our anal-
facilities [5], outpatient settings [6,7], and home health care
ysis, cholinesterase inhibitors were prescribed increasingly.
settings [8] as well as nursing homes [9]. The criteria were
By identifying the patient variables associated with the
developed initially by Beers on the basis of a literature
prescription of a relatively new class of medications, we
review and evaluated by experts in geriatrics and pharma-
hoped to characterize patients who are most likely to receive
cology using a modified Delphi method [3]. The patient-
new treatments early. These patients provide an interesting
based prevalence of potentially inappropriate use of medi-
contrast to the patients prescribed a potentially inappropri-
cations found in these studies ranges from 14% to 40% with
ate medication identified in the first part of this study.
higher percentages generally observed in nursing homes and
Our third objective was to use an innovative signal de-
lower percentages seen in community samples [10,11], al-
tection method called a receiver operating characteristic
though 2 Canadian studies observed lower rates in nursing
curve (ROC) analysis to meet objectives 1 and 2 above.
homes than in the community [12,13]. One representative
study found that 21% of community-dwelling elderly pa-
tients received at least 1 potentially inappropriate medica-
2. Methods
tion [6]. A similar prevalence was found in a European
The 1,954 AD patients in this study were seen in 1 of 11
population [14]. The patient characteristics associated with
Alzheimer's Disease Research Centers or Alzheimer's Dis-
a higher risk of receiving Beers-criteria medications include
ease Centers of California. Patients were self-referred or
poor overall health [6,10-12], depression [14], polyphar-
refelTed by outside clinicians to one of these centers for
macy [6,10-12,14], and possibly female gender [6,10-12].
further evaluation of possible dementia and potential in-
Age has had mixed results as a predictive factor, with some
volvement in research projects. All patients who presented
studies reporting older patients to be at lower risk [12-14]
for their first evaluation at one of the sites between Decem-
and others at higher risk [10,15,16] of receiving a Beers-
ber 31, 1997 and December 31, 2001 and had an initial
consensus diagnosis of probable or possible AD by National
Psychotropic medications are the most commonly pre-
Institute of Neurological and Communicative Disorders and
scribed class of Beers-criteria medications in the elderly
Stroke and Alzheimer's Disease and Related Disorders As-
[13] (23%,44%, and 51% of potentially inappropriate med-
sociation criteria [18] were included in the study. The pa-
ications in long-term care, office-based settings and outpa-
tients' capacity to consent to this study was judged by a
tient departments, respectively) [15], with benzodiazepines,
multidisciplinary consensus panel. If a patient was judged to
amitriptyline, and propoxyphene being the most commonly
be incapable of providing informed consent, a surrogate
given medications with cognitive adverse effects
decision maker was evaluated, and if deemed appropriate
[10,11,16]. One study found that 33% of community-
and approved by the patient, assigned research durable
dwelling elderly who were taking psychotropic drugs re-
power of attorney duties. This project was reviewed and
ceived medications that were generally inappropriate [16].
approved by the appropriate institutional review boards.
Although these studies did not target demented patients,
The demographic characteristics of the subjects are pre-
they were part of the subject population in many of these
studies. One report assessed anticholenergic use and poten-
Data from the initial evaluation were used to diagnose
tial drug-drug interactions in demented and non demented
and determine the medications of the patient. Data were
populations [ 17]. In this study, we evaluate the amount of
retrieved from the Minimum Uniform Data Set (MUDS),
medication with potential to impair cognition use in de-
which is maintained by the Institute for Health and Aging
for the Alzheimer's Disease Research Centers of California.
We had 3 objectives for this study. The first was to
This data set includes the conculTent medications recorded
evaluate the use of a subset of Beers-criteria medications
at the time of the visit as well as other demographic and
that can interfere with cognition in patients with possible or
probable Alzheimer's disease (AD). The physicians in our
We were interested in the subset of the Beers criteria
research group reviewed the list of Beers-criteria medica-
medications with interference with cognition as a potential
tions and defined a subset of medications that can interfere
side effect. This included the majority of Beers-criteria
with cognition. We are interested in several questions: How
medications (15 of 25). The revised list from 1997 was
commonly are AD patients on potentially inappropriate
used, and only the medications deemed potentially inappro-
medications that can interfere with cognition? What patient
priate independent of diagnoses were used (Table 2).
characteristics CO1Tespond with the prescription of Beers-
The 1997, and not the 2003 criteria were used for several
criteria medications that can interfere with cognition?
reasons: The 2003 criteria were not published until after our
E.D Huey et al. / Alzheimer'.s & Dementia 2 (2006} 314-321
---------------------------------------------
On medication with potential to impair cognition
----------------------------------------------------------------------------------------------------------- ~
-----------------------------------------------------------------------------------------------------------
NOTE Numbers in parentheses are one standard deviation for reported means. Percentages in parentheses are percentages of patients with the charaeteristic
out of the total number of patients in each column. p value determined from univariate logistie regressions.
study was completed, the 2003 criteria rely more heavily
Type of medication used in patients taking a medication with potential
than the 1997 criteria on diagnosis-specific potentially in-
appropriate medications (which is not as well suited to the
analysis we used) and to facilitate comparison to the past
literature on this topic. In the Beers criteria, benzodiaz-
epines included individual medications as being potentially
inappropriate if they were above a certain dose. We did not
Methocarbamol (Roxabin), carisoprodol (Soma),
have records on specific doses of medications, so we were
unable to determine if patients were above a certain dose.
We also do not have information on as needed versus
scheduled use. However, we felt that benzodiazepines were
an important class of medications to analyze and so we
Amitriptyline (Elavil), chlordiazepoxide
amitriptyline (Limbitrol), and perphenazine
included these medications in our analyses irrespective of
The entire MUDS was reviewed, and variables that were
judged as clinically significant were included in the analy-
sis. These variables were age, gender, ethnic group, educa-
alprazolam (Xanax), temazepam (Restoril),
tion, age of symptom onset, number of prescriptions, num-
Chlordiazepoxide (Librium), chlordiazepoxide
ber of medical diagnoses, MMSE [19], BRDRS [20], and
probable versus possible AD diagnosis. Data from the initial
patient evaluation were used in the analysis.
Two families of multivariate statistical methods are used
Dicyclomine (Bentyl), hyoscyamine (Lev sin,
Levsinex), propantheline (Pro-Banthine),
commonly to identify subgroups of individuals at elevated
belladonna alkaloids Donnatal and others,
risk for a particular outcome. Linear models, including
logistic regression analysis, are most commonly used. The
Antihistamines including chlorpheniramine
other family, recursive partitioning, includes classification
and regression trees (CART), y automatic interaction de-
(Benadry1), hydroxyzine (Visaril, Atarax),
cyproheptadine (Periactin), promethazine
tection, and signal detection methods [21] .In this study, we
chose to use a signal detection method, rather than logistic
regression analysis, for several reasons. First, although lo-
gistic regression analysis is preferred for the testing of a
priori hypotheses, signal detection techniques are designed
NOTE Because some patients were taking more than I medication with
for exploratory, hypothesis-generating studies such as this
potential to impair cognition, the total percentage sums to greater than 100%.
E'. D. Huey et al. / A Izheimer'.I. & Dementia 2 (2006} 314-321
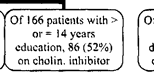
Of \ \ 38 patients on < 5 medications, 98 (9'/,)
Of 480 patients on > or = 5 medications, 90
Of 206 patients on < 9 medications, 55 (27%)
Of 130 patients on > or = 9 medications. 53
on med with potential to impair cognition
are on med with potential to impair cognition
(4 J %) are on med with potential to impair
Of 869 patients with MMSE Of 198 patients with MMSE
Fig I. ROC analysis of medications with potential to impair cognition.
one. The recursive partitioning process of signal detection
cance of p < 0.01, or the subgroup to be analyzed has 10 or
techniques automatically and systematically examines a se-
fewer subjects, or after the program has reached 3 levels of
ries of interactions [21] .In contrast, stepwise forward re-
analysis (i.e., creating a maximum of 8 subgroups). For
gression requires that the investigator enter alllower-order
continuous predictor variables (e.g., age), the procedure
interaction terms before considering higher-order interac-
calculates ROC curves first for the lowest value in the data
tions [21] .These explicit decisions can affect the magnitude
set, then for the lowest value plus 1, then plus 2, and so on,
of the estimated weights and thus the identified predictors
and ultimately selects the value with the best sensitivity and
[22]. Second, if there are reasons to believe that predictors
specificity. The ROC procedure can be set to differentially
are collinear (as in this study), signal detection may be
weight the analysis for sensitivity and specificity. Our anal-
preferred to logistic regression, because collinear predictors
yses were set to equally weigh sensitivity and specificity
can substantially bias the estimated weights for the predic-
thereby achieving both maximum sensitivity and maximum
tors in all-in logistic regression, independent of the actual
specificity. The ROC analysis software was developed at the
relationship between predictor and outcome [21,23,24].
Sierra-Pacific MIRECC at the Palo Alto Veterans Affairs
Third, in stepwise-forward logistic regression, the main
hospital. The program is public domain and may be ac-
effect terms making up an interaction must be entered be-
cessed at http://mirecc.stanford. edu.
fore the interaction term itself, which lowers statistical
power to detect interaction terms [21,25].
The specific signal detection analysis we used is called a
3. Results
"receiver operating characteristic curve (ROC) analysis"
because it calculates ROC curves to identify subgroups of a
3.1. Potentially inappropriate medication use
population at higher or lower risk for a dichotomous out-
come of interest (in our case, use of a potentially inappro-
In Fig. 1 at the top of the analysis, we can see that
priate medication and the use of a cholinesterase inhibitor)
overall, 15% of patients were prescribed a potentially inap-
propriate medication that could interfere with cognition.
Benzodiazepines were the most commonly prescribed class
We used an ROC analysis to identify patient character-
of medications. Looking at the first cutpoint in the ROC
istics associated with prescription of either a potentially
analysis, the number of prescriptions ("RxCount") ;::: or less
inappropriate medication or of a cholinesterase inhibitor.
than 7 medications best separates patients who are and are
The procedure constructs ROC curves for each potential
not prescribed a medication with potential to impair cogni-
predictor variable and determines which variable best sep-
tion (32% vs. 12%). After another split by number of pre-
arates the larger group into 2 subgroups with the greatest
scriptions, those patients with education less than 4 years or
purity of the dichotomous outcome of interest (i.e., the
patients with a MMSE score less than 12 were more likely
largest difference of prevalence) [21,23]. Each splitting
to receive a medication with potential to impair cognition.
variable must achieve a level of statistical significance of p
Taking the extreme categories from Fig. I, a patient on 7 or
< 0.01 or lower. After a split has been made, the program
8 medications and who had less than 4 years of education
repeats the analysis on each of the subgroups to further
was 10 times more likely to be on a medication with po-
divide the sample into subgroups having improved purity
tential to impair cognition as a patient on less than 5 med-
for the outcome of interest. The process repeats until the
ications with a MMSE score of 12 or greater (62% vs. 6%).
program can not identify a predictor that achieves signifi
The number of prescriptions was an important variable at
E.D. Huey et al / Alzheimer's & Dementia 2 (2006} 314-321
Of 1844 patients wilh age < 89,265 (14%)
Of 100 patienls with age > or = 89, 30
on med with potential to impair cognition
Of 1536 patients with MMSE > or = 10.204
on med with potcntial to impair cognition
Of 1393 patients with < 4 medical diagnoses,
Of 143 patients with > or = 4 medical
Of91 patientson>or= 1 vitamin. 1) (12%)
Of 106 paticnts on 0 vitamins, 31 (29%) on
175 (13%) on med with potential to impair
diagnoses, 29 (20%) on med with potential to
on med with potcntial to impair cognition
Fig 2. ROC analysis of medications with potential to impair cognition excluding number of prescriptions.
3.2. Cholinesterase inhibitor use
several steps in the analysis, as we expected based on the
results of previous studies and because our outcome vari-
able affects this variable. (Because we are looking at the
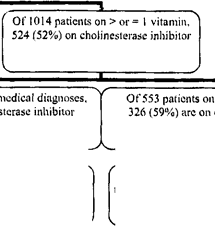
Forty-four percent of the patients were on a cholinester-
possibility of being prescribed a certain medication, being
ase inhibitor at the time of their initial evaluation (Fig. 3).
prescribed one of these medications will affect the total
The greatest predictor of whether a patient was on a cho-
number of prescriptions.) We therefore wanted to reanalyze
linesterase inhibitor was whether the patient was taking
the data without the influence of prescription number and so
vitamins. Vitamin takers were more likely to be prescribed
Fig. 2 is the same analysis as Fig. 1, excluding the number
a cholinesterase inhibitor. Total number of prescriptions
also predicted who was on a cholinesterase inhibitor. If we
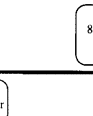
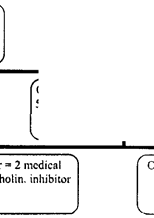
If we drop the number of prescriptions from the analysis
look at the ROC analysis without the inclusion of number of
(Fig. 2), age, with patient age greater than or equal to 89
prescriptions (Fig. 4), we see that additional predictors of
years, is the most predictive of which patients were more
being on a cholinesterase inhibitor are fewer medical diag-
likely to receive a medication with potential to impair cog-
noses, lower age of symptom onset, and education ~14
nition (30% vs. 14%). Among the patients less than 89
years. Looking at the most widely separated groups in Fig.
years, prescription of a medication with potential to impair
4, we see that a patient on vitamins, with fewer than 2
cognition was more likely if they had a MMSE score less
medical diagnoses and with symptom onset at less than 74
than 10 and were not taking vitamins. In patients with an
years old, was almost 3 times as likely to be on a cholines-
MMSE score ~ 10, ~4 medical diagnoses was associated
terase inhibitor than a patient not on vitamins, with less than
with prescription of a medication with potential to impair
14 years of education, with age of symptom onset at 80
Of 530 pnticnts OIJ > or ~ 4 medicat;Jns,
120 (29"10) on cholinc,tcrasc inhibitor
Fig 3. ROC analysis of cholinesterase inhibitor use.
E. D. Huey et al. / Alzheimer's & Dementia 2 (2006) 314--321
Of 553 patients with < 2 medical diagnoses.
education, 130 (43'Yo) on cb"lin inbibitor
Of 162 patients witb age at Of 410 patients with age at
Fig 4, ROC analysis of cholinesterase inhibitor use excluding number of prescriptions.
3.3. Variables chosen for analysis
several reasons: We were only looking at a subset of the
Beers criteria medications, dementia patients are hopefully
Univariate logistic regressions were performed on all of
less likely than non-demented patients to receive a medica-
the independent variables that we selected for our analysis
tion that may interfere with cognition, and the patient pop-
(Table 1). With the exception of one split on the basis of
ulation we analyzed is a research population that is likely
vitamin use at the third level of analysis of Fig. 2, all of the
highly motivated and more closely monitored compared to
independent variables identified in the ROC analysis were
the general population. However, as previously noted, a
significant in univariate logistic regressions. Note that this
significant proportion of subjects in previous studies on this
minor discrepancy does not mean that the ROC analysis was
topic suffered from dementia. We were unable to remove
incorrect in this instance. Within the subgroup defined by
low dose benzodiazepines from our analysis as specified in
the previous 2 splits, and removing the effect of number of
the Beers criteria [3], and so 15 % may be an overestima-
prescriptions, the third level split on the basis of vitamin use
tion, especially since benzodiazepines were the most com-
in Fig. 2 was statistically significant at p < 0.0 1 in the ROC
monly prescribed class of Beers criteria medications in our
sample. This is a serious limitation as benzodiazepines were
the largest category of medications with potential to impair
cognition prescribed. 7% of the patients were on both a
To test whether assessment center had an effect on our
medication with potential to impair cognition and a cho-
outcomes of interest, we reperformed with ROC analyses
linesterase inhibitor. Note that we use the term "potential to
discussed above with the inclusion of assessment center as
impair cognition." The Beers criteria are guidelines and
a variable. There were no differences on the 2 analyses on
there may be instances where the best choice for an indi-
prescription of a medication with potential to impair cog-
vidual patient is a Beers criteria "potentially inappropriate"
nition (Figs. I and 2) in the reanalysis. There was an effect
of center on cholinesterase inhibitor use, but the effect was
Our results agree with previous studies that the strongest
minor (at the third and final split level of the analysis).
single predictor for a patient being on a medication with
Patients not on vitamins with 4 or more prescriptions were
potential to impair cognition is being on a high number of
more likely to be on a cholinesterase inhibitor if they were
medications. Being on 7 or more medications almost tripled
seen at the Martinez, Caljfornia sjte. Patients not on vita-
mins who had less than 14 years of education were more
a patient's chance of being on a medication with potential to
likely to be on a cholinesterase inhibitor if they were seen at
impair cognition. Our results also support previous papers
the Martinez, California site. Otherwise, the analyses with
that have reported older age and more medical diagnoses as
and without assessment center were identical.
significant predictors of being on a medication with poten-
tial to impair cognition. Lower education and lower MMSE
have not been as consistently reported. It appears that older,
4. Discussion
sicker, less-educated dementia patients are at particular risk
for receiving a medication that can impair cognition. Not
Overall, 15% of patients were prescribed a potentially
taking vitamins is also a predictor of being on a medication
inappropriate medication that could interfere wjth cogni-
with potential to impair cognition. This has not, to our
tion. This is on the low end of the range reported in previous
knowledge, been reported. This information could help cli-
studies of outpatient and nursing home elderly (14% to
nicians involved in quality improvement projects. For ex-
40%) [10,11]. However, we would expect the number found
ample, if a pharmacy wanted to assess whether patients with
in our study to be lower than that of previous studies for
E.D. Huey et ul. / Alzheimer.s & Dementia 2 (2006) 314-.'121
dementia are on medications with potential to impair cog-
cation use were the opposite of those associated with cho-
nition, they could prioritize resources to patients identified
linesterase inhibitor use. The research on this topic demon-
in this study at particularly high risk for being on such a
strates the complexity of medical care delivery to the
elderly, the continuing need for highly trained prescribing
The patient characteristics that predicted cholinesterase
physicians, and the need to develop new statistical methods
inhibitor treatment are quite different than those that pre-
to investigate the complex factors that influence medication
dicted medication with potential to impair cognition use.
Taking vitamins was the single best predictor of a patient
taking a cholinesterase inhibitor. Other predictors included
fewer medical diagnoses, earlier symptom onset, and higher
Acknowledgment
education. These characteristics are likely markers for
healthier, health-literate patients who may be more likely to
The authors thank Helena C KI-aemer for statistical con-
request a new medication from their physician. The process
sultation, Art Noda for his assistance with the ROC analy-
of the prescription of therapeutic medications is an under-
sis, Elizabeth C. Lindenberger for her assistance with manu-
script preparation, the investigators at the Alzheimer's
Overall, 44% of our patients were taking a cholinest-
Disease Research Centers of California, the staff at the
erase inhibitor. This is, however, a group of dementia
StanfordN A Alzheimer's Center, and all of the patients and
patients referred to a research clinic during the years
their families who were involved in this study.
1998 to 200 1 , and as such it represents a particular group
This project was funded by the State of California DHS
of patients during a specific period. Preceding and during
Alzheimer's Disease Program, Grant Agreement No. 03-
this period, more cholinesterase inhibitors were made
75273; NIA-AG 17824; and the Sierra-Pacific Mental Il1ness
available (tacrine in 1993, donepezil in 1996, rivastig-
Research, Education and Clinical Center (MlRECC). Work
mine in 2000, and galantamine in 2001 ), and the pre-
was performed at the Palo Alto, California Veteran's Affairs
scription of this class of medications gained acceptance
in the medical community. We do not know how many
patients during this period were on cholinesterase inhib-
itors in a general community sample or how the prescrip-
References
tion rates have changed since then. Also, these results
were obtained on a specific population and may not be
generalizable to other populations. Another limitation of
[II Golden AG, Preston RA, Barnett SD, LJorente M, Hamdan K, Sil-
verman MA. Inappropriate medication prescribing in homebound
our study is, because it is cross-sectional, we can note
older adults. J Am Geriatr Soc 1999;47(8):948-53.
associations, but we cannot assign causality. For exam-
[2] Beers MH, Ouslander JG, Rollingher I, Reuben DB, Brooks J, Beck
ple, low MMSE score could increase the chance of being
JC. Explicit criteria for determining inappropriate medication use in
prescribed a potentially inappropriate medication or it
nursing home residents. UCLA Division of Geriatric Medicine, Arch
could be the result of the administration of a medication
[3) Beers MH. Explicit criteria for determining potentially inappropriate
that interferes with cognition. Also, we do not know the
medication use by the elderly. An update. Arch Intern Med 1997;
temporal relationship of when medications were prescribed.
Signal detection analysis is well suited to the questions
[4) Fick DM, Cooper JW, Wade WE, Waller JL, Maclean JR, Beers MH.
addressed in this study. It indicates not only which patient
Updating the Beers criteria for potentially inappropriate medication
characteristics are associated with the outcome of interest, it
use in older aduJts: results of a US eonsensus panel of experts. Arch
gives the cutpoints that maximally sepaI-ate the patients on
[51 Spore DL, Mor V, Larrat P, Hawes C, Hiris J. Inappropriate drug
the outcome of interest. It also indicates which patients are
prescriptions for elderly residents of board and care facilities. Am J
at high or low risk for an outcome within groups already
defined as high or low risk in previous levels of the analysis.
[6] Zhan C, Sangl J, Bierman AS, Miller MR, Friedman B, Wiekizer SW,
The resulting "tree" display is clinically relevant and easy to
et al PotentjaJly inappropriate medieation use in the community-
dwelling elderly: findings from the 1996 Medical Expenditure Panel
A significant number of our dementia patients were on a
[7] Stuck AE, Beers MH, Steiner A, Aronow HU, Rubenstein LZ, Beck
potentially inappropriate medication that could interfere
JC. Inappropriate mediclltion use in community-residing older per-
with cognition. These patients are likely to be at higher risk
sons. Arch Intern Med 1994;154(19)-2]95-200.
for adverse effects, as they tend to be on more medications,
[8) Meredith S, Feldman PH, Frey D, Hall K, Arnold K, Brown NJ, et al
Possible medication el,ors in home healthcare patiento. J Am Geriatr
tend to be older, and have more medical diagnoses. Cho-
linesterase inhibitor use was associated with patient charac-
[9] Beers MH, Ouslander JG, Fingold SF, Morgenstern H, Reuben DB,
teristics that are likely markers for patients who are more
Rogers W, et al Inappropriate medication pre5cribing in skilled-
likely to seek new treatments for a disorder. Many of the
nursing ti!cilitie.!;. Ann Intern Med 1992;117(8);684-9.
patient chaI.acteristics associated with inappropriate medi
[ 10] Aparasu RR. Mort JR Inappropriate prescribing for the elderly Beers
criteria-based review. Ann Pharmacother 2000;34(3):338-46.
E.D. Huey et a[ / Alzheimer's & Dementia 2 (2006) 314-321
[ II] Liu GO, Christensen OB. The continuing challenge of inappropriate
NINCDS-ADRDA Work Group under the auspices of Department of
prescribing in the elderly: an update of the evidence. J Am Pharm
Health and Human Services Task Force on Alzheimer's Disease.
[12] Lane CJ, Bronskill SE, Sykora K, Dhalla IA, Anderson OM, Mam-
[19] Folstein MF, Fo!stein SE, MeHugh PR. "Mini-mental state:' A prac-
dani MM, et al. Potentially inappropriate prescribing in Ontario
tical method for grading the cognitive !;tate of patients for the clini-
community-dwelling older adults and nursing home residents. J Am
cian. J Psychiatr Res 1975;]2(3):189-98.
[20] Blessed a, Tomlinson BE. Roth M. The association between quan-
[13] Dhalla IA, Anderson OM, Mamdani MM, Bronskill SE, Sykora K,
titative measures of dementia and of senile change in the cerebra]
Rochon PA. Inappropriate prescribing before and after nursing home
grey matter of elderly subjects. Br J Psychiatry 1968; 114(512)-797-
admission. J Am aeriatr Soc 2002;50(6);995-l000.
[14] Fialova D, Topinkova E, aambassi a, Finne-Soveri H, Jonsson PV,
[21] Kiernan M, Kraemer HC, Winkleby MA, King AC. Taylor CB. Do
Carpenter I, et al, Potentially inappropriate medication use among
logistic regression and signal detection identify different subgroups at
elderly home care patients in Europe. JAMA 2005;293(1 I): 1348-58.
risk? Implications for the design of tailored interventions Psychol
[15] Mort JR, Aparasu RR. Prescribing potentially inappropriate psycho-
tropic medications to the ambulatory elderly. Arch Intern Med 2000;
[22] Hosrner OW Jr, Lemeshow S. Applied logistic regression, New York.
[ 16] Aparasu RR, Mort JR. Prevalence, conelates, and associated outcomes
of potentially inappropriate psychotropic use in the con1lnunity-
[23] Kraemer H. Evaluating medical tests objective and quantitative
dwelling elderly. Am J aeriatr Pharmacother 2004;2(2):102-11
guidelines. Newbury Park, CA. Sage Publications, 1992
[17] airon MS, Wang HX, Bernsten C, Thorslund M. Winblad B, Fastbom
[24] Mcaee D, Reed D, Yano K. The results of logistic analyses when the
J. The appropriateness of drug use in an older nondemented and
variables are highly conelated. an empirical example using diet and
demented population. J Am aeriatr Soc 2001;49(3).277-83.
CHD incidence. J Chronic Dis 1984;37(9-10):713-9.
[] 8] McKIlann a, Drachman D, Folstein M, Katzman R, Price O, Stadlan
[25] Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed
EM. Clinieal diagnosis of Alzheimer's disease. report of the
E.D. Huey et a[ / Alzheimer's & Dementia 2 (2006) 314-321
[ II] Liu GO, Christensen OB. The continuing challenge of inappropriate
NINCDS-ADRDA Work Group under the auspices of Department of
prescribing in the elderly: an update of the evidence. J Am Pharm
Health and Human Services Task Force on Alzheimer's Disease.
[12] Lane CJ, Bronskill SE, Sykora K, Dhalla IA, Anderson OM, Mam-
[19] Folstein MF, Fo!stein SE, MeHugh PR. "Mini-mental state:' A prac-
dani MM, et al. Potentially inappropriate prescribing in Ontario
tical method for grading the cognitive !;tate of patients for the clini-
community-dwelling older adults and nursing home residents. J Am
cian. J Psychiatr Res 1975;]2(3):189-98.
[20] Blessed a, Tomlinson BE. Roth M. The association between quan-
[13] Dhalla IA, Anderson OM, Mamdani MM, Bronskill SE, Sykora K,
titative measures of dementia and of senile change in the cerebra]
Rochon PA. Inappropriate prescribing before and after nursing home
grey matter of elderly subjects. Br J Psychiatry 1968; 114(512)-797-
admission. J Am aeriatr Soc 2002;50(6);995-l000.
[14] Fialova D, Topinkova E, aambassi a, Finne-Soveri H, Jonsson PV,
[21] Kiernan M, Kraemer HC, Winkleby MA, King AC. Taylor CB. Do
Carpenter I, et al, Potentially inappropriate medication use among
logistic regression and signal detection identify different subgroups at
elderly home care patients in Europe. JAMA 2005;293(1 I): 1348-58.
risk? Implications for the design of tailored interventions Psychol
[15] Mort JR, Aparasu RR. Prescribing potentially inappropriate psycho-
tropic medications to the ambulatory elderly. Arch Intern Med 2000;
[22] Hosrner OW Jr, Lemeshow S. Applied logistic regression, New York.
[ 16] Aparasu RR, Mort JR. Prevalence, conelates, and associated outcomes
of potentially inappropriate psychotropic use in the con1lnunity-
[23] Kraemer H. Evaluating medical tests objective and quantitative
dwelling elderly. Am J aeriatr Pharmacother 2004;2(2):102-11
guidelines. Newbury Park, CA. Sage Publications, 1992
[17] airon MS, Wang HX, Bernsten C, Thorslund M. Winblad B, Fastbom
[24] Mcaee D, Reed D, Yano K. The results of logistic analyses when the
J. The appropriateness of drug use in an older nondemented and
variables are highly conelated. an empirical example using diet and
demented population. J Am aeriatr Soc 2001;49(3).277-83.
CHD incidence. J Chronic Dis 1984;37(9-10):713-9.
[] 8] McKIlann a, Drachman D, Folstein M, Katzman R, Price O, Stadlan
[25] Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed
EM. Clinieal diagnosis of Alzheimer's disease. report of the
The following is a list of the most commonly prescribed drugs. It represents an abbreviatedversion of the drug list (formulary) that is at the core of your prescription-drug benefit plan. The list is not all-inclusive and does not guarantee coverage. In addition to using this list,you are encouraged to ask your doctor to prescribe generic drugs whenever appropriate. PLEASE NOTE: The symbol * nex
P27 Post-partum haemorrhage admissions to critical care: completing the audit cycle A D Evans, L Rees, R E Collis Department ofAnaesthetics, University Hospital of Wales, Cardiff, UK Introduction: Post -partum haemorrhage (PPH) remains a common cause of obstetric admissions to critical care in the UK. Our audit (May 2004 association with carboprost (HaemobateTM) and pulmon
 Alzheimer's & Dementia 2 (2006) 314-321
Factors associated with use of medications with potential to impair
cognition or cholinesterase inhibitors among Alzheimer's
Edward D. Huey,*, Joy L. Taylor,C, Pauline Luu, John Oehlert, Jared R. Tinklenberg
"Cognitive Neuroscience Section, National Institute of Neurological disorders and Stroke, Building 10, Room 5C205, MSC 1440, National Institutes ~f
bStanfordlVA Alzheimer's Center, Palo Alto, CA, USA
cSierra-Pacific MIRECC, Palo Alto, CA, USA
"Stanjord University Department of Psychiatry, Stanford, CA, USA
--------------------------------------------------------------
Background: The aim of this study was to use a signal detection method to examine the prevalence
of, and patient characteristics associated with, medication with potential to impair cognition and
cholinesterase inhibitor use in patients with Alzheimer's disease.
Methods: A cross-sectional study was conducted of 1,954 patients with a diagnosis of probable or
possible Alzheimer's disease. Concurrent medications were measured, specifically; (I) a medication
with potential to impair cognition or (2) a cholinesterase inhibitor. Predictor variables included age,
gender, ethnic group, education, age of symptom onset, number of prescriptions, number of medical
diagnoses, Mini-Mental State Examination (MMSE), Blessed-Roth Dementia Rating Scale
(BRDRS), probable versus possible AD diagnosis.
Results: Fifteen percent of the Alzheimer's disease patients were on a medication with potential to
impair cognition, and 44% were on a cholinesterase inhibitor. Patient characteristics associated with
the prescription of a medication with potential to impair cognition included total number of
prescription medications, low education, low MMSE, older age, reported lack of vitamin use, and
more medical diagnoses. Patient characteristics associated with the prescription of a cholinesterase
inhibitor included reported use of vitamins, the total number of prescription medications, fewer
medical diagnoses, lower age of symptom onset, and higher education.
Conclusions: Determining the patient characteristics associated with the prescription of a medi-
cation with potential to impair cognition can help clinicians identify patients who are at risk for
drug-related morbidity. Patient characteristics unassociated with dementia appear to influence the
prescription of cholinesterase inhibitors. Signal detection analysis is well suited to this type of
@ 2006 The Alzheimer's Association. All rights reserved.
Alzheimer's disease; inappropriate medications; cholinesterase inhibitors; Beers criteria; signal detection;
receiver operating characteristic analysis
total US population, they consume more than 25% of all
prescription medications and can have increased rates of
Inappropriate medication use, especially in the elderly,
adverse effects [I]. One of the challenges in this area has
has been a topic of increasing concern. Although older
been to develop criteria for inappropriate medication use.
Alzheimer's & Dementia 2 (2006) 314-321
Factors associated with use of medications with potential to impair
cognition or cholinesterase inhibitors among Alzheimer's
Edward D. Huey,*, Joy L. Taylor,C, Pauline Luu, John Oehlert, Jared R. Tinklenberg
"Cognitive Neuroscience Section, National Institute of Neurological disorders and Stroke, Building 10, Room 5C205, MSC 1440, National Institutes ~f
bStanfordlVA Alzheimer's Center, Palo Alto, CA, USA
cSierra-Pacific MIRECC, Palo Alto, CA, USA
"Stanjord University Department of Psychiatry, Stanford, CA, USA
--------------------------------------------------------------
Background: The aim of this study was to use a signal detection method to examine the prevalence
of, and patient characteristics associated with, medication with potential to impair cognition and
cholinesterase inhibitor use in patients with Alzheimer's disease.
Methods: A cross-sectional study was conducted of 1,954 patients with a diagnosis of probable or
possible Alzheimer's disease. Concurrent medications were measured, specifically; (I) a medication
with potential to impair cognition or (2) a cholinesterase inhibitor. Predictor variables included age,
gender, ethnic group, education, age of symptom onset, number of prescriptions, number of medical
diagnoses, Mini-Mental State Examination (MMSE), Blessed-Roth Dementia Rating Scale
(BRDRS), probable versus possible AD diagnosis.
Results: Fifteen percent of the Alzheimer's disease patients were on a medication with potential to
impair cognition, and 44% were on a cholinesterase inhibitor. Patient characteristics associated with
the prescription of a medication with potential to impair cognition included total number of
prescription medications, low education, low MMSE, older age, reported lack of vitamin use, and
more medical diagnoses. Patient characteristics associated with the prescription of a cholinesterase
inhibitor included reported use of vitamins, the total number of prescription medications, fewer
medical diagnoses, lower age of symptom onset, and higher education.
Conclusions: Determining the patient characteristics associated with the prescription of a medi-
cation with potential to impair cognition can help clinicians identify patients who are at risk for
drug-related morbidity. Patient characteristics unassociated with dementia appear to influence the
prescription of cholinesterase inhibitors. Signal detection analysis is well suited to this type of
@ 2006 The Alzheimer's Association. All rights reserved.
Alzheimer's disease; inappropriate medications; cholinesterase inhibitors; Beers criteria; signal detection;
receiver operating characteristic analysis
total US population, they consume more than 25% of all
prescription medications and can have increased rates of
Inappropriate medication use, especially in the elderly,
adverse effects [I]. One of the challenges in this area has
has been a topic of increasing concern. Although older
been to develop criteria for inappropriate medication use. E.D Huey et al. / Alzheimer'.s & Dementia 2 (2006} 314-321
---------------------------------------------
On medication with potential to impair cognition
----------------------------------------------------------------------------------------------------------- ~
-----------------------------------------------------------------------------------------------------------
NOTE Numbers in parentheses are one standard deviation for reported means. Percentages in parentheses are percentages of patients with the charaeteristic
out of the total number of patients in each column. p value determined from univariate logistie regressions.
study was completed, the 2003 criteria rely more heavily
Type of medication used in patients taking a medication with potential
than the 1997 criteria on diagnosis-specific potentially in-
appropriate medications (which is not as well suited to the
analysis we used) and to facilitate comparison to the past
literature on this topic. In the Beers criteria, benzodiaz-
epines included individual medications as being potentially
inappropriate if they were above a certain dose. We did not
Methocarbamol (Roxabin), carisoprodol (Soma),
have records on specific doses of medications, so we were
unable to determine if patients were above a certain dose.
E.D Huey et al. / Alzheimer'.s & Dementia 2 (2006} 314-321
---------------------------------------------
On medication with potential to impair cognition
----------------------------------------------------------------------------------------------------------- ~
-----------------------------------------------------------------------------------------------------------
NOTE Numbers in parentheses are one standard deviation for reported means. Percentages in parentheses are percentages of patients with the charaeteristic
out of the total number of patients in each column. p value determined from univariate logistie regressions.
study was completed, the 2003 criteria rely more heavily
Type of medication used in patients taking a medication with potential
than the 1997 criteria on diagnosis-specific potentially in-
appropriate medications (which is not as well suited to the
analysis we used) and to facilitate comparison to the past
literature on this topic. In the Beers criteria, benzodiaz-
epines included individual medications as being potentially
inappropriate if they were above a certain dose. We did not
Methocarbamol (Roxabin), carisoprodol (Soma),
have records on specific doses of medications, so we were
unable to determine if patients were above a certain dose.
 E'. D. Huey et al. / A Izheimer'.I. & Dementia 2 (2006} 314-321
Of \ \ 38 patients on < 5 medications, 98 (9'/,)
Of 480 patients on > or = 5 medications, 90
Of 206 patients on < 9 medications, 55 (27%)
Of 130 patients on > or = 9 medications. 53
on med with potential to impair cognition
are on med with potential to impair cognition
(4 J %) are on med with potential to impair
Of 869 patients with MMSE Of 198 patients with MMSE
Fig I. ROC analysis of medications with potential to impair cognition.
one. The recursive partitioning process of signal detection
cance of p < 0.01, or the subgroup to be analyzed has 10 or
techniques automatically and systematically examines a se-
fewer subjects, or after the program has reached 3 levels of
ries of interactions [21] .In contrast, stepwise forward re-
analysis (i.e., creating a maximum of 8 subgroups). For
gression requires that the investigator enter alllower-order
continuous predictor variables (e.g., age), the procedure
interaction terms before considering higher-order interac-
calculates ROC curves first for the lowest value in the data
tions [21] .These explicit decisions can affect the magnitude
set, then for the lowest value plus 1, then plus 2, and so on,
of the estimated weights and thus the identified predictors
and ultimately selects the value with the best sensitivity and
[22]. Second, if there are reasons to believe that predictors
specificity. The ROC procedure can be set to differentially
are collinear (as in this study), signal detection may be
weight the analysis for sensitivity and specificity. Our anal-
preferred to logistic regression, because collinear predictors
yses were set to equally weigh sensitivity and specificity
can substantially bias the estimated weights for the predic-
thereby achieving both maximum sensitivity and maximum
tors in all-in logistic regression, independent of the actual
specificity. The ROC analysis software was developed at the
relationship between predictor and outcome [21,23,24].
E'. D. Huey et al. / A Izheimer'.I. & Dementia 2 (2006} 314-321
Of \ \ 38 patients on < 5 medications, 98 (9'/,)
Of 480 patients on > or = 5 medications, 90
Of 206 patients on < 9 medications, 55 (27%)
Of 130 patients on > or = 9 medications. 53
on med with potential to impair cognition
are on med with potential to impair cognition
(4 J %) are on med with potential to impair
Of 869 patients with MMSE Of 198 patients with MMSE
Fig I. ROC analysis of medications with potential to impair cognition.
one. The recursive partitioning process of signal detection
cance of p < 0.01, or the subgroup to be analyzed has 10 or
techniques automatically and systematically examines a se-
fewer subjects, or after the program has reached 3 levels of
ries of interactions [21] .In contrast, stepwise forward re-
analysis (i.e., creating a maximum of 8 subgroups). For
gression requires that the investigator enter alllower-order
continuous predictor variables (e.g., age), the procedure
interaction terms before considering higher-order interac-
calculates ROC curves first for the lowest value in the data
tions [21] .These explicit decisions can affect the magnitude
set, then for the lowest value plus 1, then plus 2, and so on,
of the estimated weights and thus the identified predictors
and ultimately selects the value with the best sensitivity and
[22]. Second, if there are reasons to believe that predictors
specificity. The ROC procedure can be set to differentially
are collinear (as in this study), signal detection may be
weight the analysis for sensitivity and specificity. Our anal-
preferred to logistic regression, because collinear predictors
yses were set to equally weigh sensitivity and specificity
can substantially bias the estimated weights for the predic-
thereby achieving both maximum sensitivity and maximum
tors in all-in logistic regression, independent of the actual
specificity. The ROC analysis software was developed at the
relationship between predictor and outcome [21,23,24].

 E.D. Huey et al / Alzheimer's & Dementia 2 (2006} 314-321
Of 1844 patients wilh age < 89,265 (14%)
Of 100 patienls with age > or = 89, 30
on med with potential to impair cognition
Of 1536 patients with MMSE > or = 10.204
on med with potcntial to impair cognition
Of 1393 patients with < 4 medical diagnoses,
Of 143 patients with > or = 4 medical
Of91 patientson>or= 1 vitamin. 1) (12%)
Of 106 paticnts on 0 vitamins, 31 (29%) on
175 (13%) on med with potential to impair
diagnoses, 29 (20%) on med with potential to
on med with potcntial to impair cognition
Fig 2. ROC analysis of medications with potential to impair cognition excluding number of prescriptions.
3.2. Cholinesterase inhibitor use
several steps in the analysis, as we expected based on the
results of previous studies and because our outcome vari-
able affects this variable. (Because we are looking at the
Forty-four percent of the patients were on a cholinester-
possibility of being prescribed a certain medication, being
ase inhibitor at the time of their initial evaluation (Fig. 3).
E.D. Huey et al / Alzheimer's & Dementia 2 (2006} 314-321
Of 1844 patients wilh age < 89,265 (14%)
Of 100 patienls with age > or = 89, 30
on med with potential to impair cognition
Of 1536 patients with MMSE > or = 10.204
on med with potcntial to impair cognition
Of 1393 patients with < 4 medical diagnoses,
Of 143 patients with > or = 4 medical
Of91 patientson>or= 1 vitamin. 1) (12%)
Of 106 paticnts on 0 vitamins, 31 (29%) on
175 (13%) on med with potential to impair
diagnoses, 29 (20%) on med with potential to
on med with potcntial to impair cognition
Fig 2. ROC analysis of medications with potential to impair cognition excluding number of prescriptions.
3.2. Cholinesterase inhibitor use
several steps in the analysis, as we expected based on the
results of previous studies and because our outcome vari-
able affects this variable. (Because we are looking at the
Forty-four percent of the patients were on a cholinester-
possibility of being prescribed a certain medication, being
ase inhibitor at the time of their initial evaluation (Fig. 3).
 E. D. Huey et al. / Alzheimer's & Dementia 2 (2006) 314--321
Of 553 patients with < 2 medical diagnoses.
E. D. Huey et al. / Alzheimer's & Dementia 2 (2006) 314--321
Of 553 patients with < 2 medical diagnoses.