Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
Untitled
Journal of Veterinary Emergency and Critical Care 19(2) 2009, pp 158–164
Use of human immunoglobulin in addition toglucocorticoids for the initial treatment of dogswith immune-mediated hemolytic anemia
Megan F. Whelan, DVM, DACVECC; Therese E. O’Toole, DVM, DACVIM; Daniel L. Chan, DVM,DACVECC, DACVN, MRCVS; Elizabeth A. Rozanski, DVM, DACVECC, DACVIM; Armelle M. deLaforcade, DVM, DACVECC; Sybil L. Crawford, PhD, and Susan M. Cotter, DVM, DACVIM
Objective –To determine the utility of human intravenous immunoglobulin (hIVIG) for the initial treatment ofcanine immune-mediated hemolytic anemia (IMHA). Design –Blinded, randomized, clinical trial. Setting –Veterinary teaching hospital. Animals –Twenty-eight, client-owned dogs with primary IMHA. Interventions –At enrollment, after diagnosis of IMHA, dogs were randomly assigned to receive eitherhIVIG or placebo, in a blinded fashion. For the next 14 days, all dogs received glucocorticoids as the soleimmunosuppressant agent. All dogs received low-molecular-weight heparin as an anticoagulant. D-dimerconcentrations were evaluated at the beginning and end of the study protocol to monitor for thromboemboliccomplications. Measurements and Main Results –Twenty-five of 28 dogs (89%) were discharged from the hospital. Thirteenof those received hIVIG and 12 received placebo. Twenty-four dogs (86%) were alive 14 days after enrollment,and of these 13 received hIVIG and 11 received placebo. D-dimer concentrations were elevated in 86% of alldogs at the time of diagnosis. Conclusions –For initial treatment of dogs with IMHA, the addition of hIVIG to corticosteroid treatment didnot improve initial response, nor did it shorten hospitalization.
(J Vet Emerg Crit Care 2009; 19(2): 158–164) doi: 10.1111/j.1476-4431.2009.00403.x
Keywords: autoimmune hemolytic anemia, D-dimer, icterus, thromboembolism
The condition is considered to be primary after otherdetectable causes of hemolytic anemia have been ruled
Immune-mediated hemolytic anemia (IMHA) occurs
out. Many different treatment regimens have been uti-
commonly in dogs and has variable degrees of severity.
lized.1–7 Despite the growing availability of tertiary carefacilities and intensive care management, morbidity
From the Cummings School of Veterinary Medicine at Tufts University,
and mortality associated with IMHA remain high. Pre-
North Grafton, MA 01536 (Whelan, O’Toole, Chan, Rozanski, deLaforcade,
viously reported mortality rates ranging from 29%8 to
Cotter); and the University of Massachusetts Medical School, Worcester,
70%7 have not changed over the last 2 decades.9
Glucocorticoids are the most commonly used treat-
The study was conducted at the Cummings School of Veterinary Medicineat Tufts University. The study was supported by a grant from The Barry
ment to induce immunosuppression. The fact that some
and Savannah French-Poodle Memorial Fund.
dogs fail to respond and others respond initially only to
The authors report no financial conflicts of interest.
relapse later has led to the addition of other drugs. Those commonly advocated drugs either alone or in
Dr. Chan’s current address: The Royal Veterinary College, HawksheadLane, North Mymms, Hatfield, Hertfordshire AL9 7TA, UK.
Address correspondence and reprint requests to
cyclophosphamide,2,3,5,6,11 cyclosporine,11,a and human
Dr. Susan M. Cotter, Department of Clinical Sciences, Cummings School of
intravenous immunoglobulin (hIVIG).1,5,10–12 All drugs
Veterinary Medicine at Tufts University, 200 Westboro Road, North Grafton,
other than glucocorticoids have been used anecdotally
without adequate study. No additional treatment has
& Veterinary Emergency and Critical Care Society 2009
proven to be superior to glucocorticoids alone for initial
cost and inconsistent availability of hIVIG to veterinary
clinicians makes the use of hIVIG difficult to justify
hIVIG has been used in humans for over 25 years13
without further evidence of efficacy and safety. Human
for treatment of a variety of diseases, primarily im-
IVIG costs approximately US$125/g. The average cost
mune-mediated thrombocytopenia and other immune-
for a 20-kg dog could approach US$3,000.
mediated diseases. Occasional reports exist of its use
In humans, hIVIG has been associated with adverse
as a second line drug in IMHA.14,15 hIVIG is composed
effects, including thrombotic events.24 Because many
of highly purified immunoglobulin G (IgG), obtained
dogs with severe IMHA have developed thromboem-
from large pools of donated human plasma.13 The
bolic complications, any additional risk imposed by
mechanism of action of hIVIG is complex, including
hIVIG must be evaluated and considered when treat-
modulation of expression and function of Fc receptors,
ment decisions are made.4,25 The purpose of this study
interference with activation of B and T cells and com-
was to determine whether the addition of hIVIG to
plement, and a decrease in immunoglobulin produc-
glucocorticoid therapy would improve initial response
tion.13 Similar effects of hIVIG on canine white blood
and survival in dogs with IMHA, and whether adverse
cells have been described.16 Although not approved for
effects, especially thromboembolism, would be associ-
use in dogs, hIVIG has been reported as a treatment
for canine IMHA,1,5,17,18 and canine immune-mediatedthrombocytopenia,19 and for severe dermatological
conditions such as pemphigus and drug allergies.20–23hIVIG has been evaluated in both prospective1 and ret-
Twenty-eight client-owned dogs with primary IMHA
rospective5,11,12,18 clinical trials in dogs. Scott-Moncrieff
were enrolled between April 2005 and December 2006.
et al12 described the administration of hIVIG to 5 dogs
This study was conducted with approval by the Cum-
and concluded that its efficacy was not known at that
mings School of Veterinary Medicine at Tufts Univer-
time. Kellerman et al5 gave hIVIG in conjunction with
sity Institutional Animal Care and Use Committee, and
various other conventional immunosuppressive drugs
written informed consent was obtained from all own-
to 13 dogs and concluded that it may be of value to
ers. All potential study dogs were evaluated by per-
those dogs who do not respond to corticosteroids
forming a complete history, physical examination,
within 7 days. Grundy et al11 retrospectively reported
complete blood count, reticulocyte count, serum bio-
on 88 dogs with primary IMHA that received various
chemical, and coagulation profiles. A direct Coombs
treatments including hIVIG. In this study, mortality
test was conducted if autoagglutination cleared with
was not significantly associated with hIVIG adminis-
the addition of saline, or was absent. All dogs had sur-
tration, and the authors concluded that hIVIG therapy
vey thoracic radiographs (3 views) and an ultrasono-
may be beneficial. Gerber et al18 gave hIVIG in addition
graphic examination of the abdomen to exclude other
to other immunosuppressive agents, to 9 dogs, and de-
possible causes of hemolytic anemia and to evaluate for
scribed a potential positive effect despite the fact that
evidence of preexisting thromboembolism in the lungs
the dogs who received hIVIG were more severely
or in splenic or other abdominal vessels. Eligibility for
affected. The only prospective study, conducted by
inclusion included dogs with anemia (HCTo28%) and
Scott-Moncrieff et al,1 evaluated the use of hIVIG in
the presence of autoagglutination, spherocytosis, or a
10 dogs with IMHA that failed to respond to conven-
positive direct Coombs test. Dogs were included if no
tional immunosuppression. The authors concluded that
underlying cause for IMHA was identified. Dogs were
hIVIG may be useful for short-term stabilization of
excluded if any glucocorticoid medication had been
administered for 448 hours before admission, or if any
Generally hIVIG was used in dogs that did not re-
other immunosuppressive drugs had been adminis-
spond to corticosteroids or other immunosuppressive
tered since diagnosis. Of 29 dogs considered eligible,
drugs, either by replacing these drugs, or by using it
concurrently. Although it was hypothesized that hIVIG
Dogs with primary IMHA meeting the inclusion cri-
may be helpful, it was often difficult to determine ex-
teria were randomly assigned to either (1) glucocor-
actly what drug or combination caused the response.
ticoids alone (placebo group) or (2) glucocorticoids and
A randomized, blinded, placebo-controlled evaluation
hIVIG (hIVIG group). Assignment was made by ran-
has not yet been reported. Because the blockade of Fc
dom selection of a sealed envelope from a mixed stack
receptors by hIVIG is an immediate effect, and because
of 28 envelopes directing either hIVIG (14) or placebo
mortality can be high in the first few days of treatment,
(14) administration. The treatment assignment was
our hypothesis was that hIVIG would be helpful for
known only by the designated individual responsible
initial stabilization of patients. Concurrently, the high
for the reconstitution of the treatment solution; this
& Veterinary Emergency and Critical Care Society 2009, doi: 10.1111/j.1476-4431.2009.00403.x
individual was not involved in clinical management
ples were batched, and submitted at the end of the
of the patient. If glucocorticoid treatment had been
study for analysisk via a latex agglutination assay.
started before enrollment in the trial, an immunosup-
The PCV and total plasma protein were monitored
pressive dose of prednisoneb (3 mg/kg, PO, q 24 h) was
twice daily during hospitalization, or more frequently if
continued. All other dogs received a single dose of
clinically indicated. Prednisone was continued in both
dexamethasone sodium phosphatec (0.3 mg/kg, IV) fol-
groups as the sole immunosuppressive agent for at
lowed by prednisone (3 mg/kg, PO, q 24 h). If vomiting
least 14 days. After that time other immunosuppressive
precluded oral therapy, prednisolone acetated was
agents could be added or substituted if deemed neces-
substituted at the same dose, subcutaneously. All
dogs received prophylactic anticoagulation with low–molecular-weight heparin (dalteparin,e 150 IU/kg, SQ,
q 12 h), beginning at the same time as other medica-
Abnormalities previously reported to have prognostic
tions. Other supportive management including blood
significance in canine IMHA were specifically com-
transfusions, IV fluids, gastroprotectants, or antimicro-
pared between groups at the time of entry into the
bials was administered to some dogs, at the discretion
study and included parameters such as HCT, ret-
of the managing clinician. The decision as to when to
iculocyte count, Coombs test results (polyspecific anti-
transfuse was made on the basis of clinical signs of
bodies to canine IgG, IgM, and complement) at 371C,
anemia, weakness, tachycardia, tachypnea, and bound-
white blood cell count, presence of band neutrophils
ing pulses, not on a laboratory-based transfusion trigger.
(40.1 Â 109/L), nucleated red blood cells, autoag-
hIVIGf was reconstituted with the prescribed volume
glutination, or spherocytes. Additional comparisons
of sterile water according to the manufacturer’s in-
included presence of thrombocytopenia or other abnor-
structions. The amount reconstituted was calculated to
malities on the coagulation profile as well as, elevation
provide a dosage of 0.5 g/kg daily for 3 consecutive
of serum bilirubin concentration, alkaline phosphatase
days. All infused hIVIG was refrigerated and admin-
activity, or hypoalbuminemia on the chemistry profile.
istered within 24 hours of reconstitution to minimize
D-dimer concentrations were measured pre- and post-
risk of bacterial contamination. The placebo treatment
study drug infusion, to monitor for any increased
consisted of 0.9% NaClg at the same calculated volume
as projected for hIVIG. All personnel involved in case
Remission was defined as stabilization of PCV for
management and nursing care, as well as the owners
48 hours, and subsequent increase with no further
were blinded as to the study drug group assignment.
transfusion requirement. Information recorded in-
To maintain concealment, the study drug or placebo
cluded number of days from the start of glucocorticoid
was transferred to a sterile infusion bagh covered with
medication to remission, number of days from last
a second, opaque plastic bag with the inscribed de-
blood transfusion to remission, and number of days to
scription IMHA study drug. The study drug, supplied
PCV normalization (reference interval, 39–55%). Also
without cost to the owner, was then administered in-
recorded were packed red blood cell transfusion vol-
travenously over 6 hours via a dedicated IV line with
ume (mL/kg), length of hospital stay, survival to dis-
charge from the hospital, survival to 14 days after start
During the administration of the study drug or pla-
of treatment, and beyond 40 days after discharge.
cebo, systolic blood pressure measured using an ultra-
Adverse events were noted, as well as total cost of
sonic Doppler flow detector,i heart and respiratory
rates, temperature, and appearance of the catheter siteand limb were evaluated hourly. All other IV fluids
were discontinued during the infusion, and any ad-
All analyses were conducted using a statistical software
justment in infusion rate was determined by changes in
program.l The population parameters for the 28 dogs
physical findings or blood pressure. Blood samples for
enrolled in the study were summarized using frequen-
D-dimer analysis were obtained pre- and poststudy
cies and medians for categorical data and means and
drug administration. Blood, drawn from the jugular
standard deviations for continuous variables. The 2
vein using a plastic syringe and needle, was immedi-
treatment arms were compared using w2 testing for cat-
ately placed in an evacuated blood tube containing
egorical variables and Wilcoxon’s signed rank testing
3.8% sodium citrate,j and spun for 10 minutes in a table-
for continuous variables. The mean within-dog change
top centrifuge at 1,315 Â g. Before freezing, 6 samples
in D-dimer concentrations (pre versus post) were also
were analyzed at our own laboratory using a latex
compared between the 2 treatment arms using a
agglutination assay.k All samples then had the plasma
method applied by Evans et al26 to handle floor and
separated and stored in a plastic tube at À 801C. Sam-
ceiling effects. Briefly, within-dog changes were ranked
& Veterinary Emergency and Critical Care Society 2009, doi: 10.1111/j.1476-4431.2009.00403.x
Table 1: Comparison at admission between 14 dogs receiving human intravenous immunoglobulin (hIVIG) and 14 receiving placebo
All values listed as median (range) or patient number. nWilcoxon’s signed ranks test or Fisher’s exact test. wOmitting 1 value of ‘clumped’. M, male; F, female; HCT, hematocrit; NRBC, nucleated red blood cell; PT, prothrombin time; APTT, activated partial thromboplastin time; FDPs, fibrindegradation products.
separately for each pre D-dimer value, the ranks
Of the 14 dogs in the hIVIG group, 13 were dis-
were transformed using normal scores, and the trans-
charged from the hospital and were still alive at day 14
formed ranks were compared by treatment arm using
(Figure 1). Five additional dogs in this group were eu-
Wilcoxon’s signed rank testing. Also, exact P-values, for
thanized within 40 days after discharge, and 8 re-
within-dog change in D-dimer value, were computed
mained alive and in remission beyond 5 months. The
for each treatment arm separately using a test of mar-
median number of days for PCV stabilization was 4.
ginal homogeneity, an extension of McNemar’s test for
Twelve dogs in the placebo group were discharged.
more than 2 categories.27 Finally, correlates of duration
One additional dog from this group was euthanized by
of survival were identified using Kaplan-Meier estima-
day 14, and 11 remained alive and in remission beyond
tion and Cox proportional hazards modeling.28
Twenty-eight dogs with primary IMHA were enrolledas shown in Table 1. Fourteen were assigned to receivehIVIG and 14 to receive placebo. The study popula-tion consisted of 10 males (9 neutered), 18 females(7 spayed). Twenty-six dogs were purebred and in-cluded American Cocker Spaniel (n 5 4 total, 2 in eachstudy group), English Cocker Spaniel (n 5 2), StandardPoodle (n 5 2), Maltese (n 5 2), Border Collie (n 5 2),and 1 each of 14 other breeds. No significant differenceswere found between groups in age, sex, or prognosticvariables. On admission, the mean HCT of all dogs was15%
9–27%). All dogs had anemia and agglutination orspherocytosis.
Figure 1: Comparison of survival between the 2 study groups.
& Veterinary Emergency and Critical Care Society 2009, doi: 10.1111/j.1476-4431.2009.00403.x
5 months. The median number of days for PCV stabi-lization was 5. None of the differences in survival, timeto PCV stabilization, or length of hospitalization be-tween the 2 groups were statistically significant.
Three dogs were euthanized during hospitalization,
1 in the hIVIG group, and 2 in the placebo group. Thedog in the hIVIG group was euthanized on day 5 be-cause of ongoing hemolysis despite receiving the totaldose of study drug without complications. The 2 dogsin the placebo group were euthanized on days 1 and 2after acute onset of central nervous system signs. These2 dogs each received only 1 infusion of placebo. One doghad a necropsy that showed pulmonary thromboemboliand evidence of multiorgan hemorrhage, including thebrain. Grossly, the brain had multifocal regions of hem-orrhage on the frontal lobe, right parietal lobe, cranialcerebellum, and within the pituitary gland. Other areasof the brain examined microscopically were normal.
Figure 2: Comparison of D-dimer values between study groupsbefore and after the study drug with Fisher’s exact P-values. (n)
Of the 6 dogs (5 in hIVIG group and 1 in placebo
Omitting 1 dog from the placebo group that did not have a
group) euthanized within 40 days after discharge, re-
ported abnormalities included continued hemolysis in2 dogs, renal failure, undiagnosed paresis, respiratory
Coombs results, platelet count, amount of blood trans-
distress, and ascites in 1 dog each. Necropsies were
fused, white blood cell count, presence of band neutro-
conducted on 2 of these dogs, 1 with respiratory dis-
phils, partial thromboplastin time, fibrinogen, fibrinogen
tress and the other with undiagnosed posterior paresis.
degradation products, alkaline phosphatase, and albu-
Grossly, the dog with respiratory distress had evidence
min were not found to be associated with mortality.
of thrombi in the lung and spleen, whereas the spinal
Systolic arterial blood pressure increased during the
cord and spinal vertebrae of the second dog were nor-
infusion in 20 dogs, 12 of which were in the hIVIG
mal both on gross and histologic examination.
group. The difference between groups was not signifi-
Twenty-six of the 28 dogs received packed red blood
cant. No dogs developed significant changes in tem-
cell transfusions with a mean transfusion volume of
perature or heart rate that required intervention. Two
23 mL/kg (range, 10–56 mL/kg). No difference was de-
dogs receiving hIVIG developed swelling in the infu-
tected in transfusion requirement between the 2 groups.
sion leg. The protocol was continued via a newly placed
On admission, 24 of the 28 dogs had elevation in
catheter, and after the affected legs were warm packed,
D-dimer concentrations. Before studying drug infusion
the swelling resolved within 24 hours without residual
the median D-dimer concentration of the 2 groups was
complications. One dog in the hIVIG group with pre-
the same (500–1000 mg/L; the assay’s detectable range
viously asymptomatic mitral insufficiency developed
was o250–42000 and o250 mg/L was considered the
an increased respiratory rate and effort during the third
reference interval for clinically healthy dogs). The
infusion. Radiographic evidence of volume overload
hIVIG group showed a slight, but not significant
prompted discontinuation of the infusion. This dog had
(P 5 0.11) increase in D-dimers following infusion of
received 83% of the total assigned dose.
the study drug. No significant change (P 5 0.69) in the
The mean cost of hospitalization for all 28 dogs was
D-dimer concentrations was noted in the placebo
US$3,771, with a range of US$1,652–US$8,753. The
group. Similarly, no difference was noted between
hIVIG was provided without charge to enable random-
groups (P 5 0.61 prestudy drug, and P 5 0.27 poststudy
ization. If the cost of hIVIG was added, the mean cost
would have increased by approximately 50%.
In all 28 dogs, factors identified on admission that
were associated with increased mortality included el-evation in total serum bilirubin (hazard ratio 5 1.03,
95% confidence interval [CI] 5 1.00–1.07, P 5 0.05) andprolonged prothrombin time (hazard ratio 5 1.46, 95%
IMHA is a common condition, and many dogs respond
CI 5 1.05–2.02, P 5 0.02). All other variables including
well to glucocorticoid therapy alone. Transfusion-
temperature, respiratory rate, heart rate, HCT, presence
dependent dogs with IMHA tend to be more difficult
of autoagglutination, spherocytes, or reticulocytosis,
to manage, and may be referred to tertiary care facilities
& Veterinary Emergency and Critical Care Society 2009, doi: 10.1111/j.1476-4431.2009.00403.x
where stronger immunosuppressive protocols are gen-
in 2 dogs, which had not been identified on thoracic
erally used. The variable response to these protocols
radiographs. This is not unexpected because thoracic
likely depends on several factors, including primarily
radiographs can often be normal in these cases. It might
the extent of illness, the drug protocol chosen, and
also be speculated that the development of neurologic
seemingly the degree of monitoring and critical care. In
signs and posterior paresis may have been caused
some dogs with severe IMHA, hIVIG has been added to
by undetected thromboembolism. A specific D-dimer
other drugs after publication of reports that hIVIG im-
concentration could not be identified as a prognostic
proves outcome in dogs that failed to improve after
indicator, because 2 of the 4 dogs with D-dimer con-
initial treatment.1,5,9 To our knowledge, however, no
centrations 42000 mg/L at admission did not survive
prospective, blinded, randomized, placebo-controlled
to discharge. There did not appear to be a difference in
investigations have previously been undertaken to pro-
rate of thrombotic disease between the groups.
vide evidence of efficacy of any of these protocols.
It would seem reasonable that early institution of pro-
The hIVIG and placebo groups were statistically sim-
phylactic anticoagulation might be helpful in preventing
ilar to each other based on data collected at admission.
this complication. One group reported that ultralow-
Adverse prognostic factors that have been identified in
dose aspirin was effective in preventing thromboem-
prior reports were further evaluated, as well as some
bolic complications in dogs being treated for IMHA.10
others.29 The only significant adverse prognostic find-
Although we used low–molecular-weight heparin to
ings in this study in both groups were an hyper-
try to prevent this complication, we were not entirely
bilirubinemia and prolonged prothrombin time at
successful. The best drug or even the need for antico-
agulation in management of dogs with IMHA has not
In this group of 28 dogs with IMHA, all but 2 re-
been extensively investigated, and more work is
quired transfusions. No significant difference was
found between the hIVIG group and the placebo group
We failed to detect a statistical difference in D-dimer
in number or volume of blood transfusions required.
concentrations between or within groups. A larger sam-
The length of hospitalization did not differ between the
ple size or inclusion of other coagulation parameters to
2 groups. Although the group receiving hIVIG tended
monitor for thrombotic tendencies might have given
to have stabilization of PCV approximately 1 day
better insight into the detection and extent of ongoing
sooner than the placebo group, this difference was not
thromboembolism and consumption coagulopathy.
significant. Survival to discharge was comparable be-
This study was limited to a relatively small number
tween the dogs receiving hIVIG and placebo. Although
of dogs, and thus statistical power to detect treatment-
5 of the 6 dogs euthanized within 40 days after dis-
related differences smaller than a magnitude of 0.8
charge had received hIVIG, the difference in survival
standard deviations was also limited.32 Although the
at that time was not significant. Reported mortality
use of post-hoc power calculations is controversial,
rates with canine IMHA have ranged from 29% to 70%.
these calculations were performed and demonstrate
In this study, 14% of dogs were euthanized in the first
that the current study was underpowered (power for
14 days, and an additional 18% within 40 days after
the study endpoints ranged from only 5–36%). In light
discharge, resulting in an overall mortality of 32%.
of these findings, failure to detect statistical significance
Although long-term survival was not an endpoint of
in various endpoints could be due to inadequate sam-
the study, all 19 dogs remaining in remission 40 days
ple size of the population or a true lack of difference
after discharge, remained clinically well 5 months after
between treatment protocols. However, if there was a
difference, it was not likely enough to warrant the ad-
Thromboembolism has been reported as a significant
ditional costs of the hIVIG. Data from the current study
cause of death in dogs with IMHA,4,8,25,29 as high as
can now be used to design adequately powered studies
80% in one study.29 In addition, the use of glucocor-
ticoids30 and placement of IV catheters may contribute
All dogs in both groups received glucocorticoid
to the risk of thrombotic complications. The presence of
treatment for at least 14 days after diagnosis. Less ag-
D-dimer elevation, as part of a coagulation profile, is
gressive immunosuppression with prednisone used as
an accepted indication of active coagulation and fibrin-
a single agent might allow for response with fewer ad-
olysis.31 In one prospective study 16 of 20 dogs with
verse effects than might occur with more potent drugs.
primary IMHA had elevations in D-dimer concentra-
For example, the addition of cyclophosphamide to pre-
tions.30 In our study, 24 of 28 dogs had elevations in
dnisone has not improved survival, and may even have
D-dimers on admission and evidence of thromboem-
been detrimental.2,6,11 Some authors have suggested
bolism was identified in 2 of the 3 necropsies con-
improved outcomes with azathioprine2,7,10 or cyclo-
ducted. Necropsy identified pulmonary thromboemboli
sporine,a but most dogs received these drugs only after
& Veterinary Emergency and Critical Care Society 2009, doi: 10.1111/j.1476-4431.2009.00403.x
they had already received prednisone for several days
8. Klag AR, Giger U, Shofer FS. Idiopathic immune-mediated hemo-
lytic anemia in dogs: 42 cases (1986–1990). J Am Vet Med Assoc
or longer. They may have inadvertently selected a
group with a better prognosis because many severely
9. McCullough S. Immune-mediated hemolytic anemia: understand-
affected dogs fail to survive beyond the first few days,
ing the nemesis. Vet Clin Small Anim 2003; 33(6):1295–1315.
10. Weinkle TK, Center SA, Randolph JF, et al. Evaluation of prog-
and would not have received the additional drugs. To
nostic factors, survival rates, and treatment protocols for immune-
date, no investigations have proven the benefit of any
mediated hemolytic anemia in dogs: 151 cases (1993–2002). J Am
additional immunosuppressive drugs over the use of
Vet Med Assoc 2005; 226(11):1869–1880.
11. Grundy SA, Barton C. Influence of drug treatment on survival of
dogs with immune-mediated hemolytic anemia: 88 cases (1989–
In summary, for initial treatment of dogs with IMHA,
1999). J Am Vet Med Assoc 2001; 218(4):543–546.
the addition of hIVIG to glucocorticoids did not im-
12. Scott-Moncrieff JC, Reagan WJ, Glickman LT, et al. Treatment of
nonregenerative anemia with human g-globulin in dogs. J Am Vet
prove response or survival, nor did it shorten length of
Med Assoc 1999; 206(12):1895–1900.
hospitalization nor decrease the transfusion require-
13. Kazatchkine MD, Kaveri SV. Immunomodulation of autoimmune
ment when compared with glucocorticoids alone.
and inflammatory diseases with intravenous immune globulin. N Engl J Med 2001; 345(10):747–755.
14. Kurtzberg J, Friedman HS, Chaffee S, et al. Efficacy of intravenous
gamma globulin in autoimmune-mediated pediatric blood dys-
crasias. Am J Med 1987; 83(4A):4–9.
15. Flores G, Cunningham-Rundles C, Newland AC, et al. Efficacy of
We would like to thank Dr. Scott Shaw for his help with
intravenous immunoglobulin in the treatment of autoimmune he-
molytic anemia: results in 73 patients. Am J Hematol 1993;44(4):237–242.
16. Reagan WJ, Scott-Moncrieff JC, Christian J, et al. Effects of human
intravenous immunoglobulin on canine monocytes and lympho-
cytes. Am J Vet Res 1998; 59(12):1568–1574.
17. Scott-Moncrieff JC, Reagan WJ. Human intravenous immunoglob-
Wohl JS, Moore AS. The use of single-agent cyclosporine A in dogs with
ulin therapy. Semin Vet Med Surg 1997; 12(3):178–185.
severe immune mediated hemolytic anemia (abstr). J Vet Intern Med1996; 10(3):173.
18. Gerber B, Steger A, Hassig M, et al. Use of human intravenous
Prednisone, Roxane Laboratories Inc, Columbus, OH.
immunoglobulin in dogs with primary immune mediated hemo-
Dexamethasone sodium phosphate, The Butler Co, Columbus, OH.
lytic anemia. Schweiz Arch Tierheilkd 2002; 144(4):180–185.
Prednisone acetate, Prescription Specialties Pharmacy Inc, Chesire, CT.
19. Bianco D, Armstong J, Washabau R, et al. Treatment of severe
Dalteparin sodium, Fragmin, Pfizer, New York, NY.
immune-mediated thrombocytopenia with human IV immuno-
Gammagard S/D, Baxter Healthcare Corp, Westlake Village, CA.
globulin in 5 dogs. J Vet Intern Med 2007; 21(4):694–699.
0.9% Saline, Baxter Healthcare Corp, Deerfield, IL.
20. Byrne KP, Giger U. Use of human immunoglobulin for treatment
Ethylene Vinyl Acetate TPN bag, Baxter Healthcare Corp.
of severe erythema mulitforme in a cat. J Am Vet Med Assoc 2002;
Ultrasonic Doppler Flow Detector 811-BL, Parks Medical Inc, Aloha, OR.
BD Vacutainer Plus Citrate Tubes (1.8 mL, 3.8% sodium citrate), Becton
21. Nutall TJ, Malham T. Successful intravenous human immuno-
globulin treatment of drug-induced Stevens-Johnson syndrome in
Comparative coagulation section diagnostic laboratory, College of
a dog. J Small Anim Pract 2004; 45(7):357–361.
Veterinary Medicine Cornell University, Ithaca, NY.
22. Rahilly LJ, Keating JH, O’Toole TE. The use of intravenous human
SAS/STAT version 9.1, SAS Institute Inc, Cary, NC.
immunoglobulin in treatment of severe pemphigus foliaceus in adog. J Vet Intern Med 2006; 20(6):1483–1486.
23. Trotman TK, Phillips H, Fordyce H, et al. Treatment of severe ad-
verse cutaneous drug reactions with human intravenous immuno-globulin in two dogs. J Am Anim Hosp Assoc 2006; 42(4):312–320.
1. Scott-Moncrieff JC, Reagan WJ, Synder PW, et al. Intravenous ad-
24. Gammagard S/D [package insert]. Westlake Village, CA: Bussel,
ministration of human immune globulin in dogs with immune-
mediated hemolytic anemia. J Am Vet Med Assoc 1997; 210(11):
25. Klein MK, Dow SK, Rosychuk RAW. Pulmonary thromboembo-
lism associated with immune-mediated hemolytic anemia in dogs:
2. Burgess K, Moore A, Rand W, et al. Treatment of immune-
ten cases (1982–1987). J Am Vet Med Assoc 1989; 195(2):246–250.
mediated hemolytic anemia in dogs with cyclophosphamide. J Vet
26. Evans DA, Beckett LA, Albert MS, et al. Level of education and
change in cognitive function in a community population of older
3. Matus RE, Schrader LA, Leifer CE, et al. Plasmapheresis as ad-
persons. Ann Epidemiol 1993; 3:71–77.
juvant therapy for autoimmune hemolytic anemia. J Am Vet Med
27. Agresti A. Categorical Data Analysis. New York: John Wiley &
4. Thompson MF, Scott-Moncrieff JC, Brooks MB. Effect of a single
28. Cox DR. Regression models and life tables. J R Statist Soc B 1972;
plasma transfusion on thromboembolism in 13 dogs with primary
immune-mediated hemolytic anemia. J Am Anim Hosp Assoc
29. Carr AP, Panciera DL, Kidd L. Prognostic factors for mortality and
thromboembolism in canine immune-mediated hemolytic anemia:
5. Kellerman DL, Bruyette DS. Intravenous human immunoglobulin
a retrospective study of 72 dogs. J Vet Intern Med 2002; 16(5):
for treatment of immune-mediated hemolytic anemia in 13 dogs.
J Vet Intern Med 1997; 11(6):327–332.
30. Scott-Moncrieff JC, Treadwell NG, McCullough SM, et al. Hemo-
6. Mason N, Duval D, Shofer FS, et al. Cyclophosphamide exerts no
static abnormalities in dogs with primary immune-mediated he-
beneficial effect over prednisone alone in the initial treatment of
molytic anemia. J Am Anim Hosp Assoc 2001; 37(3):220–227.
acute immune-mediated hemolytic anemia in dogs: a randomized
31. Nelson OL. Use of the D-dimer assay for diagnosing thromboem-
controlled clinical trial. J Vet Intern Med 2003; 17(2):206–212.
bolic disease in the dog. J Am Anim Hosp Assoc 2005; 41(3):
7. Reimer ME, Troy GC, Warnick LD. Immune-mediated hemolytic
anemia 70 cases (1988–1996). J Am Anim Hosp Assoc 1999;
32. Cohen J. Statistical Power Analysis for the Behavioral Sciences, 1st
ed. New York, NY: Academic Press; 1977, pp. 25–26.
& Veterinary Emergency and Critical Care Society 2009, doi: 10.1111/j.1476-4431.2009.00403.x
What are the issues around the age of a child? The main issues around the age of a child are: • The age until which children should fall under the provisions of the Bill; • The minimum age for prosecution of a child; • The age until which criminal incapacity is presumed but may be rebutted; and • Problems around determining the age of a child. The Child Justice Bill establi
Nell’Europa27+EFTA1 sono state registrate complessivamente 1,06 milioni di vetture nel mese di aprile 2012, con una flessione del 6,5 % rispetto allo stesso mese del 2011, pari a 73.800 mila unità in meno. APRILE 2012 APRILE 2011 UE27+EFTA 1.058.348 1.132.172 GEN/APRILE 2012 GEN/APRILE 2011 UE27+EFTA 4.487.798 4.829.116 Rispetto al mese di aprile 20
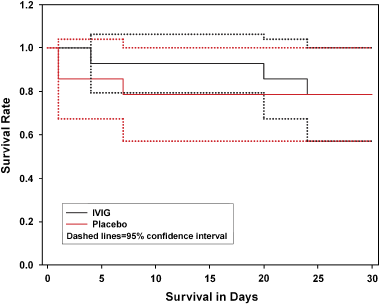 Table 1: Comparison at admission between 14 dogs receiving human intravenous immunoglobulin (hIVIG) and 14 receiving placebo
All values listed as median (range) or patient number.
Table 1: Comparison at admission between 14 dogs receiving human intravenous immunoglobulin (hIVIG) and 14 receiving placebo
All values listed as median (range) or patient number.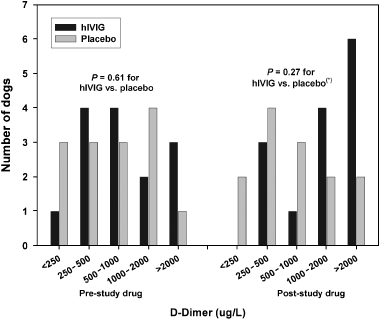 5 months. The median number of days for PCV stabi-lization was 5. None of the differences in survival, timeto PCV stabilization, or length of hospitalization be-tween the 2 groups were statistically significant.
5 months. The median number of days for PCV stabi-lization was 5. None of the differences in survival, timeto PCV stabilization, or length of hospitalization be-tween the 2 groups were statistically significant.