Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
Doi:10.1016/j.maturitas.2005.02.018
Breast cancer risk in the WHI study: The problem of obesity
Department of Gynecology and Obstetrics, J. W. Goethe University of Frankfurt, Theodor-Stern-Kai 7,D-60590 Frankfurt am Main, GermanyAbstract
In the climacteric, about 40% of the women have occult breast tumors the growth of which may be stimulated by hormones.
Many genetic, reproductive and lifestyle factors may influence the incidence of breast cancer. Epidemiological data suggestthat the increase in the relative risk (RR) of breast cancer induced by hormone replacement therapy (HRT) is comparable withthat associated with early menarche, late menopause, late first birth, alcohol consumption, etc. One of the most important riskfactors is obesity which exceeds the effect of HRT by far, and in overweight postmenopausal women the elevated risk of breastcancer is not further increased by HRT. As in the WHI study the majority of women was overweight or obese, this trial wasunsuitable for the investigation of breast cancer risk. In the women treated with an estrogen/progestin combination, the RR ofbreast cancer rose only in those women who have been treated with hormones prior to the study, suggesting a selection bias. In the women not pretreated with hormones, it was not elevated. In the estrogen-only arm of the WHI study, there was noincrease but a steady decrease in the RR of breast cancer during 6.8 years of estrogen therapy. This result was unexpected, asestrogens are known to facilitate the development and growth of breast tumors, and the effect is enhanced by the addition ofprogestins.
Obese women are at high risk to develop a metabolic syndrome including insulin resistance and hyperinsulinemia. In post-
menopausal women, elevated insulin levels are not only associated with an increased risk for cardiovascular disease, but alsofor breast cancer. This might explain the effects observed in both arms of the WHI study: HRT with relative low doses ofestrogens may improve insulin resistance and, hence, reduce the elevated breast cancer risk in obese patients, whereas thisbeneficial estrogen effect may be antagonized by progestins. The principal options for the reduction of breast cancer risk inpostmenopausal women are the prevention of overweight and obesity to avoid the development of hyperinsulinemia, the medicaltreatment of insulin resistance, the use of low doses of estrogens and the reduction of exposure to progestins. The latter mightinclude long-cycles with the sequential use of appropriate progestins every 3 months for 14 days. There are large inter-individualvariations in the proliferative response to estrogens of the endometrium. Control by vaginalsonography and progestin challengetests may help to identify those women who may be candidates for low-dose estrogen-only therapy. 2005 Elsevier Ireland Ltd. All rights reserved. Keywords: Breast cancer risk; Postmenopause; Obesity; Hyperinsulinemia; Hormone replacement therapy
∗ Tel.: +49 69 6301 5692; fax: +49 69 6301 5522. E-mail address: h.kuhl@em.uni-frankfurt.de.
0378-5122/$ – see front matter 2005 Elsevier Ireland Ltd. All rights reserved. H. Kuhl / Maturitas 51 (2005) 83–971. Introduction
and BRCA2) must be accepted as an unchangeablepredisposition. Many other risk factors, e.g., obesity
Breast cancer is the most frequent malignant dis-
or hormone replacement therapy (HRT) can, how-
ease in Western countries and seems to be dependent
ever, be avoided or changed. Early menarche and late
on lifestyle and nutrition. The development of breast
menopause indicate a prolonged exposition to estro-
cancer is usually regarded as a multifactorial process
gens and progesterone that increase the risk of breast
which means that the etiology is unknown. There are
cancer, whereas long-term lactation decreases the risk
many theories that are based on experimental investi-
gation and relatively inconsistent epidemiological data.
sion of ovulation during breastfeeding. Moreover, the
There is, however, no doubt that reproductive factors
Nurses’ Health Study showed that irregular cycles in
play an important role. Concerning the impact of sex
young women are associated with a reduced life-time
steroids, the cumulative exposure to endogenous and
breast cancer risk As in anovulatory cycles there
exogenous estrogens and progestins seems to deter-
is generally no estrogen deficiency, it may be assumed
mine the life-time risk of breast cancer.
that the protective effect of anovulation is associatedwith the lack of progesterone. Obesity, insulin resis-tance, disorders of lipid metabolism and elevated alco-
2. Risk factors for the development of breast
hol consumption seem to increase breast cancer risk.
The impact of long-term shift work is possibly relatedto the prolonged light exposure at night resulting in
Certain risk factors for the development of breast
a suppression of melatonin levels, while the cumula-
cancer like age and gene mutation (e.g., BRCA1
tive association of use of antibiotics with the risk ofbreast cancer might reflect a weakened immune func-tion (
Table 1Risk factors for the development of breast cancer
3. Breast cancer risk and HRT: epidemiological
Many observational studies on the influence of HRT
on breast cancer risk revealed contradictory results,
and every new case-control study or cohort study will
enlarge this long row of inconsistent outcomes. The
collaborative reanalysis from 1997 was an attempt to
bring together and re-examine the individual data of all
relevant studies published so far. It revealed that each
year of delayed menopause increases the risk by 2.8%
which was in the range of 2.3% for each year of HRT
relative risk of breast cancer increased by 35%
in postmenopausal women who had used HRT for 11
years on average. The cumulative excess of breast can-
cers diagnosed between the ages of 50 and 70 years
per 1000 women who began HRT at age 50 and used
it for 5, 10, and 15 years, were estimated to be 2, 6,
and 12 cases. Within 5 years after discontinuation of
treatment, the elevated risk has returned to baseline
H. Kuhl / Maturitas 51 (2005) 83–97
relative risk of breast cancer by 24%, but only in thosewomen who were pretreated with hormones prior to the
Randomised placebo-controlled trials are regarded
start of the WHI study ver, that arm of the
as the non-plus-ultra for the investigation of the im-
WHI study which investigated the effect of CEE alone
pact of drugs on disease risk. Therefore, the results of
in hysterectomized women, revealed a highly surpris-
the HER study and both arms of the WHI study were
ing result: after 6.8 years of treatment the relative risk
of breast cancer was 0.77 ven though the result
ever, whether the group of women investigated in these
narrowly missed statistical significance, the consistent
studies, reflects those women who normally receive
time course of the Kaplan–Meier estimates suggests
HRT. In the WHI study and the HER study the partic-
that the estrogen therapy had a protective effect
ipating women were selected as to suffer not from cli-macteric symptoms. Consequently, their mean age was
3.3. Effect of different regimens of hormone
very high (about 63 years) and a high proportion of the
women was obese (35–45% had a BMI ≥ 30 kg/m2). As obesity is associated not only with an elevated risk
In the collaborative reanalysis the type of HRT was
for developing a metabolic syndrome and coronary
known for about 40% of the users: 80% of them were
heart disease, but also with an increased risk of breast
treated with conjugated estrogens and only 12% with
cancer, the results may be rather questionable.
estrogen/progestin combinations. The relative risk of
The HER study on the secondary prevention of
breast cancer was found to be 1.34 in women treated
coronary heart disease by continuous treatment with
for ≥5 years with estrogens alone and 1.53 in women
0.625 mg conjugated equine estrogens and 2.5 mg
treated for ≥5 years with estrogen/progestin combina-
medroxyprogesterone acetate (CEE/MPA), observed
tions. There was no difference in risk between the dose
a non-significant 27% increase in the relative risk of
of ≤0.625 mg and ≥1.85 mg conjugated estrogens
breast cancer after 6.8 years In the WHI study
The Million Women Study (MWS) reported on an in-
5.2 years of treatment with CEE/MPA increased the
crease in breast cancer risk by 30% using estrogens
Table 2Relative risk (RR) of breast cancer during replacement therapy with estrogens only (ERT) or estrogen/progestin combinations (HRT)
a Continuous combined estrogen/progestin therapy. b Sequential or continuous combined estrogen/progestin therapy. H. Kuhl / Maturitas 51 (2005) 83–97
alone and by 100% using estrogen/progestin combi-
gen/progestin combinations increased the frequency
nations The results may, however, be impaired
of estrogen receptor-positive (ER+) and progesterone
by detection bias, as, e.g., within 1 year after the first
receptor-positive (PR+) invasive breast cancers 2- to
mammographic screening the number of breast cancer
2.5-fold, whereas the effect on receptor-negative car-
diagnoses (interval cancers) had increased three-fold in
postmenopausal women treated continuously with es-
of hormones was associated with a higher incidence of
trogen/progestin combinations since several years. The
tumors with the low malignancy grade1 anal-
MWS did not find any difference in the risk of breast
ysis of data from the Nurses’ Health Study revealed that
cancer regarding type and dose of estrogens, route of
postmenopausal women who used HRT had a higher
administration, type of progestins, or sequential or con-
probability of developing ER+ and PR+ tumors, and
a higher body mass index (BMI) was associated with
During the last years evidence has accumulated
that the increase in breast cancer risk is relatively lowduring use of unopposed estrogens, and is consider-ably enhanced by the addition of progestins (
4. The role of sex steroids in the development of breast cancer
control study which found the highest risk with estro-gen only
4.1. Effect of sex steroids on the proliferation of
A qualitative review showed the inconsistency of
normal and malignant breast tissue
results of observational studies, and most of the cohortstudies were not associated with a significant increase
Although estrogens may be involved in the initia-
in risk Recent studies confirmed the elevated
tion of breast cancer, a carcinogenic/mutagenic role of
breast cancer risk using estrogen/progestin combina-
sex steroids is rather improbable. The available exper-
tions. According to the data of the Nurses’ Health
imental, clinical and epidemiological data suggest that
Study, the use of unopposed estrogens increases the risk
the development of breast cancer is closely related to
of breast cancer by 23% and of estrogen/progestin com-
an accelerated hormone-induced growth of preexisting
binations by 67% The randomised, double-blind,
occult tumors. In an autopsy study, small occult breast
placebo-controlled Womens’s Health Study revealed
cancers were found in 39% of women aged 40–50
no increase in risk using estrogens alone or sequential
years Epidemiological studies revealed that the
estrogen/progestin combinations, but a significant 82%
impact of estrogens on the relative risk of breast cancer
increase in women treated with continuous combined
is modest, but considerably enhanced by the addition
estrogen/progestin preparations Three Scandi-
of progestins. This corresponds to the proliferative ef-
navian cohort studies revealed a considerably higher
fects both on normal mammary epithelium and breast
relative risk in women treated with estrogen/progestin
cancers of estrogens which is enhanced by the pres-
ence of MPA or progesterone. The mitosis rate of both
ER+/PR+ and ER−/PR− carcinoma was higher in theluteal phase than in the follicular phase ,
3.4. Histological types and receptor status of
the mitosis rate of healthy breast epithelium was high-
est in the luteal phase, and higher during treatmentof postmenopausal women with CEE/MPA as com-
In most studies continuous combined HRT was as-
sociated with the highest relative risk of breast can-
CEE/MPA were observed in the monkey model
cer, particularly of hormone receptor-positive carci-
In contrast, neither ethinylestradiol plus norethisterone
noma. While the use of estrogens alone was as-
nor tibolone had a significant effect on the proliferation
sociated with no or a slightly elevated risk, estro-
of normal breast epithelium ven though both
gen/progestin combinations increased the incidence of
tibolone and all types of estrogen/progestin combina-
lobular cancers to a much greater extent than that of
tions were found to be associated with an increased risk
H. Kuhl / Maturitas 51 (2005) 83–97
tionable whether the effects of different HRT prepara-
mutations of ER− stem cells may cause the
tions on healthy mammary epithelium reflect those on
differentiation of a subset of cells into ER+ cells. These
tumors contain ER+ and ER− cells and may transito-rily respond to HRT and antiestrogens, but would not
4.2. Regulation of growth in benign and malignant
have lasting effects, because proliferation of ER− cells
continues. Therefore, HRT should not increase signif-icantly the risk of this subtype of breast cancer
There are profound differences between healthy
A third subtype may arise through transformation of
and malignant breast tissue concerning the hormone-
ER+ progenitor cells and consists of more differenti-
dependent regulation of mitoses. In the resting normal
ated cells. Their growth may be slowed down by treat-
mammary tissue ER␣ and PR are expressed in very
ment with antiestrogens and accelerated during HRT,
few epithelial cells, while ER is present in 70%
and in both cases this subtype has the best prognosis
of the cells. Those 2% of epithelial cells which are
proliferating, do not contain ER The mitosesare probably controlled by paracrine interactionsof adjacent epithelial cells containing ER␣ and PR,
5. Interference of overweight with HRT
while ER was suggested to inhibit ER␣-induced
concerning breast cancer risk
effects. The effect of progesterone on proliferationand differentiation of the mammary epithelium is
5.1. Relation between breast cancer risk and body
primarily dependent on the PRB, whereas PRA has a
negative effect on PRB, and overexpression of PRAmay reflect a more aggressive state
Obesity is associated not only with an elevated risk
While in healthy tissue ER␣ is expressed only in
of developing coronary heart disease, but also with an
resting cells, the transition of benign to malignant mam-
increase in risk of various cancers Moreover,
mary tissue is characterized by a switch from paracrine
there is a highly significant association between the risk
to autocrine regulation of epithelial cell proliferation
of breast cancer and BMI, % body fat and weight gain
by sex steroids, i.e., in breast tumors ER␣ and PRs
are expressed also in proliferating cells The
Epidemiological data suggest that a high BMI may
development of breast cancer is closely related to the
attenuate the effect of estrogens on breast cancer risk.
function of the normal, slow dividing, long living,
The collaborative reanalysis from 1997 found an asso-
undifferentiated stem cells which have both a highly
ciation between body mass index (BMI) and the rela-
proliferative potential and the ability to differentiate
tive risk of breast cancer, increasing by 3.1% per kg/m2
Long-term exposure to genotoxic agents may
Moreover, the relative breast cancer risk associ-
cause mutations resulting in the formation of breast
ated with HRT decreased progressively with increasing
cancer stem cells/progenitor cells. They can either lose
weight or BMI. It was 1.73 in postmenopausal women
their steroid receptors and become rapidly proliferat-
with a BMI below 22.5 kg/m2 and 1.02 for BMI of
ing ER− cells or they become ER+ progenitor cells
which proliferate and in addition stimulate growth of
to increase the risk of breast cancer only in women
ER− cells by producing paracrine factors The
with a BMI of less than 24.5 kg/m2 In the Nurses
better prognosis of ER+ breast tumors and the more
Health Study, the risk of breast cancer correlated with
aggressive behaviour of ER− tumors as well as the
the BMI in postmenopausal women without HRT, but
effect of HRT on these subtypes are associated with
their origin. ER␣ and ER are expressed in 60–75%
It is well known that an increase in caloric uptake
and energy expenditure leads to a stimulation of
ER− tumors which arise from the most primitive
adrenal androgen secretion, a decrease in SHBG
ER− stem/early progenitor cells, are poorly differenti-
and an elevated aromatisation of androgens in the
ated, more aggressive, and have a poor prognosis. Their
excessive fat tissue. A significant correlation between
growth is neither influenced by HRT nor by SERMs
the serum levels of total and free estradiol and the
H. Kuhl / Maturitas 51 (2005) 83–97
characterized by hypertension, coronary heart disease,
Association between risk of breast cancer and obesity-related factors
dyslipidemia, insulin resistance and hyperinsulinemia
Recent investigations suggest that it is in all
Breast cancer risk is elevated in obese postmenopausal
probability the elevated insulin level in obese post-
menopausal women which is responsible for the in-
At very low serum concentrations breast cancer risk corre-
creased risk of breast cancer. A specific protein secreted
HRT does not increase risk of breast cancer in obese post-
by adipocytes, adiponectin, correlates with insulin sen-
sitivity. Low levels of adiponectin which precede a de-
Breast cancer risk correlates with body mass index
crease in insulin sensitivity, are closely and inversely
Breast cancer risk correlates with % body fat
associated with insulin resistance and hyperinsuline-
Breast cancer risk correlates with weight gainPrevalence of metabolic syndrome is elevated in obese
mia In postmenopausal women a significant in-
verse relation between serum adiponectin and breast
Insulin resistance and hyperinsulinemia increase breast can-
cancer risk was observed, whereas in premenopausal
Serum level of C-peptide correlates with risk of mammary
has been suggested to be associated with breast cancer
Serum level of adiponectin correlates with insulin sensitivity
risk in premenopausal women, but in postmenopausal
Serum level of adiponectin correlates negatively with body
women no relation between breast cancer risk and the
levels of IGF-1 was found significant cor-
Serum level of adiponectin correlates negatively with insulin
relation of the levels of C-peptide with the occurrence
of epithelial hyperplasia of the breast or breast can-
Serum level of adiponectin correlates negatively with breast
cer suggests a key role of elevated insulin levels in
Estrogen replacement therapy reduces fasting insulin and in-
the growth of breast cancer in postmenopausal women
Postmenopausal patients, but not premenopausal
Estrogen/progestin reduces incidence of diabetes mellitus in
women with type 2 diabetes had a 16% higher breast
cancer risk than women without diabetes (
Estrogen replacement therapy reduces risk of breast cancer
The lack of an association between breast cancer
risk and hyperinsulinemia in premenopausal womensuggests a modulatory role of sex steroids.
risk of breast cancer in postmenopausal women has
Low doses of estrogens have been demonstrated to
been reported. At estradiol levels of above 8 pg/ml
improve insulin sensitivity in postmenopausal women
the risk was three times higher than that at levels
and to reduce elevated fasting insulin levels, while
below 5 pg/ml, and at levels of above 11 pg/ml it was
higher estrogen levels or the use of more potent es-
five times higher than that at levels below 8 pg/ml
trogens may decrease insulin sensitivity. The addition
Correlations do not imply causality, and it
of progestins may decrease insulin sensitivity, possibly
seems rather improbable that such large differences in
by reducing insulin binding to the insulin receptor and
breast cancer risk are due to such small differences in
the estradiol levels. There must be an additional risk
Treatment of non-obese postmenopausal women
factor associated with obesity, e.g., insulin resistance
with 0.625 mg CEE improved insulin sensitivity by
and hyperinsulinemia, which is influenced by sex
25%, whereas 1.25 mg CEE caused a decrease by 25%.
steroids and might be involved in the development of
The sequential addition of 10 mg MPA antagonized
the beneficial effect of 0.625 mg CEE and caused an18% decrease in insulin sensitivity Treatment of
5.2. Hyperinsulinemia and breast cancer risk
postmenopausal women with estrogen-only reducedfasting insulin by 35%, while estrogen/progestin
The prevalence of insulin resistance and hyperin-
combinations were less effective PEPI study
sulinemia increases with age, BMI and estrogen de-
revealed that treatment of postmenopausal women with
ficiency Obese postmenopausal women are at
0.625 mg CEE with or without additional progestins led
a high risk to develop a metabolic syndrome that is
to a reduction in fasting insulin and glucose levels
H. Kuhl / Maturitas 51 (2005) 83–97
In postmenopausal women with impaired glucose tol-
erance continuous combined treatment with 0.625 mg
Baseline characteristics of the volunteers participating in the WHIstudy
CEE and 2.5 mg MPA reduced insulin resistance andfasting glucose levels, while in women with normal glu-
cose tolerance the levels of fasting insulin and glucose
were decreased increase in the postchallenge
glucose concentrations during OGTT that was ob-
served in postmenopausal women under HRT, might
be caused by a delayed insulin response to glucose and
an increased insulin clearance in the liver
It was observed in the WHI study that treatment of
postmenopausal women with CEE/MPA for 5.6 years
on average caused a significant decrease in the inci-
dence of diabetes mellitus by 21%. This was probably
mediated by a decrease in insulin resistance, as already
after 1 year of treatment fasting glucose and insulin had
6. The WHI study – unsuitable for the investigation of breast cancer risk 6.1. Characteristics of the women participating in
In the estrogen-only study the women were randomly assigned to be
Concerning the assessment of breast cancer risk, the
treated with either placebo or 0.625 mg conjugated equine estrogens
high age of the women enrolled in the WHI study could
(CEE) in the estrogen/progestin study either with placebo
be regarded as an advantage, because the incidence of
or 0.625 mg conjugated equine estrogens plus 2.5 mg medroxypro-
invasive breast cancer rises with increasing age. The
annual number of breast cancer diagnoses increasesfrom 18/1000 women at age 50 years up to 45/1000
cancer risk. As it was shown that HRT does not influ-
women at age 63 years and to 63/1000 women at age
ence breast cancer risk in postmenopausal women with
70 n both arms of the WHI study the mean age was
about 63 years on average and two third of the women
suitable for the investigation of the influence of HRT
on breast cancer risk. This was even confirmed by the
On the other hand, the extremely high mean body
WHI Observational Study with about 86,000 women
mass index (30.1 and 28.5 kg/m2) and the high per-
centage of overweight (34.8 and 35.3%) and adiposewomen (44.6 and 34.1%) in the CEE arm and the
6.2. The WHI study: effect of CEE/MPA or
CEE/MPA arm of the WHI study suggests a high preva-
lence of the metabolic syndrome (incidence of the metabolic syndrome increases with
The randomised placebo-controlled WHI study was
menopause, and is associated not only with an ele-
planned for an average time of 8.5 years of exposure
vated risk of cardiovascular disease, but also with an in-
to either CEE/MPA or placebo The premature
creased risk of breast cancer owing to insulin resistance
discontinuation of treatment with CEE/MPA after 5.2
years was justified with an increased risk of cardiovas-
women participating in the WHI study had both an el-
cular disease and a pretendedly elevated risk of breast
evated risk of coronary heart disease, and a high breast
cancer estimated hazard ratio (HR) for inva-
H. Kuhl / Maturitas 51 (2005) 83–97
Fig. 1. Number of breast cancer diagnoses per 1000 women per year during the course of treatment with placebo or CEE/MPA in the WHI study(data from of the WHI study published by Chlebowski et al. The left part of the graph refers to women who werenot treated with hormones prior to the WHI study, the right part of the graph refers to women who have received hormone replacement therapyprior to the WHI study (reproduced from Kuhl 2004
sive breast cancer was calculated as 1.26 which was,
1.7 for women with <5 years of prior use and of 2.27
however, not significant. A subsequent updated sub-
for ≥5 years of prior use of HRT was due to the ex-
analysis based on a mean follow-up of 5.6 years re-
tremely low risk in the 2079 women on placebo which
vealed a significantly elevated HR of breast cancer of
did not show an age-dependent increase in risk. This
1.24 which just surpassed the border of statistical sig-
can be interpreted as a hangover effect of pretreatment.
In the Nurses’ Health Study, the HRT-induced eleva-
The analysis revealed, however, that in those women
tion in breast cancer risk decreased within 2 years after
who had never used hormones before initiation of the
cessation of treatment and remained lowered during
WHI study, treatment with CEE/MPA did not increase
the first 5 years without hormones The lacking
the risk of breast cancer. It was elevated during treat-
effect of CEE/MPA on breast cancer risk in the WHI
ment with CEE/MPA only in those patients who re-
study corresponds to the results of other studies which
ported HRT prior to WHI study graph showing
showed that HRT does not increase breast cancer risk
the annual number of breast cancers per 1000 women
in overweight postmenopausal women with a BMI of
during the course of the study (was based
25 kg/m2 or more. This has been observed in the col-
on the data depicted in the paper of Chlebowski et
laborative study in 1997 n cohort studies
al. suspicion that the elevated risk calcu-
but also in the large WHI Observational Study
lated in this group is an artifact due to a pretreatment-associated selection bias In the group of women
6.3. The WHI study: effect of CEE only or placebo
without prior HRT, both the 6277 women treated withCEE/MPA and the 6020 women on placebo showed a
The findings of a consistent reduction in the HR of
similar age-dependent rise in the rate of breast cancer
breast cancer during 6.8 years of treatment of hysterec-
which corresponded to a hazard ratio (HR) of 1.09.
tomized postmenopausal women with CEE alone was
In the group of women with prior HRT before the
highly surprising n total, the relative risk was 0.77
WHI study, treatment of 2225 women with CEE/MPA
(95% CI 0.59–1.01), narrowly missing statistical sig-
also caused an age-dependent increase which – after
nificance. According to the available data on the effect
smoothing for fluctuations – was similar to that of the
6020 never users. In this group, the calculated HR of
been acceptable if the WHI study had revealed no influ-
H. Kuhl / Maturitas 51 (2005) 83–97
ence of estrogens on breast cancer risk. The mean BMI
associated with fat mass and high caloric nutrition, and
of the women participating in the estrogen-only arm
is known as a risk factor for breast cancer. Abdominal
was even higher than in the CEE/MPA arm, and was
obesity in childhood which is related to early menar-
in the range of obesity (30.1 kg/m2). Only 21% had a
che, tends to continue into adult life and may be asso-
BMI < 25 kg/m2, while 34% had a BMI of 25–29 kg/m2
ciated with an earlier onset of insulin resistance
Moreover, late pregnancies are associated with the de-
The reduction in breast cancer risk is difficult to
velopment of insulin resistance which may persist post
explain. Although in postmenopausal women increas-
partum in overweight women n the other hand,
ing BMI correlates with increasing serum levels of
obesity in teenage women may lead to anovulatory cy-
estradiol and breast cancer risk correlates with
cles which are associated with a reduced risk of breast
serum estradiol within a very low concentration range
cancer n contrast, the manifestation of obesity af-
it is not very probable that the rise of estro-
ter teenage increases the risk of postmenopausal breast
gen levels during use of 0.625 mg CEE directly protects
from the development of breast cancer. On the contrary,
In a case-control study with Mexican women char-
it is generally believed that high estrogen serum con-
acterized by a low fat intake, carbohydrate consump-
centrations or high local tissue concentrations stimulate
tion was associated with increased breast cancer risk
growth of breast tumors. So far, the available epidemi-
In another study, a direct association with breast
ological data did not show any difference between the
cancer risk was observed for glycemic index and
effect on breast cancer risk of low and high estrogen
glycemic load, but more in postmenopausal than in pre-
menopausal women High levels of insulin were
Another explanation might be derived from the as-
also found to be associated with poorer survival for
sociation between breast cancer risk, obesity, insulin
postmenopausal women, while higher dietary protein
resistance and hyperinsulinemia, as outlined above
intake was associated with better survival
(According to the high proportion of over-
The question is, whether or not a change in di-
weight and obese women in the WHI study in whom
etary habits leading to weight loss and maintenance
a high prevalence of the metabolic syndrome and in-
of normal body weight, can normalize the elevated
sulin resistance can be assumed, long-term treatment
breast cancer risk in overweight women. The results
with 0.625 mg CEE might have improved insulin re-
of various animal experiments suggest that an energy-
sistance and reduced the elevated insulin levels. This
restricted state induced by reduced caloric intake and/or
might have attenuated the stimulatory effect of insulin
an increased energy expenditure might be a suitable
on tumor growth resulting in a reduction of breast can-
measure to prevent breast cancer In contrast to
endocrine treatments this strategy would also includereceptor-negative carcinoma. It might reduce both thecarcinogen-induced initiation and the growth of exist-
7. How to reduce breast cancer risk?
ing tumors. Interestingly, caloric restriction was ac-companied by a persistent reduction in insulin levels
case-control study revealed that in adult obesewomen weight loss at younger ages may reduce the risk
Western lifestyle is associated with overweight, ab-
of postmenopausal breast cancer, whereas weight loss
dominal obesity, insulin resistance and low physical
after age 45 was ineffective. Fluctuating weight, i.e.,
activity. Higher age, estrogen deficiency and obesity
weight loss followed by weight gain did not influence
increase the prevalence of insulin resistance, and di-
etary habits may play a critical role. Even in non-obese
There are various studies on the association between
postmenopausal women the prevalence of fasting hy-
diet composition and recurrence rate and survival fol-
perinsulinemia is high risk of breast cancer in
lowing breast cancer diagnosis. Most studies did not ad-
Western countries is five-fold that in Japan, but migra-
just for energy intake and the results are contradictory,
tion of Japanese women to the USA results in adapta-
but suggest an increase in mortality with energy intake
tion of risk Early menarche is to a certain degree
and a protective effect of elevated intake of protein,
H. Kuhl / Maturitas 51 (2005) 83–97
beta-carotene, Vitamin C, fruit and vegetables
breast cancer in postmenopausal women. The pro-
For postmenopausal women, there is no epidemiolog-
tection correlated with the duration and intensity
ical evidence for a prophylactic effect of intake of soy
of physical activity and was most pronounced in
or phytoestrogens concerning the risk of breast can-
women with a lower BMI (<24.1 kg/m2) In
cer. Two large NIH-funded clinical trials are currently
another study with postmenopausal women it was
investigating the influence of diet composition on re-
shown that vigorous exercise was associated with
currence and survival in breast cancer patients.
the lowest plasma insulin levels and the highest in-sulin sensitivity, and this effect was enhanced by HRT
7.2. Medical treatment of hyperinsulinemia
There are, however, no clear data on the type and in-
Even though diet and exercise are recommended as
tensity of exercise necessary for a significant beneficial
the primary intervention to improve insulin resistance,
the use of insulin-sensitizing agents in patients with in-sulin resistance might be an option to reduce the inci-
dence of postmenopausal breast cancer. Metformin hasbeen demonstrated to decrease gluconeogenesis and in-
The risk of breast cancer is elevated in women with
testinal absorption of glucose, to increase peripheral
a mother or sister with breast cancer, and increases
glucose uptake and utilization, and to improve insulin
further if there are more affected relatives, particularly
sensitivity and hyperinsulinemia n combination
at young age. In women with genetic mutations
with diet it has been shown to improve the symptoms
associated with a very high risk for breast cancer,
of the metabolic syndrome in women with polycystic
prophylactic bilateral mastectomy may reduce the risk
ovarian syndrome. Metformin has been used in type
by 90% Chemoprevention is also an option to
2 diabetes for many years and is recommended par-
reduce the probability of developing the disease early
ticularly for overweight patients with type 2 diabetes.
in life. Before long-term treatment with tamoxifen
Long-term treatment with insulin-sensitizer may be as-
or raloxifene, GnRH analogs or aromatase inhibitors
sociated with gastrointestinal side-effects and Vitamin
will be considered, the risks, side-effects and benefits
B12 deficiency t remains, however, to be proven
must be carefully evaluated. It is not clarified whether
that long-term metformin-induced normalization of in-
and to what extent the use of HRT in carriers of
sulin levels leads to a reduction in breast cancer risk.
BRCA1 or BRCA2 increases the risk of breastcancer.
Moderate alcohol consumption is associated with a
slightly elevated risk which increases with the amount
Benign breast disease, especially fibrocystic dis-
of consumed alcohol Therefore, abstinence
ease, epithelial hyperplasia and the presence of atypia
or reduction of alcohol consumption may have a
enhance the risk of breast cancer two- to four-fold
favourable effect. A slight increase in breast cancer
It was highest in young women with breast cysts and
risk was found in postmenopausal women who started
decreased with age In postmenopausal women
smoking before 16 years of age. Current smoking has
benign breast disease was associated with a relative
a favourable rather than an unfavourable effect on the
risk of breast cancer of about 1.6 and the use
risk of breast cancer, because the proportion of infer-
of HRT may increase the occurrence of atypical hy-
tile women is higher among smokers and smokers reach
perplasia In premenopausal women with benign
breast disease long-term treatment with daily 8–10 mgnorethisterone, but not progesterone derivatives, was
found to reduce the risk of breast cancer by 50% Whether or not this was associated with a reduction of
The WHI study revealed that an increased phys-
blood flow in the breast remains an open ques-
ical activity is associated with a reduced risk for
H. Kuhl / Maturitas 51 (2005) 83–97
might be reconsidered. Moreover, the general rec-ommendations to individualize HRT may include the
Women with an elevated mammographic density
need of an indication for the use of a progestin.
have a four to six times higher risk of developing breast
There is little doubt that treatment with unopposed
cancer. Mammographic density in more than 75% of
estrogens increases dose-dependently the risk of en-
the breast area was found to be associated with a relative
dometrial hyperplasia and cancer. It has been suggested
risk of about 14 for hyperplasia and of 9 for atypical
that the use of low-dose estrogens might be associated
hyperplasia and/or carcinoma in situ Histologi-
with a lower relative risk of endometrial cancer, but
cal investigation of biopsies revealed that the increase
the results of clinical trials are inconsistent. Whereas
in mammographic density does not reflect changes in
no difference in the risk of endometrial cancer was
ductal or lobular epithelium, but a significantly higher
found between the use of 0.3 and 0.625 mg of unop-
expression of proteoglycans in the stroma which is
posed CEE, the incidence of endometrial hyperplasia
the major breast tissue compartment by volume
did not differ between placebo and 0.3 mg unopposed
These proteoglycans are a highly abundant component
of breast tissue stroma and may be involved in the
It is generally accepted that an endometrial
development of benign (e.g. fibrocystic changes) and
thickness of 5 mm is an appropriate cut-off level in
screening for endometrial hyperplasia. Monitoring
aggregate to form collagen fibres, but can also form
of endometrial growth during estrogen therapy by
macromolecules with a high capacity for water stor-
means of vaginalsonography has been suggested as
age. Therefore, the increase in mammographic density
a suitable diagnostic tool to evaluate the need for the
observed in postmenopausal women during treatment
addition of progestins in patients treated with low-dose
with estrogen/progestin preparations may reflect an in-
estrogens-only. The choice of patients suitable for
creased water storage in breast stroma which may also
this therapy may be facilitated by the outcome of a
cause breast tenderness. A similar phenomenon can be
observed in younger women with premenstrual syn-
In postmenopausal women, there are large varia-
drome who show an increased capillary permeability
tions in the endometrial response to unopposed estro-
gen therapy. Treatment with 0.625 mg CEE, 1–2 mg
It is unknown whether or not this reversible phe-
estradiol or 50 g transdermal estradiol revealed that
nomenon induced by HRT is associated with an ele-
about 20% of the women were fast growers with an
vated risk for breast cancer. As an increased density
increase in endometrial thickness by more than 1 mm
may impair the sensitivity and accuracy of mammo-
in 5 weeks, whereas 50% were slow growers with an
graphic screening, transitory discontinuation of HRT
increase by 1 mm or less over a period of more than 20
for 3 weeks may reverse mammographic density in-
weeks Only a few women developed hyperpla-
crease and improve the diagnostic sensitivity -
sia within 2 months, and no hyperplasia was observed
ing this time, the administration of low-dose estrogens
in women with endometrial thickness of 4 mm or less
may prevent the recurrence of climacteric symptoms.
In 11% of the patients, there was no or onlya slow proliferation rate and after 2 years of treatment
7.8. Do we need an indication for the use of
endometrial thickness was below 8 mm showing nor-
mal biopsies n about two third of the patients theadministration of progestin could be postponed until at
The only indication for the addition of progestins
least to the fourth month without inducing endometrial
to estrogen replacement therapy is the endometrial
protection. Besides other specific progestin-related
Long-cycle HRT using quarterly progestin may,
adverse effects, the progestin component increases
therefore, be an option for the majority of post-
menopausal women, but the most suitable regimens
Considering the emotional and clinical impact of
remain to be elucidated. There are several clinical tri-
breast cancer as compared with that of endometrial
als on the risk of endometrial hyperplasia and cancer in
cancer, the demand for a regular addition of progestins
postmenopausal women during long-cycle HRT which
H. Kuhl / Maturitas 51 (2005) 83–97
revealed contradictory results. Whereas some long-
estrogen-only arm of the WHI study. The lacking effect
cycle regimens taken for 1–5 years did not increase the
in the estrogen/progestin combination arm may be due
incidence of endometrial hyperplasia as compared with
to the impairment by the progestin component of the
the use of normal sequential preparations n
beneficial effect of estrogens on insulin resistance.
elevated rate of endometrial hyperplasia and cancer was
With regard to the breast cancer risk, the develop-
observed in two Scandinavian studies n one
ment of overweight and obesity should be avoided,
of the latter studies, the progestin phase of 10 days
and an appropriate diet and lifestyle should be recom-
might have been too short and in the other study, many
mended early in life. In postmenopausal women with
of the women who developed endometrial cancer, have
insulin resistance, treatment with insulin-sensitizing
been treated with hormones including unopposed es-
agents like metformin might be an option, but a
favourable effect on breast cancer risk remains to
Long-cycle HRT might be applicable to patients
be proven. In healthy postmenopausal women with
who respond to estrogens with slow endometrial pro-
climacteric symptoms, low-dose estrogen therapy is
liferation and have weak or no withdrawal bleeding
the treatment of choice, and the exposure to pro-
during sequential HRT. The most suitable progestins
gestins should be kept minimal in non-hysterectomized
are compounds with strong endometrial activity, and
women. There are large inter-individual variations
in the proliferative response to estrogens of the en-dometrium. Vaginalsonographic surveillance and theintensity of withdrawal bleeding may help to identify
8. Conclusion
those women who may profit from long-cycle regimensof HRT or may be candidates for therapy with low-dose
HRT may stimulate growth of occult breast tumors
in postmenopausal women. This concerns primarilyhormone receptor-positive cancers, and the effect ofestrogens is enhanced by progestins. Observational
References
and randomised studies suggest that HRT with estro-gen/progestin combinations increases the relative risk
[1] Kvale G. Reproductive factors in breast cancer epidemiology.
of breast cancer in postmenopausal women more than
estrogens alone. Besides many other risk factors, over-
[2] Collaborative Group on Hormonal Factors in Breast Cancer.
weight and obesity is associated with an elevated risk
Breast cancer and breastfeeding: collaborative reanalysis ofindividual data from 47 epidemiological studies in 30 coun-
of breast cancer in postmenopausal women, which is
tries, including 50302 women with breast cancer and 96973
women without the disease. Lancet 2002;360:187–95.
As most participants in the WHI study were over-
[3] Garland M, Hunter DJ, Colditz GA, et al. Menstrual cycle
weight, it was not suitable for the investigation of breast
characteristics and history of ovulatory infertility in relation
cancer risk. The increase in risk during treatment with
to breast cancer risk in a large cohort of US women. Am JEpidemiol 1998;147:636–43.
estrogen/progestin concerned only those women who
[4] Collaborative Group on Hormonal Factors in Breast Cancer.
had been pretreated with hormones prior to the WHI
Breast cancer and hormone replacement therapy: collaborative
study, suggesting a selection bias. Moreover, treatment
reanalysis of data from 51 epidemiological studies with 52705
of postmenopausal women with estrogens alone dur-
women with breast cancer and 108411 women without breast
ing 6.8 years caused a consistent decrease in the in-
[5] Hulka BS, Moorman PG. Breast cancer: hormones and other
cidence of breast cancer. Overweight women have a
risk factors. Maturitas 2002;42(Suppl 1):95–108.
high risk for the development of insulin resistance,
[6] Morimoto LM, White E, Chen Z, et al. Obesity, body size, and
and the growth-stimulating effect of elevated insulin
risk of postmenopausal breast cancer: the Women’s Health Ini-
levels may explain the elevated breast cancer risk in
tiative (United States). Cancer Causes Contr 2002;13:741–51.
the postmenopause. As low-dose estrogens may im-
[7] Adami HO, Adams G, Boyle P, et al. Breast cancer etiology.
Int J Cancer 1990;(Suppl 5):22–39.
prove insulin resistance and hyperinsulinemia, the el-
[8] Ewertz M, Duffy SW, Adami HO, et al. Age at first birth,
evated breast cancer risk in obese women may be re-
parity and risk of breast cancer: a meta-analysis of 8 studies
duced. This could explain the favourable results of the
from the Nordic countries. Int J Cancer 1990;46:597–603. H. Kuhl / Maturitas 51 (2005) 83–97
[9] Colditz GA, Rosner B. Cumulative risk of breast cancer to age
[26] Schairer C, Lubin J, Rroisi R, Sturgeon S, Brinton L, Hoover
70 according to risk factor status: data from the nurses’ health
R. Menopausal estrogen and estrogen-progestin replacement
study. Am J Epidemiol 2000;152:950–64.
therapy and breast cancer risk. JAMA 2000;283:485–91.
[10] Collaborative Group on Hormonal Factors in Breast Cancer.
[27] Kirsh V, Kreiger N. Estrogen and estrogen–progestin replace-
Breast cancer and hormonal contraceptives: collaborative re-
ment therapy and risk of postmenopausal breast cancer in
analysis of individual data on 53297 women with breast cancer
Canada. Cancer Causes Contr 2002;13:583–90.
and 100239 women without breast cancer from 54 epidemio-
[28] Porch JV, Lee IM, Cook NR. Estrogen–progestin replacement
logical studies. Lancet 1996;347:1713–27.
therapy and breast cancer risk: the Women’s Health Study
[11] Marchbanks PA, McDonald JA, Wilson HG, et al. Oral con-
(United states). Cancer Causes Contr 2002;13:847–54.
traceptives and the risk of breast cancer. N Engl J Med
[29] Daling JR, Malone KE, Doody DR. Relation of regimens
of combined hormone replacement therapy to lobular, duc-
[12] Writing Group for the Women’s Health initiative Investi-
tal, and other histologic types of breast carcinoma. Cancer
gators. Risks and benefits of estrogen plus progestin in
healthy postmenopausal women: principal results from the
[30] Weiss LK, Burkman RT, Cushing-Haugen KL. Hormone re-
Women’s Health Initiative randomised controlled trial. JAMA
placement therapy regimens and breast cancer risk. Obstet
[13] Chen WY, Colditz GA, Rosner B, et al. Use of postmenopausal
[31] Chen CL, Weiss NS, Newcomb P. Hormone replacement ther-
hormones, alcohol, and risk for invasive breast cancer. Ann
apy in relation to breast cancer. JAMA 2002;287:734–41.
[32] Jernstr¨om H, Bendahl PO, Lidfeldt J, Nerbrand C, Agardh
[14] Kaye JA, Meier CR, Walker AM, Jick H. Statin use, hy-
CD, Samsioe G. A prospective study of different types of
perlipidaemia, and the risk of breast cancer. Br J Cancer
hormone replacement therapy use and the risk of subsequent
breast cancer: the women’s health in the Lund area (WHILA)
[15] McTiernan, Kooperberg C, White E, et al. Recreational phys-
study (Sweden). Cancer Causes Contr 2003;14:673–80.
ical activity and the risk of breast cancer in postmenopausal
[33] Li CI, Malone KE, Porter PL. Relationship between long du-
women (WHI cohort study). JAMA 2003;290:1331–6.
rations and different regimens of hormone therapy and risk of
[16] Schernhammer ES, Laden F, Speizer FE, et al. Rotating night
breast cancer. JAMA 2003;289:3254–63.
shifts and risk of breast cancer in women participating in the
[34] Bakken K, Asaker E, Eggen AE, Lund E. Hormone replace-
nurses’ health study. J Natl Cancer Inst 2001;93:1563–8.
ment therapy and incidence of hormone-dependent cancers
[17] Velicer CM, Heckbert SR, Lampe JW, Potter JD, Robertson
in the Norwegian Women and Cancer Study. Int J Cancer
CA, Taplin SH. Antibiotic use in relation to the risk of breast
[35] Stahlberg C, Pedersen AT, Lynge E, et al. Increased risk of
[18] Hulley S, Furberg C, Barrett-Connor E, et al. Noncardiovas-
breast cancer following different regimens of hormone re-
cular disease outcomes during 6.8 years of hormone ther-
placement therapy frequently used in Europe. Int J Cancer
apy. Heart and estrogen/progestin replacement study follow-
up (HERS II). JAMA 2002;288:58–66.
[36] Stahlberg C, Pedersen AT, Andersen ZJ, et al. Breast cancer
[19] The Women’s Health Initiative Steering Committee. Effects
with different prognostic characteristics developing in Dan-
of conjugated equine estrogen in postmenopausal women with
ish women using hormone replacement therapy. Br J Cancer
hysterectomy. The Women’s Health Initiative Randomized
Controlled Trial. JAMA 2004;291:1701–12.
[37] Tjonneland A, Christensen J, Thomsen BL, et al. Hormone
[20] Kuhl H. Effects of estrogen-only treatment in postmenopausal
replacement therapy in relation to breast carcinoma incidence
rate ratios. Cancer 2004;100:2328–37.
[21] Million Women Study Collaborators. Breast cancer and
[38] Colditz GA, Rosner BA, Chen WY, Holmes MD, Hank-
hormone-replacement therapy in the Million Women Study.
inson SE. Risk factors for breast cancer according to es-
trogen and progesterone receptor status. J Natl Cancer Inst
[22] Magnusson C, Baron JA, Correia N. Breast cancer risk
following long-term oestrogen- and oestrogen-progestin-
[39] Black WC, Welch HG. Advances in diagnostic imaging and
replacement therapy. Int J Cancer 1999;81:339–44.
overestimations of disease prevalence and the benefits of ther-
[23] Chlebowski RT, Hendrix, Langer RD, et al. Influence of es-
apy. N Engl J Med 1993;328:1237–43.
trogen plus progestin on breast cancer and mammography in
[40] Menard S, Casalini P, Agresti R, Pilotti S, Balsari A. Prolif-
healthy postmenopausal women. JAMA 2003;289:3243–53.
eration of breast carcinoma during menstrual phases. Lancet
[24] Bush TL, Whiteman M, Flaws JA. Hormone replacement ther-
apy and breast cancer: a qualitative review. Obstet Gynecol
[41] Potten CS, Watson RJ, Williams GT, et al. The effect of age
and menstrual cycle upon proliferative activity of the normal
[25] Ross RK, Paganini-Hill A, Wan PC, Pike MC. Effect of
human breast. Br J Cancer 1988;58:163–70.
hormone replacement therapy on breast cancer risk: es-
[42] Hofseth LJ, Raafat AM, Osuch JR, Pathak DR, Slom-
trogen versus estrogen plus progestin. J Natl Cancer Inst
ski CA, Haslam SZ. Hormone replacement therapy with
estrogen or estrogen plus medroxyprogesterone acetate is
H. Kuhl / Maturitas 51 (2005) 83–97
associated with increased epithelial proliferation in the
[60] Lindheim SR, Presser SC, Ditkoff EC, Vijod MA, Stanczyk
normal postmenopausal breast. J Clin Endocrinol Metab
FZ, Lobo RA. A possible bimodal effect of estrogen on insulin
sensitivity in postmenopausal women and the attenuating ef-
[43] Cline JM, Soderqvist G, von Schoultz E, Skoog L, von
fect of added progestin. Fertil Steril 1993;60:664–7.
Schoultz B. Effects of hormone replacement therapy on
[61] Carr MC. The emergence of the metabolic syndrome with
mammary gland of surgically postmenopausal cynomolgus
menopause. J Clin Endocrinol Metab 2003;88:2404–11.
macaques. Am J Obstet Gynecol 1996;174:93–100.
[62] Stefan N, Vozarova B, Funahashi T, et al. Plasma adiponectin
[44] Cline JM, Register TC, Clarkson TB. Effects of tibolone and
concentration is associated with skeletal muscle insulin re-
hormone replacement therapy on the breast of cynomolgus
ceptor tyrosine phosphorylation, and low plasma concentra-
tion precedes a decrease in whole-body insulin sensitivity in
[45] Suparto ICH, Williams JK, Cline JM, Anthony MS, Fox
JL. Contrasting effects of two hormone replacement thera-
[63] Weyer C, Funahashi T, Tanaka S, et al. Hypoadiponectine-
pies on the cardiovascular and mammary gland outcomes in
mia in obesity and type 2 diabetes: close association with
surgically postmenopausal monkeys. Am J Obstet Gynecol
insulin resistance and hyperinsulinemia. J Clin Endocrinol
[46] Clarke RB. Human breast cell proliferation and its relationship
[64] Mantzoros C, Petridou E, Dessypris N, et al. Adiponectin
to steroid receptor expression. Climacteric 2004;7:129–37.
and breast cancer risk. J Clin Endocrinol Metab 2004;89:
[47] Conneely OM, Jericevic BM, Lydon JP. Progesterone recep-
tors in mammary gland development and tumorigenesis. J
[65] Schairer C, Hill D, Sturgeon SR, et al. Serum concentrations
Mammary Gland Biol Neoplasia 2003;8:205–14.
of IGF-1, IGFBP-3 and C-peptide and risk of hyperplasia and
[48] Roger P, Sahla ME, M¨akel¨a S, Gustafsson JA, Baldet P,
cancer of the breast in postmenopausal women. Int J Cancer
Rochefort H. Decreased expression of estrogen receptor 
protein in proliferative preinvasive mammary tumors. Cancer
[66] Michels KB, Solomon CG, Hu FB, et al. Type 2 diabetes and
subsequent incidence of breast cancer in the Nurses’ Health
[49] Fuqua SA, Schiff R, Parra I, et al. Estrogen receptor  pro-
Study. Diabetes Care 2003;26:1752–8.
tein in human breast cancer: correlation with clinical tumor
[67] Brown MD, Korytkowski MT, Zmuda JM, McCole SD,
parameters. Cancer Res 2003:2434–9.
Moore GE, Hagberg JM. Insulin sensitivity in postmenopausal
women. Diabetes Care 2000;23:1731–6.
stem/progenitor cells and the estrogen receptor. Trends En-
[68] Espeland MA, Hogan PE, Fineberg SE, et al. Effect of post-
menopausal hormone therapy on glucose and insulin concen-
[51] Bray GA. Medical consequences of obesity. J Clin Endocrinol
trations. Diabetes Care 1998;21:1589–95.
[69] Sumino H, Ichikawa S, Itoh H, et al. Hormone replacement
[52] Pan SY, Johnson KC, Ugnat AM, et al. Association of obesity
therapy decreases insulin resistance and lipid metabolism in
and cancer risk in Canada. Am J Epidemiol 2004;159:259–68.
Japanese postmenopausal women with impaired and normal
[53] Schapira DV, Clark RA, Wolff PA, Jarrett AR, Kumar NB,
glucose tolerance. Horm Res 2003;60:134–42.
Aziz NM. Visceral obesity and breast cancer risk. Cancer
[70] Gelfand MM, Fugere P, Bissonnette F, et al. Conjugated es-
trogens combined with sequential dydrogesterone or medrox-
[54] Lahmann PH, Lissner L, Gullberg B, Olsson H, Berglund G.
yprogesterone acetate in postmenopausal women: effects on
A prospective study of adiposity and postmenopausal breast
lipoproteins, glucose tolerance, endometrial histology, and
cancer risk: the Malm¨o diet and cancer study. Int J Cancer
[71] Margolis KL, Bonds DE, Rodabough RJ, et al. Effect of oe-
[55] Lahmann PH, Hoffmann K, Allen N, et al. Body size and
strogen plus progestin on the incidence of diabetes in post-
breast cancer risk: findings from the European Prospective
menopausal women: results from the Women’s Health Initia-
Investigation into Cancer and Nutrition (EPIC). Int J Cancer
tive Hormone Trial. Diabetologia 2004;47:1175–87.
[72] Kuhl H. Is the elevated breast cancer risk observed in the
[56] Toniolo PG, Levitz M, Zeleniuch-Jacquotte A, et al. A
WHI study an artifact? (letter to the editor). Climacteric
prospective study of endogenous estrogens and breast cancer
in postmenopausal women. J Natl Cancer Inst 1995;87:190–7.
[73] Colditz GA, Hankinson SE, Hunter DJ, et al. The use of es-
[57] Thomas HV, Key TJ, Allen DS, et al. A prospective study of
trogens and progestins and the risk of breast cancer in post-
endogenous serum hormone concentrations and breast cancer
menopausal women. N Engl J Med 1995;332:1589–93.
risk in postmenopausal women on the island of Guernsey. Br
[74] Endogenous Hormones and Breast Cancer Collaborative
Group. Body mass index, serum sex hormones, and breast
[58] Cauley JA, Lucas FL, Kuller LH, et al. Elevated serum estra-
cancer risk in postmenopausal women. J Natl Cancer Inst
diol and testosterone concentrations are associated with a high
risk for breast cancer. Ann Intern Med 1999;130:270–7.
[75] Huang Z, Hankinson SE, Colditz GA, et al. Dual effects
[59] Stoll BA. Upper abdominal obesity, insulin resistance and
of weight and weight gain on breast cancer risk. JAMA
breast cancer risk. Int J Obesity 2002;26:747–53. H. Kuhl / Maturitas 51 (2005) 83–97
[76] Romieu I, Lazcano-Ponce E, Sanchez-Zamorano LM, Willett
vessels in women with premenstrual tension. Am J Obstet
W, Hernandez-Avila M. Carbohydrates and the risk of breast
cancer among Mexican women. Cancer Epidemiol Biomark
[92] Colacurci N, Fornaro F, de Franciscis P, Mele D, Palermo M,
del Vecchio W. Effects of a short-term suspension of hormone
[77] Augustin LSA, Dal Maso L, La Vecchia C, et al. Dietary
replacement therapy on mammographic density. Fertil Steril
glycemic index and glycemic load, and breast cancer risk:
a case-control study. Ann Oncol 2001;12:1533–8.
[93] Trabal JF, Lenihan JP, Melchione TE, et al. Low-dose
[78] Borugian MJ, Sheps SB, Kim-Sing C, et al. Insulin,
unopposed estrogens: preliminary findings on the fre-
macronutrient intake, and physical activity: are potential
quency and duration of vaginal bleeding in postmenopausal
indicators of insulin resistance associated with mortality
women receiving esterified estrogens over a two-year period.
from breast cancer? Cancer Epidemiol Biomark Prevdkjdot
[94] Notelovitz M, Varner RE, Reaber RW, et al. Minimal endome-
[79] Thrompson HJ, Zhu Z, Jiang W. Dietary energy restriction in
trial proliferation over a two-year period in postmenopausal
breast cancer prevention. J Mammary Gland Biol Neoplasia
women taking 0.3 mg of unopposed esterified estrogens.
[80] Trentham-Dietz A, Newcomb PA, Egan KM, et al. Weight
[95] Cushing KL, Weiss NS, Voigt LF, McKnight B, Beresford
change and risk of postmenopausal breast cancer (United
SAA. Risk of endometrial cancer in relation to use of low-
States). Cancer Causes Contr 2000;11:533–42.
dose, unopposed estrogens. Obstet Gynecol 1998;91:35–9.
[81] Rock CL. Diet and breast cancer: can dietary factors influence
[96] Meuwissen JHJM, van Langen H, Moret E, Navarro-
survival? J Mammary Gland Biol Neoplasia 2003;8:119–32.
Morquecho I. Monitoring of oestrogen replacement ther-
[82] Kirpichnikov D, McFarlane SI, Sowers JR. Metformin: an
apy by vaginosonography of the endometrium. Maturitas
update. Ann Intern Med 2002;137:25–33.
[83] Biglia N, Defabiani E, Ponzone R, Mariani L, Marenco
[97] Meuwissen JHJM, Oddens BJ, Klinkhamer PJJM. Endome-
D, Sismondi P. Management of risk of breast carci-
trial thickness assessed by transvaginal ultrasound insuffi-
noma in postmenopausal women. Endocrine-related Cancer
ciently predicts occurrence of hyperplasia during unopposed
oestrogen use. Maturitas 1996;24:21–30.
[84] Adami HO, Adams G, Boyle P, et al. Breast-cancer etiology.
[98] Ettinger B, Selby J, Citron JT, Vangessel A, Ettinger
Int J Cancer 1990;(Suppl 5):22–39.
VM, Hendrickson MR. Cyclic hormone replacement ther-
[85] Dixon JM, McDonald C, Elton RA, Miller WR. Risk of breast
apy using quarterly progestin. Obstet Gynecol 1994;83:693–
cancer in women with palpable breast cysts: a prospective
[99] Hirvonen E, Salmi T, Puolakka J, et al. Can progestin be lim-
[86] Gayet A, Esteve J, Seradour B, Piana L, Jacquemier J. Does
ited to every third month only in postmenopausal women tak-
hormone replacement therapy increase the frequency of breast
ing estrogen? Maturitas 1995;21:39–44.
atypical hyperplasia in postmenopausal women? Results from
[100] Boerrigter PJ, van de Weijer PHM, Baak JPA, Fox H, Haspels
the Bouches du Rhone district screening campaign. Eur J Can-
AA, Kenemans P. Endometrial response in estrogen replace-
ment therapy quarterly combined with a progestogen. Matu-
[87] Plu-Bureau G, Le MG, Sitruk-Ware R, Thalabard JC,
Mauvais-Jarvis. Progestogen use and decreased risk of breast
[101] Pinto AB, Binder EF, Kohrt WM, Bronder DR, Williams
cancer in a cohort study of premenopausal women with benign
DB. Effects of trimonthly progestin administration on the en-
breast disease. Br J Cancer 1994;70:270–7.
dometrium in elderly postmenopausal women who receive
[88] Madjar H, Vetter M, Pr¨ompeler H, Breckwoldt M, Pfleiderer
hormone replacement therapy: a pilot study. Am J Obstet Gy-
A. Doppler measurement of breast vascularity in women under
pharmacologic treatment of benign breast disease. J Reprod
[102] Erkkola R, Kumento U, Lehmuskoski S, Mattila L, Mustonen
M. No increased risk of endometrial hyperplasia with fixed
[89] Boyd NF, Jensen HM, Cooke G, Lee Han H, Lockwood GA.
long-cycle oestrogen–progestogen therapy after five years. J
Mammographic densities and the prevalence and incidence
of histological types of benign disease. Eur J Cancer Prev
[103] Bjarnason K, Cerin A, Lindgren R, Weber T. Adverse endome-
trial effects during long cycle hormone replacement therapy.
[90] Alowami S, Troup S, Al-Haddad S, Kirkpatrick I, Watson
PH. Mammographic density is related to stroma and stromal
[104] Pukkala E, Tulenheimo-Silfvast A, Leminen A. Incidence
proteoglycan expression. Breast Cancer Res 2003;5:R129–35.
of cancer among women using long versus monthly cycle
[91] Wong WH, Freedman RI, Levan NE, Hyman C, Quilligan
hormonal replacement therapy, Finland 1994–1997. Cancer
EJ. Changes in the capillary filtration coefficient of cutaneous
PRODUCT SPECIFICATION Model: LR1865EC 1.3Ah Signature Date Customer Company Name : Approval Company Stamp : Prepared By Checked By Approved By TEL: (86) -22-83710503 FAX: (86)-22-83711060 http://www.lishen.com.cn History of revision Product Specification Tianjin Lishen Battery Joint-Stock Co., Ltd. TITLE: Cylindrical Lithi
Vaginal Thrush Many women have an occasional bout of vaginal thrush. It is due to an infection with a yeast germ called Candida. Treatment options include a tablet that you can take by mouth, or anti-thrush pessaries that you can insert into the vagina. There is also anti-thrush cream that you can rub onto the skin around the vagina (the vulva) if needed. Treatment usually works well. However,
 Breast cancer risk in the WHI study: The problem of obesity
Department of Gynecology and Obstetrics, J. W. Goethe University of Frankfurt, Theodor-Stern-Kai 7,
D-60590 Frankfurt am Main, Germany
Abstract
Breast cancer risk in the WHI study: The problem of obesity
Department of Gynecology and Obstetrics, J. W. Goethe University of Frankfurt, Theodor-Stern-Kai 7,
D-60590 Frankfurt am Main, Germany
Abstract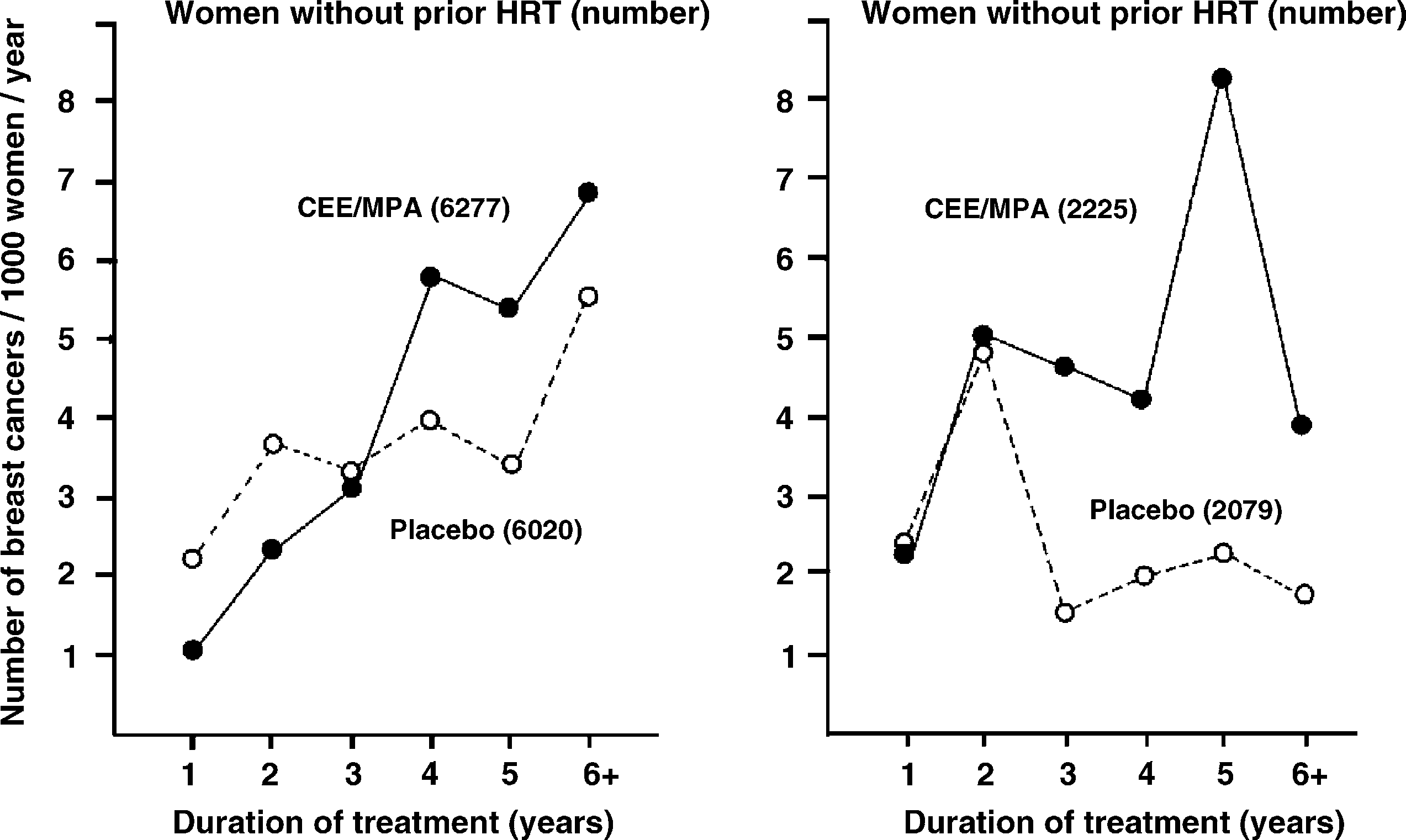 H. Kuhl / Maturitas 51 (2005) 83–97
Fig. 1. Number of breast cancer diagnoses per 1000 women per year during the course of treatment with placebo or CEE/MPA in the WHI study(data from of the WHI study published by Chlebowski et al. The left part of the graph refers to women who werenot treated with hormones prior to the WHI study, the right part of the graph refers to women who have received hormone replacement therapyprior to the WHI study (reproduced from Kuhl 2004
sive breast cancer was calculated as 1.26 which was,
1.7 for women with <5 years of prior use and of 2.27
however, not significant. A subsequent updated sub-
for ≥5 years of prior use of HRT was due to the ex-
analysis based on a mean follow-up of 5.6 years re-
tremely low risk in the 2079 women on placebo which
vealed a significantly elevated HR of breast cancer of
did not show an age-dependent increase in risk. This
1.24 which just surpassed the border of statistical sig-
can be interpreted as a hangover effect of pretreatment.
H. Kuhl / Maturitas 51 (2005) 83–97
Fig. 1. Number of breast cancer diagnoses per 1000 women per year during the course of treatment with placebo or CEE/MPA in the WHI study(data from of the WHI study published by Chlebowski et al. The left part of the graph refers to women who werenot treated with hormones prior to the WHI study, the right part of the graph refers to women who have received hormone replacement therapyprior to the WHI study (reproduced from Kuhl 2004
sive breast cancer was calculated as 1.26 which was,
1.7 for women with <5 years of prior use and of 2.27
however, not significant. A subsequent updated sub-
for ≥5 years of prior use of HRT was due to the ex-
analysis based on a mean follow-up of 5.6 years re-
tremely low risk in the 2079 women on placebo which
vealed a significantly elevated HR of breast cancer of
did not show an age-dependent increase in risk. This
1.24 which just surpassed the border of statistical sig-
can be interpreted as a hangover effect of pretreatment.