Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
Vibrafit.com.ar
JOURNAL OF BONE AND MINERAL RESEARCH Volume 19, Number 3, 2004 Published online on December 22, 2003; doi: 10.1359/JBMR.0301245 2004 American Society for Bone and Mineral Research
Effect of 6-Month Whole Body Vibration Training on Hip Density,
Muscle Strength, and Postural Control in Postmenopausal Women:
Sabine MP Verschueren,1 Machteld Roelants,2 Christophe Delecluse,2 Stephan Swinnen,1
ABSTRACT: High-frequency mechanical strain seems to stimulate bone strength in animals. In this random- ized controlled trial, hip BMD was measured in postmenopausal women after a 24-week whole body vibration (WBV) training program. Vibration training significantly increased BMD of the hip. These findings suggest that WBV training might be useful in the prevention of osteoporosis. Introduction: High-frequency mechanical strain has been shown to stimulate bone strength in different animal models. However, the effects of vibration exercise on the human skeleton have rarely been studied. Particularly in postmenopausal women—who are most at risk of developing osteoporosis—randomized controlled data on the safety and efficacy of vibration loading are lacking. The aim of this randomized controlled trial was to assess the musculoskeletal effects of high-frequency loading by means of whole body vibration (WBV) in postmenopausal women. Materials and Methods: Seventy volunteers (age, 58 –74 years) were randomly assigned to a whole body vibration training group (WBV, n ϭ 25), a resistance training group (RES, n ϭ 22), or a control group (CON, n ϭ 23). The WBV group and the RES group trained three times weekly for 24 weeks. The WBV group performed static and dynamic knee-extensor exercises on a vibration platform (35– 40 Hz, 2.28 –5.09g), which mechanically loaded the bone and evoked reflexive muscle contractions. The RES group trained knee extensors by dynamic leg press and leg extension exercises, increasing from low (20 RM) to high (8 RM) resistance. The CON group did not participate in any training. Hip bone density was measured using DXA at baseline and after the 6-month intervention. Isometric and dynamic strength were measured by means of a motor-driven dynamometer. Data were analyzed by means of repeated measures ANOVA. Results: No vibration-related side effects were observed. Vibration training improved isometric and dynamic muscle strength (ϩ15% and ϩ 16%, respectively; p Ͻ 0.01) and also significantly increased BMD of the hip (ϩ0.93%, p Ͻ 0.05). No changes in hip BMD were observed in women participating in resistance training or age-matched controls (Ϫ0.60% and Ϫ0.62%, respectively; not significant). Serum markers of bone turnover did not change in any of the groups. Conclusion: These findings suggest that WBV training may be a feasible and effective way to modify well- recognized risk factors for falls and fractures in older women and support the need for further human studies. J Bone Miner Res 2004;19:352–359. Published online on December 22, 2003; doi: 10.1359/JBMR.0301245 Key words: whole body vibration, mechanical loading, resistance training, osteoporosis INTRODUCTION
cation of osteoporosis. The mortality rate in patients withhip fracture is 12–20% higher than in persons of similar age
AS THE WORLD POPULATION ages, osteoporosis and osteo- and gender who have not suffered a fracture.(2) Of those
porotic fracture occurrence are becoming an increas-
who survive the operative intervention for an osteoporotic
ingly important public health problem.(1) By any measure,
hip fracture, less than one-third are restored to their prefrac-
proximal femoral fracture is the most devastating compli-
ture functional state.(3) Most strategies to treat postmeno-pausal bone loss have been focusing on antiresorptive med-
The authors have no conflict of interest.
ication. More recently, the potential contribution of load-
1Laboratory of Motor Control, Department of Kinesiology, Faculteit Lichamelijke Opvoeding en Kinesitherapie, Katholieke Univer-
siteit, Leuven, Belgium; 2Laboratory of Exercise Physiology and Biomechanics, Department of Kinesiology, Faculteit LichamelijkeOpvoeding en Kinesitherapie, Katholieke Universiteit, Leuven, Belgium; 3Leuven University Center for Metabolic Bone Diseases andDivision of Endocrinology, Katholieke Universiteit, Leuven, Belgium; 4Leuven University Center for Metabolic Bone Diseases andDivision of Geriatric Medicine, Faculty of Medicine, Katholieke Universiteit, Leuven, Belgium. EFFECT OF WHOLE BODY VIBRATION ON BONE DENSITY AND MUSCLE STRENGTH
TABLE 1. BASELINE CHARACTERISTICS OF THE VIBRATION GROUP (WBV), THE RESISTANCE GROUP (RES),
bearing exercise to preserve bone density and prevent
founded by degenerative changes and is highly predictive of
osteoporosis has received some attention. In this regard, a
relatively vigorous aerobic and strength training regimenhas been shown to be most effective.(4) However, this ap-
MATERIALS AND METHODS
proach has the inherent disadvantage of a lack of long-term
compliance and may even increase the risk of fracture.(5) Itis therefore imperative to continue the search for more
Seventy postmenopausal women volunteered to partici-
attractive, low-risk exercise programs, with the goal of
pate in the study. Assessment of eligibility for participation
was based on a screening by questionnaire and a thorough
Recently, Rubin et al.(6) provided evidence in an animal
medical examination. Women had to be between 60 and 70
model that low-risk, high-frequency mechanical accelera-
years of age, non-institutionalized, and free from diseases or
tions may have a strong osteogenic effect. In their study,
medications known to affect bone metabolism or muscle
they observed a dramatic increase of the quality and quan-
strength. Subjects with a total body BMD T-score of less
tity of trabecular bone in sheep when exposed to low-level,
than Ϫ2.5 (the WHO definition for osteoporosis) were also
high-frequency mechanical stimuli. A high-frequency load-
excluded from this study. All subjects were randomly as-
ing regimen applied to ovariectomized rats was effective in
signed to one of the study groups using computer-generated
preventing early post-ovariectomy bone loss.(7) Overall,
random numbers. A total of 25 women were trained for 6
these experiments have given evidence that vibration load-
months on a vibrating platform (WBV group). A group of
ing may have potential for preventing and treating osteopo-
22 woman participated in a resistance training program
rosis. However, in postmenopausal women—who are most
(RES group). Both training programs consisted of 72 train-
at risk of sustaining osteoporotic fractures—the impact of
ing sessions within a 24-week period. Training frequency
this type of approach on bone quality (and, by implication,
was three times a week, with at least 1 day of rest between
potentially on fracture risk) has not been evaluated.
two sessions. A group of 23 age-matched women served as
The aim of this randomized controlled trial was therefore
a control group (CON group) and did not participate in any
to assess musculoskeletal effects of high-frequency whole
training. The baseline characteristics of both groups are
body vibration (WBV) training in postmenopausal women.
indicated in Table 1. All participants gave their informed
Vibration training is increasingly being promoted as a safe
written consent before enrollment, and the study protocol
and efficient training method to improve muscle strength.(8)
was approved by the Leuven University Human Ethics
During a vibration session, the subject stands on a platform
that generates vertical sinusoidal vibrations at a frequency
between 35 and 40 Hz. The mechanical stimuli are trans-mitted to the body, where they load the bone and also
The subjects in the WBV group performed static and
stimulate sensory receptors (most likely muscle spindles).
dynamic knee-extensor exercises on the vibration platform
The activation of these sensory receptors results in reflexive
(PowerPlate, Amsterdam. The Netherlands): squat, deep
activation of motor units similar to the tonic vibration
squat, wide stance squat, one-legged squat, and lunge.
Training load was low at the beginning but progressed
We hypothesized that, in addition to an increase in mus-
slowly according to the overload principle.(11) The training
cle strength caused by vibration-induced muscle activity,
volume increased systematically over the 6-month training
high-frequency loading of the skeleton might improve the
period by increasing the duration of one vibration session,
mechanical competence of the skeleton in postmenopausal
the number of series of one exercise, or the number of
women. BMD of the total hip was selected as primary
different exercises. The training intensity was increased by
endpoint of this trial because the measurement is not con-
shortening the rest periods or by increasing the amplitude
VERSCHUEREN ET AL.
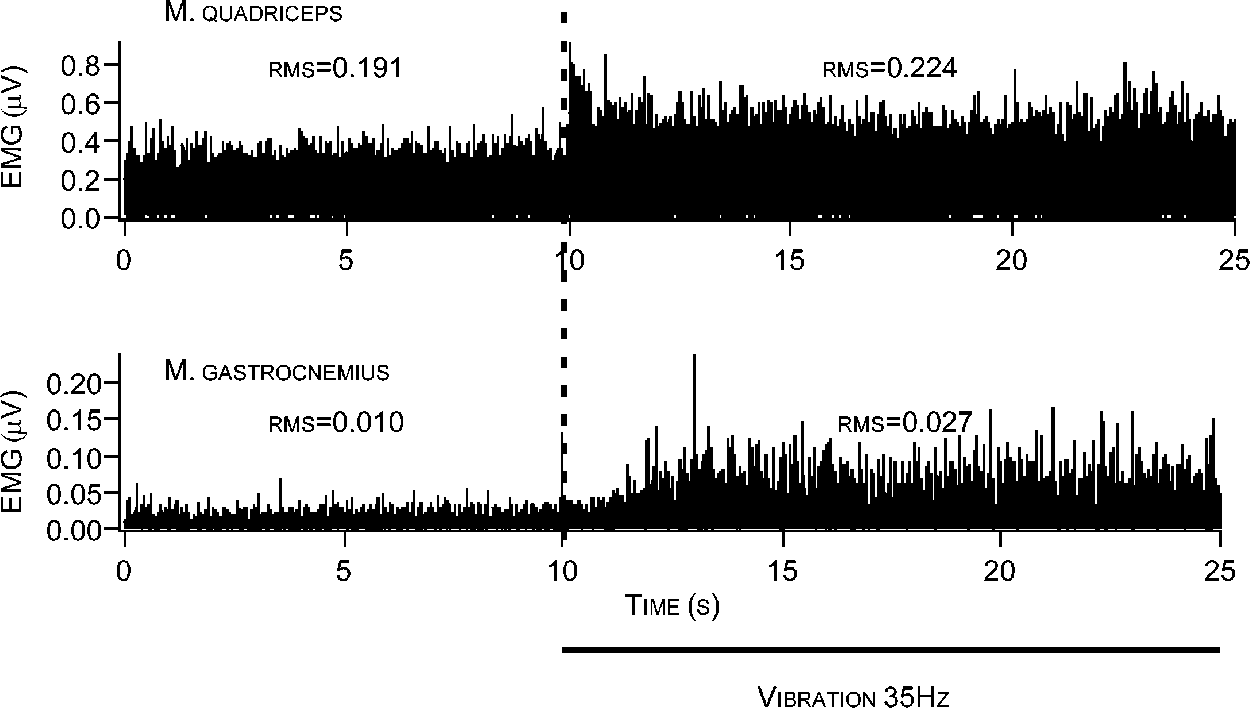
Increased muscle activation in the m.
rectus femoris and the m. gastrocnemius duringvibrating training. RMS is the root mean squareof the rectified EMG in the period without orwith vibration.
(low, 1.7 mm; high, 2.5 mm) and/or the frequency (35– 40
Hz) of the vibration. In addition, training load was increased
Control subjects were instructed to maintain their current
by changing the execution form of the exercises from pre-
level of physical activity during the 24 weeks of the study
dominantly two-legged to one-legged exercises. The dura-
and not to engage in any new form of exercise. The subjects
tion of the WBV program was a maximum of 30 minutes,
completed a questionnaire detailing their physical activity at
which included warming up and cooling down.
the beginning of the study and at monthly intervals there-
The peak acceleration of the sinusoidal vibration
stimulus—as recorded by an accelerometer (MTN 1800;Monitran, Bucks, UK)—varied between 2.28g and 5.09g
(root mean square acceleration between 13.5 and 34.6 m/s2). Of the 5g acceleration, as measured on the platform, only a
At baseline and at 6 months, areal BMD of the total hip
fraction is transmitted through the feet to the hip and spine.
and the total body was assessed by DXA using the QDR-
However, the exact degree of transmissibility is unknown.
4500A device (Hologic, Waltham, MA, USA). Standard
Bipolar surface EMGs (Myosystem 2000; Noraxon, Scotts-
positioning was used, with anterior–posterior scanning of
dale, AZ, USA) recorded from m. rectus femoris and from
the right proximal femur.(14) Lean body mass, fat mass, and
m. gastrocnemius illustrate the impact of the vibration on
percent fat were obtained from the DXA scan of the total
muscle activity (Fig. 1). During the vibration training ses-
body. All scans were performed by the same experienced
sions, the subjects wore similar gymnastic shoes to stan-
technician, who was unaware of the patient’s intervention
dardize the damping of the vibration cause by foot wear.
type. The CV for total hip DXA measurement in our labo-ratory is 0.56%.
The subjects of the RES group trained in the Leuven
University fitness center. They started with a standardized
At baseline and at 6 months, serum osteocalcin and
warm-up consisting of 20 minutes of stepping, running, or
C-telopeptide levels (CTX) were determined as markers of
cycling. The intensity of these cardiovascular exercises was
bone formation and resorption, respectively. At these time
automatically controlled by heart rate (Technogym Sys-
points, fasting blood samples were collected from all indi-
tems, Gambettola, Italy) and systematically increased from
viduals and stored at Ϫ70°C until they were analyzed.
60% to 80% of the heart rate reserve as calculated by the
Circulating osteocalcin was measured using a previously
formula of Karvonen.(12) After the warm-up, the partici-
developed radioimmunoassay (RIA).(15) Serum CTX was
pants performed a resistance training program for knee
assessed by Serum CrossLaps One-Step ELISA (Osteom-
extensors on a leg extension and a leg press machine (Tech-
eter BioTech, Herlev, Denmark) by a method previously
nogym Systems). The resistance training program was de-
signed according to the guidelines of the American Collegeof Sports Medicine (ASCM) for individuals older than 60
years of age: 10 –15 repetitions to the point of volitionalfatigue to elicit improvement in both muscular strength and
The strength of the knee extensors was evaluated on a
endurance.(13) During the first 14 weeks of training, the
motor-driven dynamometer (REV9000; Technogym Sys-
intensity was systematically increased from two sets of 20
tems) by isometric tests and dynamic tests.
repetition maximum (RM) to two sets of 15 RM, two sets of
Isometric strength: The subjects performed a maximal
12 RM, two sets of 10 RM, and finally two sets of 8 RM. In
voluntary isometric contraction of the knee extensors twice.
the last 10 weeks, training volume and training intensity
The knee joint angle was 130°. The isometric contractions
varied between three sets of 12 RM and one set of 8 RM.
lasted 3 s each and were separated by a 2-minute rest
Each RES program lasted for about 1 h in total.
interval. The highest torque (N.m) was recorded as isomet-
EFFECT OF WHOLE BODY VIBRATION ON BONE DENSITY AND MUSCLE STRENGTH
ric strength performance. The CV for isometric strength
TABLE 2. MEAN CHANGES AND BETWEEN-GROUP DIFFERENCES IN
measurement in our laboratory is 3.7%.
MUSCLE STRENGTH, HIP BONE DENSITY, AND BODY COMPOSITION
Dynamic strength: The subjects performed a series of
four consecutive isokinetic flexion– extension movements
against the lever arm of the dynamometer that moved at a
velocity of 100°/s. The knee extension was initiated at a
joint angle of 90° and ended at 160°. After each extension,the leg was returned passively to the starting position from
which the next contraction was immediately initiated. Max-
imal dynamic strength was determined as the peak torque
(N.m) recorded during these series of knee extensions. The
CV for dynamic strength measurement in our laboratory is
Postural sway was measured before and after the 24 week
period using a Bertec force plate connected to a CED Micro1401 data acquisition system and using spike2 software.
Postural sway of each subject was tested under four condi-
tions: quiet stance with vision, quiet stance with vision
occluded by means of liquid-cristal goggles, quiet stance
after a perturbation by a brief voluntary abduction of the
arms to horizontal, and quiet stance after a brief anteflexion
of the arms to horizontal. Postural sway was assessed in the
WBV group and CON group, but not in the RES group.
A one-way ANOVA was used to test for baseline differ-
ences among the WBV group, the RES group, and the CON
group. The effects of the interventions were analyzed by
means of repeated measures ANOVA. After an F value was
found to be significant for the interaction between group and
time, preplanned contrast analyses were performed to eval-
uate significant pre–post changes in each group. A Bonfer-roni correction was used to adjust the p value in relation tothe number of contrasts that were performed. All analyseswere executed using the statistical package Statistica (ver-
significant change was observed (ϩ2.2%; 95% CI, Ϫ1.5–
sion 6; Statsoft, Hamburg, Germany.). The level of signif-
5.9; p ϭ 1.14). Again, both the WBV and RES groups
showed a significant net benefit over time compared withthe CON group (ϩ14.2% and ϩ 8.4%, respectively; p Ͻ
As shown in Fig. 2, total hip BMD increased over time in
No significant differences were observed at baseline be-
the WBV training group (ϩ0.93%; 95% CI, 0.13–1.71; p ϭ
tween the experimental and the control groups in terms of
0.03), whereas no changes in hip BMD were observed in
age, weight, body mass, years since menopause, BMD,
women participating in resistance training or age-matched
serum levels of osteocalcin and CTX, isometric and dy-
controls (Ϫ0.51%; 95% CI, Ϫ1.13 to Ϫ0.11; p ϭ 0.41 and
namic muscle strength, fat mass, or lean body mass (Ta-
Ϫ0.62%; 95% CI, Ϫ1.30–0.07; p ϭ 0.16, respectively).
Compared with the RES group, the 6-month vibration in-
Isometric strength of the knee extensors increased by
tervention resulted in a significant 1.51% net benefit in total
15% (95% CI, 10.6 –19.5; p Ͻ 0.001) in the WBV group
hip BMD (p Ͻ 0.05). A similar net benefit (1.53%, p Ͻ
and by 16% in the RES group (95% CI, 9.1–23.9; p Ͻ
0.01) was observed in comparison with the CON group. The
0.001). In the control group, a nonsignificant decline of 2%
gain in total hip BMD in the WBV group was statistically
was observed (95% CI, Ϫ6.9 –2.01; p ϭ 0.57). Compared
unrelated to the increases in isometric or dynamic strength
with the CON group, the 6-month vibration intervention
(r ϭ Ϫ0.23, p ϭ 0.29 and r ϭ 0.28, p ϭ 0.20, respectively).
resulted in a significant 17.6% net benefit in isometric
Total body BMD and lumbar spine BMD did not change
quadriceps strength (p Ͻ 0.001; Table 2). A similar benefit
over time in any of the groups, and none of the between-
was observed in the RES group (ϩ18.9% versus the CON
group differences were statistically significant. Similarly, no
significant between-group differences were observed in the
Dynamic strength increased by 16.5% (95% CI, 9.4 –
markers of bone remodeling, osteocalcin, and CTX (Table 3).
23.5) and 10.6% (95% CI, 5.6 –15.5) in the WBV group and
The gain in muscle strength in the WBV and RES groups
RES group, respectively (p Ͻ 0.001). In the controls, no
was not associated with a significant change in lean body
VERSCHUEREN ET AL. DISCUSSION
There is increasing evidence that load-bearing represents
a very important functional influence on bone mass.(5) In-creased bone density after loading shows that bone tissueaccommodates to changes in the mechanical environment;this process allows the skeleton to resist the rigors of func-tional activity.(17,18) However, particularly in elderly indi-viduals, strenuous load-bearing exercises may increase therisk for injuries.(19) Moreover, there is evidence that theosteogenic effect of load-bearing may decline with ag-ing.(20) The search therefore continues for alternative strat-egies that make loading less risky and/or may enhance theeffectiveness of the adaptive bone response to loading. Thetraining paradigm presented here might potentially offersuch a strategy for postmenopausal woman, because theresults show that 24 weeks of WBV training—which me-chanically loads the bone and evokes reflexive musclecontractions—was not associated with vibration-related sideeffects and resulted in increased hip BMD. The meanchange in total hip BMD in the WBV group (with a netbenefit of about 1.5% at 6 months compared with controls)is similar in magnitude to the gain in (hip) BMD observedwith antiresorptive agents at the 6-month time point inrecent osteoporosis trials,(21,22) supporting its potential clin-ical relevance. We found no effect of the vibration inter-vention on bone turnover rate, indicating that its positiveimpact on BMD did not result from reduced bone resorp-tion. In line with the lack of significant changes in overallrate of bone turnover, no changes were observed in totalbody or lumbar spine BMD, suggesting that the effects ofvibration on total hip BMD reflect a local (site-specific)loading effect of vibration.
In addition to their gain in BMD, and not unexpectedly,(8)
the subjects in the vibration group showed improved recov-ery of balance after ballistic abduction or anteflexion of thearms and experienced an increase in (isometric and isoki-netic) muscle strength and a decline in fat mass. The
Percent changes across 24 weeks in (A) isometric and dy-
changes in muscle strength were similar in magnitude than
namic muscle strength, (B) total body and total hip BMD, and (C) leanand fat mass in the three experimental groups (WBV, RES, and CON).
those in the resistance training group. The gain in BMDduring the 6-month intervention, however, was statisticallyunrelated to the increases in isometric or dynamic strength,
mass (Table 3). However, in both groups, total fat mass
suggesting that the osteogenic effect was not mediated by
decreased significantly during the intervention period
reflexive muscle contractions. This assumption is supported
(Ϫ2.3%; 95% CI, Ϫ4.3 to Ϫ0.4; p ϭ 0.01 in the WBV
by the fact that the gain in lower limb extension strength in
group and Ϫ3.1%; 95% CI, Ϫ4.9 to Ϫ1.3; p Ͻ 0.001 in the
the resistance training group was not paralleled by a con-
RES group). In contrast, no significant change in fat mass
was observed in the CON group (ϩ0.5%; 95% CI, Ϫ1.3–
Controlled loading studies have indicated that high strain
magnitudes and high strain rates are the most osteo-
The effects of WBV training on postural sway are sum-
genic.(23,24) The loading regimen provided by the WBV
marized in Table 4. Postural sway (rms and peak-to-peak
program in this study combined both. It has been commonly
amplitude) during unperturbed stance with or without vision
assumed that the large amplitude signals inherent to intense
did not change because of WBV training (data not shown).
functional activity define bone morphology.(25) Strain on the
After a fast, brief abduction of the arms, the peak-to-peak
bones increases linearly with increased ground reaction
amplitude of sway in the anterior–posterior direction was
forces.(26) In our study, the ground reaction forces ranged
significantly decreased during the WBV training (p Ͻ 0.05).
between 2.5 times body weight at the start of the program to
Similarly, the peak-to-peak amplitude of sway in medio–
5 times body weight from week 3 onward. The loading of
lateral direction after a brief anteflexion of the arms was
the skeleton during the vibration intervention can therefore
significantly decreased because of WBV training (p ϭ
be considered as a high-strain event of similar impact than
0.05). None of these variables changed across the 24 weeks
activities like basketball, volleyball, and sprinting.(27) In this
regard, the results of this trial are in agreement with previ-
EFFECT OF WHOLE BODY VIBRATION ON BONE DENSITY AND MUSCLE STRENGTH
TABLE 3. MUSCLE STRENGTH, HIP BONE DENSITY, BONE TURNOVER, AND BODY COMPOSITION AT BASELINE AND
*Group-by-time interaction in repeated measures ANOVA on pre–post data. †,‡Significant pre–post difference within group (†p Ͻ 0.05 and ‡p Ͻ 0.01).
ous studies showing positive effects of high-impact exercise
In a very recent well-designed study in young healthy
regimens on bone density.(28) It has been hypothesized that
adults, Torvinen et al.(31) found no effect of WBV training
loading reduces the rate of bone resorption and increases
on mass, structure, and estimated strength of bone. The
bone formation in proportion to the peak strain magni-
authors argued that one reason for this nonresponse could be
tude.(23) However, while we observed an increase in hip
the good basic physical condition of the young subjects,
bone density in the vibration group within 6 months, posi-
with the musculoskeletal tissues of these young adults hav-
tive effects of high-impact exercises on BMD have not even
ing no particular physiological need to adapt to the vibration
been observed within the first year of training.(28)
loading. They suggested that a skeletal response to vibration
It is therefore tempting to speculate that the high fre-
might have been observed in older individuals, as is the case
quency of vibration (35– 40 Hz; i.e., the high strain rate)
in our study. However, as Torvinen et al.(31) indicated as
may have played a key role in the early osteogenic effect
well, the vibration stimulus can be varied in multiple ways
observed in this study. Whereas loads applied at 1 Hz must
(including type, magnitude, frequency, and duration), and
exceed 1000 microstrain to stimulate bone formation,(29)
different types of vibration loading are likely to result in
30-Hz loads only need strains of 50 microstrain to achieve
different effects on bone mass and structure. In their trial,
similar results.(30) Animal research by Rubin et al.(6,17) has
the duration of daily stimulus was only 4 minutes, three to
provided evidence that these low-level, high-frequency me-
five times per week, considerably less than the 20-minute
chanical stimuli may be anabolic to (trabecular) bone. In
stimulus in this study. Their stimulus might have been
their experiments in adult female sheep, histomorphometric
examination of the femur after 1 year of stimulation re-
To date, the mechanism underlying the osteogenic effect
vealed an increase in bone volume per total volume by 32%,
of high-frequency stimuli is not completely understood.
resulting in a 27% improvement in trabecular bone strength.
Rubin et al.(17) hypothesized that the adaptive response of
However, although bone morphology and structure were
the bone to high-frequency stimuli may not be a direct
dramatically being reinforced, no changes were identified
consequence of bone tissue deformation (as during high-
with DXA measurements. This made Rubin et al.(17) con-
impact loading), but may rather be mediated by byproducts
clude that when DXA does identify change, as in our trial,
of the high-frequency strain signal, such as shear stress
the change is likely to be relevant.
arising from fluid flow. Alternatively, the mechanism be-
VERSCHUEREN ET AL.
TABLE 4. POSTURAL SWAY (PEAK-TO-PEAK) RECOVERY AFTER
a significant increase in (total hip) BMD from baseline in
ABDUCTION OR ANTEFLEXION OF THE ARMS AT BASELINE AND AFTER
the vibration group and significant between-group differ-
ences, we acknowledge that the number of observations was
small. As indicated, we can only speculate about the mech-
anisms underlying the increase in BMD and the extent to
which this increase reflects differential effects on cortical
and trabecular bone. Many questions remain as to whetherthese short-term effects would persist over time and as to
how the training protocol can be further optimized in terms
of osteogenic effects. We selected a training program on the
vibration platform that was likely to have positive effects on
muscle and bone tissue. It is possible that high-frequency or
even broad-frequency vibration at a lower strain amplitude,
superimposed with some larger strains at intermittent inter-
vals, might be more osteogenic (but at the expense of gain
in strength). Also, our results may not be generalizable
because the participants were healthy volunteers and not a
random sample of the general older population. Finally, the
usefulness and safety of this type of training in the long-
*Group-by-time interaction in repeated ANOVA on pre–post data.
term prevention of postmenopausal osteoporosis and osteo-
†Significant pre–post difference within group ( p Ͻ 0.05).
porotic fracture occurrence remain unknown.
In conclusion, in healthy postmenopausal women, a 24-
week whole body vibration program is feasible and able to
hind the frequency-dependent adaptive response of bone to
modify muscle strength, balance, and hip bone density,
loading might be the so-called stochastic resonance. Sto-
which are well-recognized risk factors for hip fracture.(10)
chastic resonance is a phenomenon in which mechanical
Future human studies are needed to confirm these short-
noise (broad-band frequency of vibration) enhances the
term findings and further explore the potential of vibration
response of a nonlinear system to a weak signal by boosting
loading for preventing and treating osteoporosis.
it over a threshold. Previous studies have shown that sto-chastic resonance can enhance the mechanosensitivity of
ACKNOWLEDGMENTS
different mechanoreceptors in our body, like the musclespindles.(32) Recent in vitro and in vivo evidence suggests
SB is a core member of the ASBMR Working Group on
that (cortical) bone formation in response to mechanical
Musculoskeletal Rehabilitation. The authors thank all the
loading can be enhanced by adding noise to a (high-impact)
participants for taking part in this study. They also thank G
exercise regimen.(33,34) Tanaka et al.(33) showed that a vi-
Van der Meer, J Tempelaars, and N De Poot for help in
bratory stimulus added to a low-frequency, high-amplitude
designing the training program; Drs E Van den Eede and K
strain enhances the osteogenic response of the strain by
Pardaens for the medical screening of the subjects; and H
almost 4-fold. In the present trial, we applied both a large-
Borghs and H Peeters for conducting the DXA measure-
amplitude strain and a high-frequency vibratory stimulus.
ments. This study was supported by Grant G.0171.03 from
Stochastic resonance may therefore have contributed to the
(F.W.O.-Vlaanderen) to SB. SMPV is a postdoctoral fellow
In certain professions (e.g., tractor drivers, pilots, etc.) a
of the Fund for Scientific Research-Flanders, Belgium. SB
(potential) association has been observed between long-
and DV are senior clinical investigators of the Fund for
term exposure to WBV and chronic lower back pain.(35)
Scientific Research-Flanders, Belgium. SB is holder of the
However, evidence in favor of a dose–response association
Leuven University Chair in Metabolic Bone Diseases, sup-
is weak, and it remains to be clarified whether there is a
causal link between work-related WBV and low back pain. As indicated, we observed no vibration-related side effects. REFERENCES
In particular, low back pain or other symptoms or injuries
1. Kannus P, Parkkari J, Niemi S 1995 Age-adjusted incidence of hip
did not occur. Our short-term findings are in line with those
fractures. Lancet 346:50 –51.
previously reported by Rittweger et al.,(36) who recently
2. Autier P, Haentjens P, Bentin J, Baillon JM, Grivegnee AR,
even performed a randomized controlled trial to compare
Closon MC, Boonen S 2000 Costs induced by hip fractures: Aprospective controlled study in Belgium. Belgian Hip Fracture
lumbar extension exercise and WBV exercise for the treat-
Study Group. Osteoporos Int 11:373–380.
ment of chronic lower back pain.(37) Nevertheless, we ac-
3. Magaziner J, Simonsick EM, Kashner TM, Hebel JR, Kenzora JE
knowledge that the lack of safety concerns in the context of
1990 Predictors of functional recovery one year following hospital
a 6-month trial in healthy volunteers does not exclude the
discharge for hip fracture: A prospective study. J Gerontol 45: M101–M107.
potential for long-term side effects in unselected elderly
4. Gutin B, Kasper MJ 1992 Can vigorous exercise play a role in
individuals. Research is needed to further address the long-
osteoporosis prevention? A review. Osteoporos Int 2:55– 69.
term safety of WBV training in older women.
5. Lanyon LE 1996 Using functional loading to influence bone mass
and architecture: Objectives, mechanisms, and relationship with
Our study has limitations, and the results should be in-
estrogen of the mechanically adaptive process in bone. Bone
terpreted in the context of its design. Although we observed
18(Suppl 1):37S– 43S. EFFECT OF WHOLE BODY VIBRATION ON BONE DENSITY AND MUSCLE STRENGTH
6. Rubin C, Turner AS, Muller R, Mittra E, McLeod K, Lin W, Qin
ficacy With Risedronate Therapy (VERT) Study Group. JAMA
YX 2002 Quantity and quality of trabecular bone in the femur are
282:1344 –1352.
enhanced by a strongly anabolic, noninvasive mechanical interven-
23. Rubin CT, Lanyon LE 1985 Regulation of bone mass by mechan-
tion. J Bone Miner Res 17:349 –357.
ical strain magnitude. Calcif Tissue Int 37:411– 417.
7. Flieger J, Karachalios T, Khaldi L, Raptou P, Lyritis G 1998
24. Turner CH, Owan I, Takano Y 1995 Mechanotransduction in bone:
Mechanical stimulation in the form of vibration prevents post-
Role of strain rate. Am J Physiol 269:E438 –E442.
menopausal bone loss in ovariectomized rats. Calcif Tissue Int
25. Frost HM 1990 Skeletal structural adaptations to mechanical usage
63:510 –514.
(SATMU): 1. Redefining Wolff’s law: The bone modeling prob-
8. Delecluse C, Roelants M, Verschueren S 2003 Strength increase
lem. Anat Rec 226:403– 413.
after whole-body vibration compared with resistance training. Med
26. Bassey EJ, Littlewood JJ, Taylor SJ 1997 Relations between com-
Sci Sports Exerc 35:1033–1041.
pressive axial forces in an instrumented massive femoral implant,
9. Burke D, Schiller HH 1976 Discharge pattern of single motor units
ground reaction forces, and integrated electromyographs from vas-
in the tonic vibration reflex of human triceps surae. J Neurol
tus lateralis during various ’osteogenic’ exercises. J Biomech 30:
Neurosurg Psychiatry 39:729 –741.
10. Cummings SR, Nevitt MC, Browner WS, Stone K, Fox KM,
27. Groothausen J, Siemer H, Kemper HCG, Twisk J, Welten DC 1997
Ensrud KE, Cauley J, Black D, Vogt TM 1995 Risk factors for hip
Influence of peak strain on lumbar bone mineral density: An
fracture in white women. Study of Osteoporotic Fractures Re-
analysis of 15-year physical activity in young males and females.
search Group. N Engl J Med 332:767–773.
Pediatr Exerc Sci 9:159 –173.
11. American College of Sports Medicine 2000. Exercise prescription.
28. Heinonen A, Kannus P, Sievanen H, Oja P, Pasanen M, Rinne M,
In: Franklin BA, Whaley MH, Howley ET (eds.) ACSM’s Guide-
Uusi-Rasi K, Vuori I 1996 Randomised controlled trial of effect of
lines for Exercise Testing and Prescription. Lippincott Williams
high-impact exercise on selected risk factors for osteoporotic frac-
and Wilkins, Philadelphia, PA, USA, pp. 138 –139.
tures. Lancet 348:1343–1347.
12. Karvonen M, Kentala K, Mustala O 1957 The effects of training on
29. Rubin CT, Lanyon LE 1987 Kappa Delta Award paper. Osteo-
heart rate: A longitudinal study. Ann Med Experimentalis et Bio-
regulatory nature of mechanical stimuli: Function as a determinant
logiae Fenniae 35:307–315.
for adaptive remodeling in bone. J Orthop Res 5:300 –310.
13. American College of Sports Medicine 1998 American College of
30. Qin YX, Rubin CT, McLeod KJ 1998 Nonlinear dependence of
Sports Medicine Position Stand. Exercise and physical activity for
loading intensity and cycle number in the maintenance of bone
older adults. Med Sci Sports Exerc 30:992–1008.
mass and morphology. J Orthop Res 16:482– 489.
14. Boonen S, Rosen C, Bouillon R, Sommer A, McKay M, Rosen D,
31. Torvinen S, Kannus P, Sievanen H, Jarvinen TA, Pasanen M,
Adams S, Broos P, Lenaerts J, Raus J, Vanderschueren D, Geusens
Kontulainen S, Nenonen A, Jarvinen TL, Paakkala T, Jarvinen M,
P 2002 Musculoskeletal effects of the recombinant human IGF-I/
Vuori I 2003 Effect of 8-month vertical whole body vibration on
IGF binding protein-3 complex in osteoporotic patients with prox-
bone, muscle performance, and body balance: A randomized con-
imal femoral fracture: A double-blind, placebo-controlled pilot
trolled study. J Bone Miner Res 18:876 – 884.
study. J Clin Endocrinol Metab 87:1593–1599.
32. Cordo P, Inglis JT, Verschueren S, Collins JJ, Merfeld D, Rosen-
15. Bouillon R, Vanderschueren D, Van Herck E, Nielsen HK, Bex M,
blum S, Buckley S, Moss F 1996 Noise in human muscle spindles.
Heyns W, Van Baelen H 1992 Homologous radioimmunoassay of
Nature 383:769 –770.
human osteocalcin. Clin Chem 38:2055–2060.
33. Tanaka SM, Alam IM, Turner CH 2003 Stochastic resonance in
16. Rosenquist C, Fledelius C, Christgau S, Pedersen BJ, Bonde M,
osteogenic response to mechanical loading. FASEB J 17:313–314.
Qvist P, Christiansen C 1998 Serum CrossLaps One Step ELISA.
34. Tanaka SM, Li J, Duncan RL, Yokota H, Burr DB, Turner CH
First application of monoclonal antibodies for measurement in
2003 Effects of broad frequency vibration on cultured osteoblasts.
serum of bone-related degradation products from C-terminal te-
J Biomech 36:73– 80.
lopeptides of type I collagen. Clin Chem 44:2281–2289.
35. Lings S, Leboeuf-Yde C 2000 Whole-body vibration and low back
17. Rubin C, Turner AS, Mallinckrodt C, Jerome C, McLeod K, Bain
pain: A systematic, critical review of the epidemiological literature
S 2002 Mechanical strain, induced noninvasively in the high-
1992–1999. Int Arch Occup Environ Health 73:290 –297.
frequency domain, is anabolic to cancellous bone, but not cortical
36. Rittweger J, Beller G, Felsenberg D 2000 Acute physiological
bone. Bone 30:445– 452.
effects of exhaustive whole-body vibration exercise in man. Clin
18. Wolff J 1986 The law of bone remodeling. In: Maquet P, Furlong
Physiol 20:134 –142.
R (eds.) Bone Remodeling. Springer Verlag, Berlin, Germany.
37. Rittweger J, Just K, Kautzsch K, Reeg P, Felsenberg D 2002
19. Kallinen M, Markku A 1995 Aging, physical activity and sports
Treatment of chronic lower back pain with lumbar extension and
injuries. An overview of common sports injuries in the elderly.
whole-body vibration exercise: A randomized controlled trial.
Sports Med 20:41–52.
Spine 27:1829 –1834.
20. Turner CH, Takano Y, Owan I 1995 Aging changes mechanical
loading thresholds for bone formation in rats. J Bone Miner Res 10:1544 –1549.
21. Ettinger B, Black DM, Mitlak BH, Knickerbocker RK, Nickelsen
T, Genant HK, Christiansen C, Delmas PD, Zanchetta JR, Stakke-
stad J, Gluer CC, Krueger K, Cohen FJ, Eckert S, Ensrud KE,
Leuven University Center for Metabolic Bone Diseases
Avioli LV, Lips P, Cummings SR 1999 Reduction of vertebralfracture risk in postmenopausal women with osteoporosis treated
Universitaire Ziekenhuizen K.U. Leuven
with raloxifene: Results from a 3-year randomized clinical trial.
Multiple Outcomes of Raloxifene Evaluation (MORE) Investiga-
tors. JAMA 282:637– 645.
22. Harris ST, Watts NB, Genant HK, McKeever CD, Hangartner T,
E-mail: steven.boonen@uz.kuleuven.ac.be
Keller M, Chesnut CH III, Brown J, Eriksen EF, Hoseyni MS,Axelrod DW, Miller PD 1999 Effects of risedronate treatment onvertebral and nonvertebral fractures in women with postmeno-
Received in original form July 9, 2003; in revised form October 8,
pausal osteoporosis: A randomized controlled trial. Vertebral Ef-
Antibiotics Improve Survival in Severe Malnutrition Oral antibiotics amoxicillin and cefdinir show efficacy in a randomized study of children with severe acute malnutrition. Linda MacArthur, PhD February 14, 2013—In children with severe acute malnutrition, a one week course of amoxicillin or cefdinir, combined with ready-to-use therapeutic food (RUTF), improved nutritional recovery and
Effects of Initiating Insulin and Metformin on Glycemic Control and Inflammatory Biomarkers Among Patients With Type 2 Diabetes The LANCET Randomized Trial Context As diabetes is in part an inflammatory condition, the initiation of insulin and/or metformin may beneficially reduce levels of inflammatory biomarkers such as high-sensitivity C-reactive protein (hsCRP). Objective To determine
 VERSCHUEREN ET AL.
VERSCHUEREN ET AL.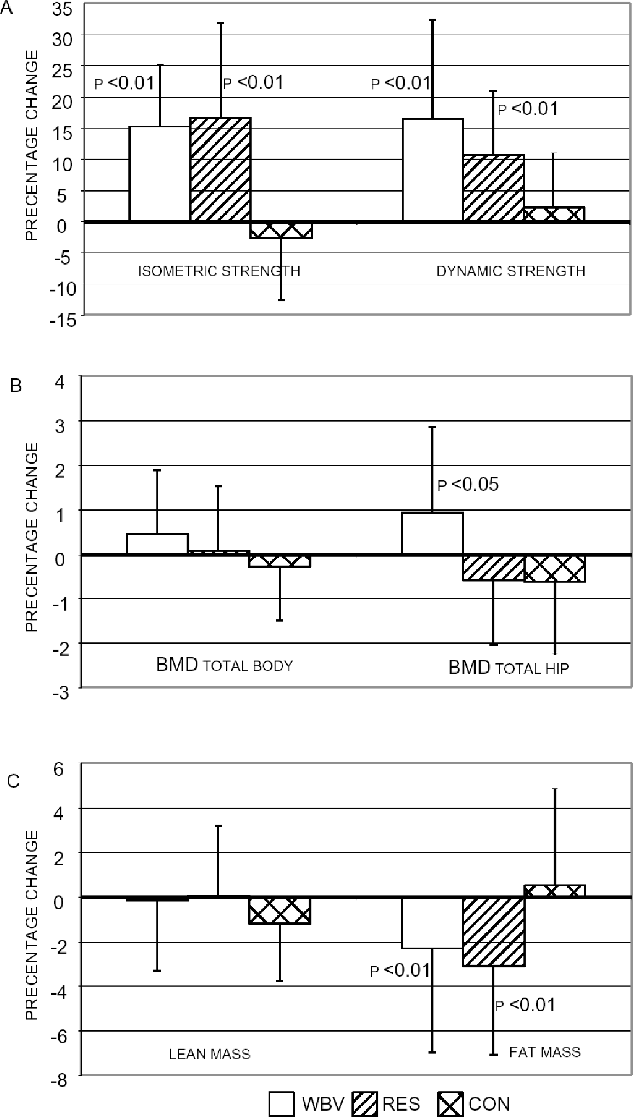 VERSCHUEREN ET AL.
VERSCHUEREN ET AL.