Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
Amiraclemolecule.com
Asymmetric Dimethylarginine Plasma Concentrations Differin Patients with End-Stage Renal Disease: Relationship toTreatment Method and Atherosclerotic Disease
AFFER,* MARK BARBEY,‡ KARL M. KOCH,* and
*Department of Nephrology, †Institute of Clinical Pharmacology, and ‡Department of Diagnostic Radiology,Hannover Medical School, Hannover, Germany.Abstract. Asymmetric dimethylarginine (ADMA) is an endog-
than those in the control group (6.0 Ϯ 0.5 versus 1.0 Ϯ 0.1
enous inhibitor of endothelial nitric oxide (NO) synthase. Its
mol/L; P Ͻ 0.05). Plasma nitrate concentrations were signif-
concentration is elevated in patients with end-stage renal dis-
icantly lower in HD-treated patients, which suggests that
ease (ESRD), in part because it is excreted via the kidneys. In
ADMA may inhibit NO synthase. In contrast, plasma ADMA
this study, the plasma concentrations of ADMA, symmetric
levels and nitrate concentrations in PD-treated patients were
dimethylarginine, and L-arginine were determined in relation to
similar to those in control subjects. Plasma L-arginine concen-
plasma nitrate levels (as an index of NO formation) for a group
trations were not significantly decreased in patients with
of 80 patients with ESRD. The effects of two treatment meth-
ESRD. ADMA concentrations were significantly decreased 5 h
ods, i.e., hemodialysis (HD) and peritoneal dialysis (PD), and
after HD, compared with baseline values. ADMA levels were
the role of the presence of atherosclerotic disease were evalu-
significantly higher in HD-treated patients with manifest ath-
ated. Forty-three patients receiving HD and 37 patients receiv-
erosclerotic disease than in HD-treated patients without ath-
ing PD were compared with healthy control subjects. Plasma
erosclerotic disease (7.31 Ϯ 0.70 versus 3.95 Ϯ 0.52 mol/L;
L-arginine and dimethylarginine levels were determined by
P Ͻ 0.05). This study confirms that ADMA is accumulated in
HPLC, using precolumn derivatization with o-phthaldialde-
ESRD. PD-treated patients exhibit significantly lower ADMA
hyde. Plasma nitrate levels were determined by gas chroma-
levels than do HD-treated patients. Accumulation of ADMA
tography-mass spectrometry. Predialysis ADMA concentra-
may be a risk factor for the development of endothelial dys-
tions in HD-treated patients were approximately sixfold higher
function and cardiovascular disease in patients with ESRD.
Endothelium-derived nitric oxide (NO) plays an important role
NO synthase (4). It is synthesized and metabolized by human
in the regulation of BP and platelet aggregation. It is synthe-
endothelial cells (5). ADMA and its biologically inactive ste-
sized by stereospecific oxidation of the terminal guanidino
reoisomer symmetric dimethylarginine (SDMA) are at least in
nitrogen of the amino acid L-arginine (1). NO is produced by
part eliminated via urinary excretion (6). Vallance et al. (7)
the action of a family of NO synthases, with endothelial,
were the first to report elevated plasma levels of ADMA and
neuronal, and macrophage isoforms (2).
SDMA in a small group of patients with end-stage renal
The synthesis of NO can be selectively inhibited by gua-
disease (ESRD). In their study, dimethylarginine (DMA) levels
nidino-substituted analogs of L-arginine, such as N-monometh-
were elevated approximately sixfold, compared with those for
yl-L-arginine, which act as competitive antagonists at the active
healthy control subjects. Those authors suggested that the high
site of the enzyme (3). Asymmetric dimethylarginine (ADMA)
incidence of conditions such as hypertension, atherosclerosis,
has been recently characterized as an endogenous inhibitor of
and immune dysfunction among patients with ESRD might becaused at least in part by dysfunction of the L-arginine/NOpathway secondary to accumulation of ADMA (7).
Data from several experimental studies suggest that ADMA
Received July 7, 1998. Accepted September 17, 1998.
concentrations in a pathophysiologically high range (3 to 15
Portions of this work were presented orally at the 35th Annual Meeting of theEuropean Dialysis and Transplantation Association (June 6 to 9, 1998, Rimini,
mol/L) significantly inhibit vascular NO formation (8,9).
Moreover, it was recently found by our group that plasma
Correspondence to Dr. Rainer H. Bo¨ger, Institute of Clinical Pharmacology,
ADMA levels are also elevated in atherosclerotic patients and
Medical School Hannover, Carl-Neuberg-Strasse 1, 30625 Hannover, Ger-
in hypercholesteremic subjects with normal renal function,
many. Phone: 49 511 532 4631; Fax: 49 511 532 5199; E-mail: boeger.rainer
suggesting that mechanisms other than decreased renal elimi-
nation may contribute to the elevation of plasma ADMA levels
in hypercholesterolemia and atherosclerosis (10). It is therefore
Journal of the American Society of NephrologyCopyright 1999 by the American Society of Nephrology
unclear whether elevated ADMA concentrations in patients
with ESRD are a cause or a consequence of accompanying
PD was 2.13 Ϯ 0.09, well above the recommended weekly Kt/Vurea
The aim of this study was to determine the plasma concen-
The mean serum creatinine concentration was 922 Ϯ 47 mol/L,
and the mean BP was 137.2 Ϯ 2.8/83.8 Ϯ 1.6 mmHg. Average serum
cholesterol and triglyceride levels were 6.16 Ϯ 0.24 and 2.80 Ϯ 0.26
ship to NO formation (measured as plasma nitrate concentra-
mmol/L, respectively. The body mass index averaged 23.2 Ϯ 0.6, and
tions) in patients with ESRD, compared with age-matched
the mean serum albumin concentration was 36.7 Ϯ 0.8 g/L. Heparin-
control subjects with normal renal excretory function. The
ized blood samples from fasting subjects were obtained during routine
effects of two treatment methods, i.e., hemodialysis (HD) and
peritoneal dialysis (PD), on these parameters were also evaluated.
The control group consisted of 37 elderly, healthy, normotensive
subjects with no apparent disease (13 female and 24 male patients;mean age, 68.3 Ϯ 1.1 yr), who exhibited mean serum creatinine
Materials and Methods
concentrations of 79.3 Ϯ 3.5 mol/L. Average cholesterol and tri-
glyceride levels were 4.86 Ϯ 0.11 and 1.61 Ϯ 0.12 mmol/L, respec-
Four groups of individuals were included in this study, after they
tively. The presence of cardiovascular or metabolic disease was ex-
had given informed consent for participation. The first group con-
cluded by medical histories, physical examinations, and routine
sisted of 43 patients receiving HD (20 female and 23 male patients;
mean age, 64.9 Ϯ 1.6 yr) who had been treated with HD for a median
An additional control group consisted of 33 patients with manifest
of 38 mo (range, 1 to 200 mo), with residual diuresis of 582 Ϯ 95 ml
arteriosclerotic disease and normal renal function. These patients (13
of urine/24 h. Sixteen of the 43 (37%) HD-treated patients were
female and 20 male patients; mean age, 61.4 Ϯ 4.0 yr) had peripheral
anuric. The average diuresis among the remaining 27 patients was
arterial occlusive disease, as verified by angiography or duplex-
sonography. The serum creatinine concentration in this group was
For these patients, a venous blood sample was drawn at midweek
96.0 Ϯ 4.4 mol/L; average cholesterol and triglyceride levels were
before dialysis. Patients were treated with HD three times each week
6.24 Ϯ 0.22 and 1.81 Ϯ 0.14 mmol/L, respectively, and BP was
and were in clinically stable conditions. The mean serum creatinine
level was 707 Ϯ 108 mol/L, and the mean arterial BP was 141.0 Ϯ3.4/78 Ϯ 1.7 mmHg. Average serum cholesterol and triglyceridelevels were 5.29 Ϯ 0.17 and 2.09 Ϯ 0.16 mmol/L, respectively. The
body mass index averaged 23.6 Ϯ 0.6, and the mean serum albumin
The plasma concentrations of L-arginine, NG,NG-DMA (ADMA),
level was 37.6 Ϯ 1.1 g/L. Patients underwent standard bicarbonate
and NG,NЈG-DMA (SDMA) were measured by HPLC with precolumn
HD with biocompatible membranes (Hemophan® [Gambro Medizin-
derivatization with o-phthaldialdehyde (OPA), using a modification of
technik, Munich, Germany] and polyamide membranes, sterilized
a previously published method (13). L-Homoarginine (10 mol/L)
with steam). The average dialysis time was 270 Ϯ 6 min, blood flow
was added to 0.5 ml of plasma as an internal standard. Plasma samples
was 290 Ϯ 8 ml/min, and dialysate flow was 500 ml/min. The delivered
and standards were extracted on solid-phase extraction cartridges
dialysis dose measured by urea reduction rate was 67.2 Ϯ 1.1%, well
(CBA Bond Elut; Varian, Harbor City, CA). The recovery rates were
above the suggested dialysis dose (by urea reduction rate) of 65%
82.9 Ϯ 3.8%. Eluates were dried under nitrogen and resuspended in
double-distilled water for HPLC analysis. Samples and standards were
Subgroup analysis was performed for patients with ESRD with
incubated with OPA reagent (5.4 mg/ml OPA in borate buffer, pH 8.4,
atherosclerotic vascular disease (n ϭ 22), which was defined as the
containing 0.4% 2-mercaptoethanol) for exactly 30 s before automatic
presence of clinically and angiographically or duplex-sonographically
injection into the HPLC system. The OPA derivatives of L-arginine,
verified peripheral arterial occlusive disease (Fontaine stage IIb to IV)
ADMA, and SDMA were separated on a 250- ϫ 4.5-mm (inner
alone (n ϭ 2) or in combination with a history of prior myocardial
diameter), 7-m, Nucleosil phenyl column (Macherey and Nagel,
infarction (n ϭ 20), compared with patients with ESRD without
Du¨ren, Germany), with the fluorescence detector set for an excitation
vascular disease (n ϭ 11). For a subgroup of eight HD-treated
wavelength of 340 nm and an emission wavelength of 450 nm.
patients, additional heparinized blood samples for the analysis of
Samples were eluted from the column with 0.96% citric acid/methanol
ADMA, SDMA, L-arginine, and nitrate were drawn 1, 5, and 18 h
(2:1, pH 6.8), at a flow rate of 1 ml/min. Standard curves generated for
after the end of a dialysis session (duration, 4.5 h). These patients (five
ADMA and SDMA in water and in pooled human plasma showed
female and three male patients; mean age, 63.1 Ϯ 4.5 yr) had been
linearity over a concentration range from 0.1 to 16 mol/L. The
receiving HD for a median of 18 mo (range, 1 to 82 mo). The mean
coefficients of variation of this method were 5.2% within assays and
serum creatinine concentration was 760 Ϯ 49 mol/L, and the mean
5.5% between assays; the detection limit was 0.1 mol/L.
arterial BP was 133.8 Ϯ 9.7/81.3 Ϯ 3.7 mmHg. Average serum
The ADMA/creatinine ratio was calculated, as ADMA (micromo-
cholesterol and triglyceride levels were 5.33 Ϯ 0.50 and 2.44 Ϯ 0.42
lar)/creatinine (micromolar) ϫ 10Ϫ3, for patients for whom multiple
samples were drawn before and after HD sessions, to assess the
The second group consisted of 37 patients (16 female and 21 male
different effects of HD treatment on methylarginine levels, as opposed
patients) receiving PD (24 patients undergoing nightly intermittent
to serum creatinine levels. Plasma nitrate was assayed as its pentaflu-
PD, nine continuous ambulatory PD, three continuous cyclic PD, and
orobenzyl derivative by gas chromatography-mass spectrometry, as
one intermittent PD; mean age, 46.4 Ϯ 2.5 yr), who had received PD
described previously (14). The detection limit of the method was 20
for a median of 55 mo (range, 7 to 168 mo). These patients exhibited
fmol of nitrite or nitrate. Intra- and interassay variabilities were
residual diuresis of 658 Ϯ 129 ml of urine/24 h. Thirteen of the 37
Ͻ3.8%. Serum creatinine concentrations were determined spectro-
(35%) patients receiving PD were anuric. The average diuresis among
photometrically with the alkaline picric acid method, in an automatic
the remaining 24 patients was 1015 Ϯ 151 ml/24 h (P ϭ not signif-
analyzer (Beckman, Galway, Ireland). Protein concentrations were
determined spectrophotometrically using the biuret method. All other
Journal of the American Society of Nephrology
laboratory data were obtained from routine laboratory tests, using
Table 1. ADMA, SDMA, L-arginine, L-arginine/ADMA
ratio, and nitrate concentration as determinants ofnitric oxide synthesis in control subjects (control)
Data are presented as mean Ϯ SEM unless otherwise stated. Sta-
tistical significance was tested using ANOVA, followed by the Fisher
protected least significant difference test for comparisons betweenpatient groups. Repeated measurements were tested for statistical
significance using ANOVA and the Scheffe´ F test. Statistical signif-
icance was accepted for P Ͻ0.05. Plasma L-Arginine, ADMA, SDMA, and NitrateConcentrations in ESRD
a Data are mean Ϯ SEM. Results are given as mol/L. ADMA,
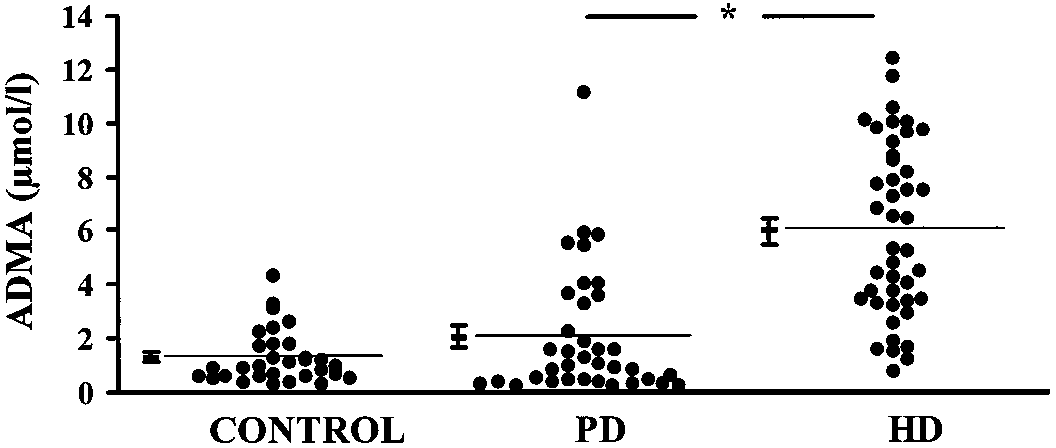
Compared with control subjects, HD-treated patients exhib-
asymmetric dimethylarginine; SDMA, symmetric dimethylarginine;
ited significantly higher plasma ADMA concentrations (P Ͻ
PD, peritoneal dialysis; HD, hemodialysis.
b P Ͻ 0.05 versus control.
0.05) (Figure 1). Plasma SDMA levels were also significantly
c P Ͻ 0.05 versus PD.
higher, but L-arginine concentrations were not significantlydifferent between the two groups (Table 1). Plasma nitrateconcentrations were significantly lower in HD-treated patientsthan in control subjects (Table 1).
change in plasma ADMA and SDMA concentrations was ob-
ADMA levels in PD-treated patients were not different from
served. When the concentrations of these L-arginine analogs
those in control subjects (P Ͼ 0.05) (Figure 1). However,
were expressed with respect to serum creatinine concentra-
SDMA concentrations in the PD-treated group were signifi-
tions, there was a significant elevation 1 h after dialysis,
cantly higher than those in control subjects (P Ͻ 0.05) (Table
compared with predialysis concentrations (ADMA, 0.86 Ϯ
1). L-Arginine and nitrate concentrations and the L-arginine/
0.20 versus 2.02 Ϯ 0.33; P Ͻ 0.05). Five hours after the end of
ADMA ratio were not significantly different, compared with
the HD session, ADMA concentrations were significantly de-
those for the control group (P Ͼ 0.05) (Table 1).
creased, below values measured 1 h after dialysis. ADMA
HD-treated patients exhibited significantly higher mean
levels then continuously increased until 18 h after dialysis
ADMA concentrations, compared with PD-treated patients.
(Figure 2). A similar time course was observed for SDMA
SDMA, L-arginine, and nitrate concentrations did not differ
levels (Table 2). However, it seemed that the reduction in
significantly between these groups. The L-arginine/ADMA ra-
plasma SDMA levels at 5 h after dialysis was not as marked as
tio in the HD-treated patients was significantly lower than that
that for ADMA. Plasma L-arginine concentrations remained
in the PD-treated patients (Table 1).
unchanged after HD. Plasma nitrate levels and total proteinconcentrations did not change significantly. Effects of HD on the Time Course of PlasmaL-Arginine, DMA, and Nitrate Levels
For eight HD-treated patients, the changes in the plasma
ADMA Concentrations with Respect to Renal
levels of L-arginine, DMA, and nitrate were assessed before
and after one HD session. One hour after the end of dialysis, no
HD-treated patients with atherosclerosis exhibited signifi-
cantly higher ADMA levels than did HD-treated patients with-out atherosclerosis (7.31 Ϯ 0.70 mol/L [n ϭ 22] versus3.95 Ϯ 0.52 mol/L [n ϭ 11]; P Ͻ 0.05) (Figure 3). Similarly,patients with peripheral arterial occlusive disease with normalrenal function exhibited significantly higher ADMA levelsthan did healthy control subjects (3.23 Ϯ 0.33 mol/L [n ϭ 33]versus 1.01 Ϯ 0.05 mol/L [n ϭ 37]; P Ͻ 0.05) (Figure 3). There was no significant difference in ADMA levels betweenHD-treated patients without atherosclerosis and patients withperipheral arterial occlusive disease with normal renal func-tion. A similar pattern of SDMA concentrations was observed(Table 3). Plasma L-arginine concentrations did not differ
Figure 1. Plasma asymmetric dimethylarginine (ADMA) concentra-
among control patients, patients with peripheral arterial occlu-
tions in healthy control subjects (1.0 Ϯ 0.1 mol/L, n ϭ 37), perito-
sive disease, and patients with ESRD with atherosclerosis.
neal dialysis (PD)-treated patients (2.1 Ϯ 0.4 mol/L, n ϭ 37), and
However, patients with ESRD without atherosclerosis exhib-
hemodialysis (HD)-treated patients (6.0 Ϯ 0.5 mol/L, n ϭ 43). Eachpoint represents one individual. Horizontal bars indicate the mean Ϯ
ited lower plasma L-arginine concentrations than did patients
with ESRD with atherosclerotic disease.
Our finding that DMA levels are significantly higher in
patients with ESRD than in healthy control subjects is consis-tent with the first description by Vallance et al. (7), whostudied nine HD-treated patients. They reported a mean totalDMA level of 8.7 Ϯ 0.7 mol/L. This concentration was sixtimes higher than that measured for control subjects (1.2 Ϯ 0.1
mol/L) (7). In other studies, lower concentrations of DMAwere reported. MacAllister et al. (15) found elevated ADMAand SDMA levels (0.9 Ϯ 0.1 and 3.8 Ϯ 0.4 mol/L, respec-tively) in six HD-treated patients. Anderstam et al. (16) re-ported ADMA levels of 0.6 Ϯ 0.2 mol/L in 19 patients, andno difference between PD and HD. However, in these studiesADMA and SDMA levels in control subjects were also verylow. The relative increase in DMA levels was 2.5- to sixfold inall of these studies. Comparing two treatment methods forpatients with ESRD, i.e., HD and PD, we found that PD-treatedpatients exhibited lower plasma ADMA concentrations thandid HD-treated patients. This difference may be caused bydifferences in dialytic clearance of ADMA with the two treat-ment methods or the metabolism of ADMA.
The origin of ADMA in human plasma is currently unclear. Figure 2. (A) Time course of plasma ADMA concentrations in eight
Animal studies suggest that the relatively low levels of ADMA
HD-treated patients before and 1, 5, and 18 h after a 4.5-h dialysis
and SDMA present in plasma from healthy rabbits are derived
session. Each line represents the time course of ADMA concentrations
mainly from the degradation of methylated proteins (6). Dif-
in one subject. The thick line indicates the mean Ϯ SEM. *P Ͻ 0.05
ferent methyltransferases seem to be responsible for L-arginine
by ANOVA. (B) Time course of plasma ADMA/creatinine ratios in
methylation in various tissues; the enzyme present in the vas-
eight HD-treated patients before and 1, 5, and 18 h after a 4.5-h
culature mainly yields ADMA, as judged by the observation
dialysis session. Each line represents the time course of ADMA/
that cultured human endothelial cells release more ADMA than
creatinine ratios in one subject. The thick line indicates the mean ϮSEM. *P Ͻ 0.05 by ANOVA.
Urinary excretion is the main elimination route for SDMA in
rabbits, whereas NG-monomethyl-L-arginine and ADMA are
Discussion
partly eliminated by other metabolic pathways (6). In rats,
The major findings of this study are that: (1) ADMA and
Ogawa and coworkers (19) demonstrated that 14C-labeled
SDMA are accumulated in patients with ESRD; (2) ADMA
ADMA is metabolized to citrulline by the enzyme DMA dim-
levels are significantly lower in patients with ESRD treated
ethylaminohydrolase (DDAH), which is present in various
with PD than in those treated with HD; (3) elevated ADMA
tissues of rats and human subjects (5,20,21). These tissues
levels are accompanied by low plasma levels of nitrate, the
include the kidneys, the vasculature, and other tissues in which
oxidative metabolite of NO; and (4) regardless of renal func-
this enzyme is colocalized with isoforms of NO synthase and
tion, patients with atherosclerosis have higher plasma levels of
may affect NO-mediated cell function (20,22). DDAH pres-
ADMA than those without atherosclerosis.
ence and activity have also been demonstrated in human en-
Table 2. Time course of plasma L-arginine, SDMA, SDMA/creatinine ratio as determinants of nitric oxide synthesis in 10
HD patients before, 1, 5 and 18 h after a 4.5-h dialysis sessiona
a Data are mean Ϯ SEM. Abbreviations as in Table 1.
Journal of the American Society of Nephrology
thors reported the exact time point of blood withdrawal, withrespect to the end of dialysis session. The data presented hereshow that the timing of blood withdrawal is very important forassessing the effects of HD on DMA levels.
Several studies performed in vitro suggest that ADMA, at
concentrations between 1 and 10 mol/L, inhibits NO elabo-ration by NO synthase in the presence of L-arginine in isolatedblood vessels, in cultured macrophages, and in cultured endo-
Figure 3. Plasma ADMA concentrations in healthy control subjects,
thelial cells (8,9,17,18). Because intracellular ADMA levels
patients with peripheral arterial occlusive disease (PAOD), and pa-
have been shown to be approximately one order of magnitude
tients with end-stage renal disease (ESRD) treated with HD, without
greater than the levels in conditioned cell culture media, the
or with concomitant atherosclerosis. Each point represents one indi-vidual. Horizontal bars indicate the mean
accumulation of ADMA observed in patients with ESRD may
be sufficient to cause clinically relevant inhibition of endothe-lial NO elaboration (17).
In 1992, Vallance et al. (7) hypothesized that inhibition of
dothelial cells (5,23). In isolated rat aortic rings studied ex vivo,
vascular NO formation caused by accumulated ADMA might
inhibition of DDAH activity causes vasoconstriction, which is
be responsible for cardiovascular disorders such as hyperten-
reversed by L-arginine (23). Differences in the tissue origin of
sion and atherosclerosis, which are frequently observed in
ADMA and SDMA and differences in the metabolism of these
ESRD. Since then, the presence of dysfunctional endothelium-
compounds may have contributed to the differences in plasma
dependent vasodilation in this disease has been confirmed in
ADMA and SDMA levels in this study. Further investigation
several clinical investigations: Joannides et al. (24) showed
will be needed to identify the influence of ESRD and different
that flow-induced, NO-dependent forearm vasodilation was
treatment regimens on the metabolism of DMA.
impaired in adult patients receiving HD. Kari et al. (25) foundimpaired flow-induced, NO-dependent vasodilation in children
with chronic renal failure. This was associated with elevated
The data presented here showed that 1 h after HD, there
ADMA levels and reduced levels of nitrosothiols in plasma.
were slight increases in plasma ADMA and SDMA concentra-
Moreover, Hand et al. (26) demonstrated that the defect of
tions, which were significant when the concentrations of DMA
endothelium-dependent vasodilation that was present in pa-
forms were expressed with respect to serum creatinine concen-
tients with ESRD before HD was reversed after HD sessions.
trations. This suggests that dialytic clearance for creatinine is
Furthermore, L-arginine, but not D-arginine, restored endothe-
greater than for ADMA and SDMA. Part of the increase could
lial function independently of HD. This study strongly supports
also be the result of redistribution of tissue DMA into the
the hypothesis that levels of ADMA present in the plasma of
plasma compartment during HD. Hemoconcentration did not
patients with ESRD induce clinically relevant inhibition of
play a role in this increase, because there was no significant
endothelial NO synthase activity, because competitive inhibi-
change in total protein levels during HD. At 5 h after the HD
tion of NO synthase by ADMA can be overcome by excess
session, plasma ADMA levels were decreased by 65%, com-
pared with 1 h after dialysis; levels slowly increased again until
In this study we measured the plasma concentration of
18 h after HD. This slow increase is probably attributable to
nitrate, a final oxidative metabolite of NO. Nitrate levels were
accumulation of newly synthesized DMA released into plasma.
significantly lower at baseline in HD-treated patients than in
Our data confirm the decrease in plasma ADMA concentra-
matched healthy control subjects. After HD, nitrate levels
tions of approximately 40% that was previously reported by
transiently increased and finally returned to baseline. These
Vallance et al. (7) and by Anderstam et al. (16). MacAllister et
data are in accordance with studies performed by other inves-
al. (15) found a smaller (approximately 20%) decrease in
tigators who also found evidence for reduced basal NO pro-
plasma ADMA levels after HD. However, none of those au-
duction in patients with ESRD (28) and increased NO forma-
Table 3. L-arginine and SDMA plasma concentrations in healthy controls, PAOD patients, and ESRD patients maintained on
hemodialysis without or with concomitant atherosclerosisa
a Data are mean Ϯ SEM. Results are given as mol/L. PAOD, peripheral arterial occlusive disease; ESRD, end-stage renal disease.
tion during HD (29,30). Using stable-isotope techniques,
cardiovascular disease are not proof of accelerated atheroscle-
Rhodes et al. (31) recently found that in human subjects the
rosis in patients undergoing maintenance dialysis. Many pa-
major portion of circulating nitrite/nitrate is derived directly
tients undergoing dialysis have more or less marked vascular
from the L-arginine/NO pathway. Although we cannot exclude
lesions at the start of dialysis treatment, and the risk factors
the possibility that differences in dietary nitrate intake ac-
present in the predialysis phase may be of primary importance
counted at least in part for differences in plasma nitrate levels
for the manifestation of cardiovascular disease. Multiple
between patient groups in this study, accumulated evidence
known cardiovascular risk factors have been shown to be
from these studies suggests that NO production is altered in
present in patients with ESRD (41– 44). Elevated ADMA lev-
ESRD. This is further supported by the recent finding of
els may be a newly identified, preexistent risk factor for
impaired endothelium-dependent, NO-mediated vasodilation
in patients undergoing dialysis (24 –26). Increased ADMA
In conclusion, we have demonstrated that ADMA is accu-
levels may be one important factor determining endothelial
mulated during chronic renal failure. Different dialysis treat-
ment strategies affect ADMA levels differently. The presenceof atherosclerosis is associated with higher ADMA levels in
Consequences of Reduced NO Elaboration in ESRD
patients with normal renal function, as well as in patients
Aside from volume changes during HD, acute alterations in
undergoing dialysis, but this phenomenon may be unrelated to
NO formation during HD may contribute to peridialytic BP
renal handling of ADMA. Reduced NO elaboration secondary
instability in HD-treated patients (32–34). Changes in ADMA-
to accumulation of ADMA may be an important pathogenic
induced inhibition of endothelial NO production may contrib-
factor for atherosclerosis in chronic renal failure.
ute to this phenomenon. In the long term, chronic reduction ofNO synthase activity secondary to accumulation of ADMA
Acknowledgments
may contribute to the pathogenesis of hypertension and ath-
The authors gratefully acknowledge the excellent technical assis-
erosclerosis. Chronic inhibition of NO synthesis has been
tance of T. Suchy, F.-M. Gutzki, and B. Schubert. The authors are
shown to produce hypertension (35) and to accelerate athero-
grateful to their colleagues Drs. Hilfenhaus, Jonassen, Lorenzen, Lu¨th,
sclerosis in animal models (13,36,37). Chronically elevated
Riechers, and Zaunbauer for help in collecting the clinical data from
ADMA concentrations may induce similar proatherogenic ef-
fects, like those observed in these experimental models (17).
Our group previously reported that plasma ADMA concen-
References
trations were elevated two- to threefold in patients with gen-
1. Moncada S, Higgs A: The L-arginine-nitric oxide pathway.
eralized atherosclerosis and peripheral arterial occlusive dis-
N Engl J Med 329: 2002–2012, 1993
ease (10). This increase, which was associated with reduced
2. Fo¨rstermann U, Closs EI, Pollock JS, Nakane M, Schwarz P,
urinary excretion of nitrate and cGMP, was independent of the
Gath I, Kleinert H: Nitric oxide synthase isozymes: Character-
presence of impaired renal excretory function. Moreover, we
ization, purification, molecular cloning, and functions. Hyperten-
found a twofold elevation of ADMA levels in the plasma of
sion (Dallas) 23: 1121–1131, 1994
asymptomatic young hypercholesterolemic subjects with nor-
3. Rees DD, Palmer RM, Hodson HF, Moncada S: A specific
mal renal function (38). We therefore investigated, in this
inhibitor of nitric oxide formation from L-arginine attenuates
study, whether the presence of atherosclerosis was also asso-
endothelium-dependent relaxation. Br J Pharmacol 96: 418 –
ciated with increased ADMA levels in patients with ESRD. We
found a similar relative elevation of ADMA levels in patients
4. Vallance P, Leone A, Calver A, Collier J, Moncada S: Endoge-
nous dimethylarginine as an inhibitor of nitric oxide synthesis.
with ESRD with atherosclerosis, compared with patients with
J Cardiovasc Pharmacol 20[Suppl 12]: S60 –S62, 1992
ESRD without atherosclerosis, and in patients with peripheral
5. MacAllister RJ, Fickling SA, Whitley GS, Vallance P: Metabo-
arterial occlusive disease with normal renal function, compared
lism of methylarginines by human vasculature: Implications for
with control subjects. From these data it remains unresolved
the regulation of nitric oxide synthesis. Br J Pharmacol 112:
whether patients with ESRD with atherosclerosis exhibited
higher ADMA levels because of the presence of atherosclerosis
6. McDermott JR: Studies on the catabolism of NG-methylarginine,
or whether they suffered from atherosclerosis as a consequence
NG,NG-dimethylarginine and NG,NG-dimethylarginine in the rab-
of higher ADMA levels. However, the elevation of ADMA
bit. Biochem J 154: 179 –184, 1976
levels in patients with peripheral arterial occlusive disease with
7. Vallance P, Leone A, Calver A, Collier J, Moncada S: Accumu-
normal renal function, compared with control subjects, sug-
lation of an endogenous inhibitor of nitric oxide synthesis in
gests that mechanisms other than reduced renal excretion may
chronic renal failure. Lancet 339: 572–575, 1992
8. Kurose I, Wolf R, Grisham MB, Granger DN: Effects of an
also contribute to the greater accumulation of ADMA in pa-
endogenous inhibitor of nitric oxide synthesis on postcapillary
tients with ESRD with peripheral arterial occlusive disease,
venules. Am J Physiol 268: H2224 –H2231, 1995
compared with patients with ESRD without atherosclerosis.
9. Faraci FM, Brian JEJ, Heistad DD: Response of cerebral blood
The concept of accelerated atherosclerosis in patients chroni-
vessels to an endogenous inhibitor of nitric oxide synthase. Am J
cally undergoing dialysis has been widely accepted since it was
first published (39). However, in a recent review, London and
10. Bo¨ger RH, Bode-Bo¨ger SM, Thiele W, Junker W, Alexander K,
Dru¨eke (40) argued that the high mortality rates resulting from
Fro¨lich JC: Biochemical evidence for impaired nitric oxide syn-
Journal of the American Society of Nephrology
thesis in patients with peripheral arterial occlusive disease. Cir-
27. Bo¨ger RH, Bode-Bo¨ger SM, Brandes RP, Phivthong-ngam L,
Bo¨hme M, Nafe R, Mu¨gge A, Fro¨lich JC: Dietary L-arginine
11. National Kidney Foundation DOQI: Clinical Practice Guidelines
reduces the progression of atherosclerosis in cholesterol-fed rab-
for Hemodialysis Adequacy, New York, National Kidney Foun-
bits: Comparison with lovastatin. Circulation 96: 1282–1290, 1997
28. Blum M, Yachnin T, Wollman Y, Chernihovsky T, Peer G,
12. National Kidney Foundation DOQI: Clinical Practice Guidelines
Grosskopf I, Kaplan E, Silverberg D, Cabili S, Iania A: Low
for Peritoneal Dialysis Adequacy, New York, National Kidney
nitric oxide production in patients with chronic renal failure.
13. Bode-Bo¨ger SM, Bo¨ger RH, Kienke S, Junker W, Fro¨lich JC:
29. Rysz J, Luciak M, Kedziora J, Blaszczyk J, Sibinska E: Nitric
Elevated L-arginine/dimethylarginine ratio contributes to en-
oxide release in the peripheral blood during hemodialysis. Kid-
hanced systemic NO production by dietary L-arginine in hyper-
cholesterolemic rabbits. Biochem Biophys Res Commun 219:
30. Yokokawa K, Mankus R, Saklayen MG, Kohno M, Yasunari K,
Minami M, Kano H, Horio T, Takeda T, Mandel AK: Increased
14. Tsikas D, Bo¨ger RH, Bode-Bo¨ger SM, Gutzki FM, Fro¨lich JC:
nitric oxide production in patients with hypotension during he-
Quantification of nitrite and nitrate in human urine and plasma as
modialysis. Ann Intern Med 123: 35–37, 1995
pentafluorobenzyl derivatives by gas chromatography-mass
31. Rhodes P, Leone A, Francis P, Struthers A, Moncada S: The
spectrometry using their 15N-labelled analogs. J Chromatogr B
L-arginine:nitric oxide pathway is the major source of plasma
nitrite in fasted humans. Biochem Biophys Res Commun 209:
15. MacAllister RJ, Rambausek MH, Vallance P, Williams D, Hoff-
mann KH, Ritz E: Concentration of dimethyl-L-arginine in the
32. Maiorca R: Cardiovascular problems in the choice of dialysis
plasma of patients with end- stage renal failure. Nephrol Dial
therapy for the elderly. Contrib Nephrol 106: 74 – 83, 1994
33. Maiorca R, Cancarini GC, Zubani R, Movilli E, Brunori G:
16. Anderstam B, Katzarski K, Bergstrom J: Serum levels of NG,NG-
Differing dialysis treatment strategies and outcome [Review].
dimethyl-L-arginine, a potential endogenous nitric oxide inhibitor
Nephrol Dial Transplant 11[Suppl 2]: 134 –139, 1996
in dialysis patients. J Am Soc Nephrol 8: 1437–1442, 1997
34. Maiorca R, Cancarini GC, Brunori G, Zubani R, Camerini C,
17. Bo¨ger RH, Bode-Bo¨ger SM, Tsao PS, Lin Chan JR, Cooke JP:
Manili L, Movilli E: Comparison of long-term survival between
The endogenous NO synthase inhibitor asymmetric dimethyl-
hemodialysis and peritoneal dialysis [Review]. Adv Perit Dial
arginine (ADMA) exerts pro-atherosclerotic effects in cultured
human endothelial cells [Abstract]. Circulation 96: I-1588, 1997
35. Baylis C, Mitruka B, Deng A: Chronic blockade of nitric oxide
18. Fickling SA, Leone A, Nussey SS, Vallance P, Whitley G:
synthesis in the rat produces systemic hypertension and glomer-
Synthesis of NG,NG-dimethylarginine by human endothelial
ular damage. J Clin Invest 90: 278 –281, 1992
36. Cayatte AJ, Palacino JJ, Horten K, Cohen RA: Chronic inhibition
19. Ogawa T, Kimoto M, Watanabe H, Sasaoka K: Metabolism of
of nitric oxide production accelerates neointima formation and
NG,NG- and NG,NЈG-dimethylarginine in rats. Arch Biochem Bio-
impairs endothelial function in hypercholesterolemic rabbits. Ar-terioscler Thromb 14: 753–759, 1994
20. Kimoto M, Tsuji H, Ogawa T, Sasaoka K: Detection of NG,NG-
37. Naruse K, Shimizu K, Muramatsu M, Toki Y, Miyazaki Y,
dimethylarginine dimethylaminohydrolase in the nitric oxide-
Okumura K, Hashimoto H, Ito T: Long-term inhibition of NO
generating systems of rats using monoclonal antibody. Arch
synthesis promotes atherosclerosis in the hypercholesterolemic
Biochem Biophys 300: 657– 662, 1993
21. Kimoto M, Whitley GS, Tsuji H, Ogawa T: Detection of NG,NG-
endothelium-dependent relaxation. Arterioscler Thromb 14:
dimethylarginine dimethylaminohydrolase in human tissues us-
ing a monoclonal antibody. J Biochem (Tokyo) 117: 237–238,
38. Bo¨ger RH, Bode-Bo¨ger SM, Szuba A, Tsao PS, Chan JR, Cooke
JP: Asymmetric dimethylarginine (ADMA): A novel risk factor
22. Tojo A, Welch WJ, Bremer V, Kimoto M, Kimura K, Omata M,
for endothelial dysfunction. Its role in hypercholesterolemia.
Ogawa T, Vallance P, Wilcox CS: Colocalization of demethyl-
ating enzymes and NOS and functional effects of methylargin-
39. Lindner A, Charra B, Sherrard DJ, Scribner BH: Accelerated
ines in rat kidney. Kidney Int 52: 1593–1601, 1997
atherosclerosis in prolonged maintenance hemodialysis. N Engl
23. MacAllister RJ, Parry H, Kimoto M, Ogawa T, Russell RJ,
Hodson H, Whitley GS, Vallance P: Regulation of nitric oxide
40. London GM, Dru¨eke TB: Atherosclerosis and arteriosclerosis in
synthesis by dimethylarginine dimethylaminohydrolase. Br J
chronic renal failure. Kidney Int 51: 1678 –1695, 1997
41. Attman PO, Samuelsson O, Alaupovic P: Progression of renal
24. Joannides R, Bakkali EH, Le RF, Rivault O, Godin M, Moore N,
failure: Role of apolipoprotein B-containing lipoproteins. Kidney
Fillastre JP, Thuillez C: Altered flow-dependent vasodilatation of
conduit arteries in maintenance haemodialysis. Nephrol Dial
42. Nishizawa Y, Shoji T, Kawagishi T, Morii H: Atherosclerosis in
uremia: Possible roles of hyperparathyroidism and intermediate
25. Kari JA, Donald AE, Vallance DT, Bruckdorfer KR, Leone A,
density lipoprotein accumulation. Kidney Int Suppl 62: S90 –S92,
Mullen MJ, Bunce T, Dorado B, Deanfield JE, Rees L: Physi-
ology and biochemistry of endothelial function in children with
43. Wanner C, Zimmermann J, Quaschning T, Galle J: Inflamma-
chronic renal failure. Kidney Int 52: 468 – 472, 1997
tion, dyslipidemia and vascular risk factors in hemodialysis pa-
26. Hand MF, Haynes WG, Webb DJ: Hemodialysis and L-arginine,
tients. Kidney Int Suppl 62: S53–S55, 1997
but not D-arginine, correct renal failure-associated endothelial
44. Gupta A, Robinson K: Hyperhomocysteinaemia and end stage
dysfunction. Kidney Int 53: 1068 –1077, 1998
renal disease. J Nephrol 10: 77– 84, 1997
Principal Life Over-The-Counter (OTC) Des Moines, IA 50392-0002 Insurance Company Drug List Guideline Flexible Spending Account The IRS defines eligible Over-The-Counter Drugs as pain relievers, antacids, cold remedies and allergy medications. In an effort to help define each of the categories we have established a list of examples. (This is not an all-inclusive list.) Th
Dalam menjalani kehidupan seharian, terutamanya masalah dan cabaran di tempat kerja serta masalah- masalah keluarga yang timbul dari masa ke masa, membuatkan kita rasa tertekan dan berada dalam kemurungan. Kadang-kadang kita tidak perasan pun yang kita berada dalam kemurungan, tahu-tahu akhirnya bermacam penyakit berkaitan yang muncul yang tidak sama sekali dijangka. Oleh itu, s
 Journal of the American Society of Nephrology
laboratory data were obtained from routine laboratory tests, using
Table 1. ADMA, SDMA, L-arginine, L-arginine/ADMA
ratio, and nitrate concentration as determinants ofnitric oxide synthesis in control subjects (control)
Data are presented as mean Ϯ SEM unless otherwise stated. Sta-
tistical significance was tested using ANOVA, followed by the Fisher
protected least significant difference test for comparisons betweenpatient groups. Repeated measurements were tested for statistical
significance using ANOVA and the Scheffe´ F test. Statistical signif-
icance was accepted for P Ͻ0.05.
Journal of the American Society of Nephrology
laboratory data were obtained from routine laboratory tests, using
Table 1. ADMA, SDMA, L-arginine, L-arginine/ADMA
ratio, and nitrate concentration as determinants ofnitric oxide synthesis in control subjects (control)
Data are presented as mean Ϯ SEM unless otherwise stated. Sta-
tistical significance was tested using ANOVA, followed by the Fisher
protected least significant difference test for comparisons betweenpatient groups. Repeated measurements were tested for statistical
significance using ANOVA and the Scheffe´ F test. Statistical signif-
icance was accepted for P Ͻ0.05.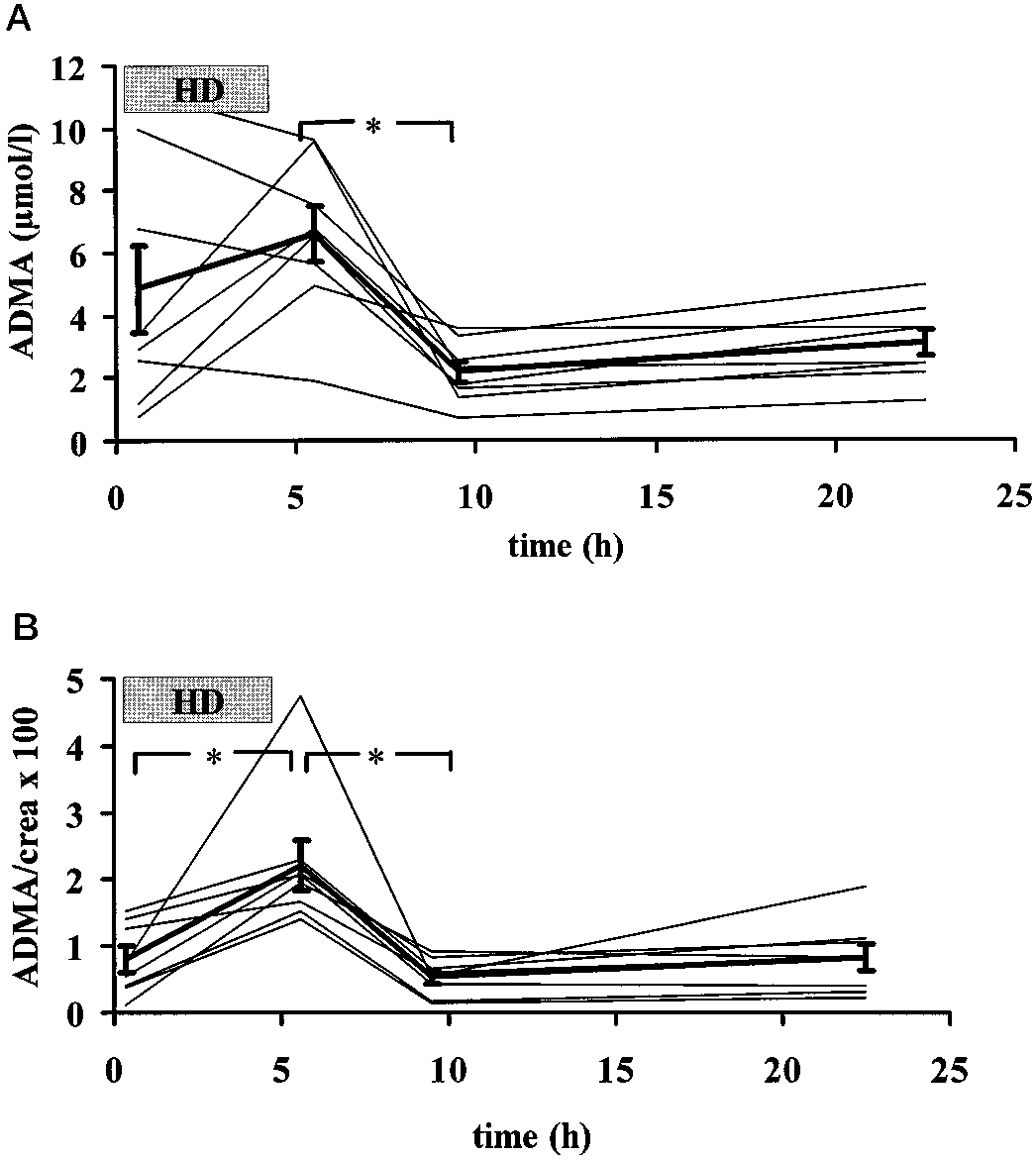 Our finding that DMA levels are significantly higher in
patients with ESRD than in healthy control subjects is consis-tent with the first description by Vallance et al. (7), whostudied nine HD-treated patients. They reported a mean totalDMA level of 8.7 Ϯ 0.7 mol/L. This concentration was sixtimes higher than that measured for control subjects (1.2 Ϯ 0.1
mol/L) (7). In other studies, lower concentrations of DMAwere reported. MacAllister et al. (15) found elevated ADMAand SDMA levels (0.9 Ϯ 0.1 and 3.8 Ϯ 0.4 mol/L, respec-tively) in six HD-treated patients. Anderstam et al. (16) re-ported ADMA levels of 0.6 Ϯ 0.2 mol/L in 19 patients, andno difference between PD and HD. However, in these studiesADMA and SDMA levels in control subjects were also verylow. The relative increase in DMA levels was 2.5- to sixfold inall of these studies. Comparing two treatment methods forpatients with ESRD, i.e., HD and PD, we found that PD-treatedpatients exhibited lower plasma ADMA concentrations thandid HD-treated patients. This difference may be caused bydifferences in dialytic clearance of ADMA with the two treat-ment methods or the metabolism of ADMA.
Our finding that DMA levels are significantly higher in
patients with ESRD than in healthy control subjects is consis-tent with the first description by Vallance et al. (7), whostudied nine HD-treated patients. They reported a mean totalDMA level of 8.7 Ϯ 0.7 mol/L. This concentration was sixtimes higher than that measured for control subjects (1.2 Ϯ 0.1
mol/L) (7). In other studies, lower concentrations of DMAwere reported. MacAllister et al. (15) found elevated ADMAand SDMA levels (0.9 Ϯ 0.1 and 3.8 Ϯ 0.4 mol/L, respec-tively) in six HD-treated patients. Anderstam et al. (16) re-ported ADMA levels of 0.6 Ϯ 0.2 mol/L in 19 patients, andno difference between PD and HD. However, in these studiesADMA and SDMA levels in control subjects were also verylow. The relative increase in DMA levels was 2.5- to sixfold inall of these studies. Comparing two treatment methods forpatients with ESRD, i.e., HD and PD, we found that PD-treatedpatients exhibited lower plasma ADMA concentrations thandid HD-treated patients. This difference may be caused bydifferences in dialytic clearance of ADMA with the two treat-ment methods or the metabolism of ADMA.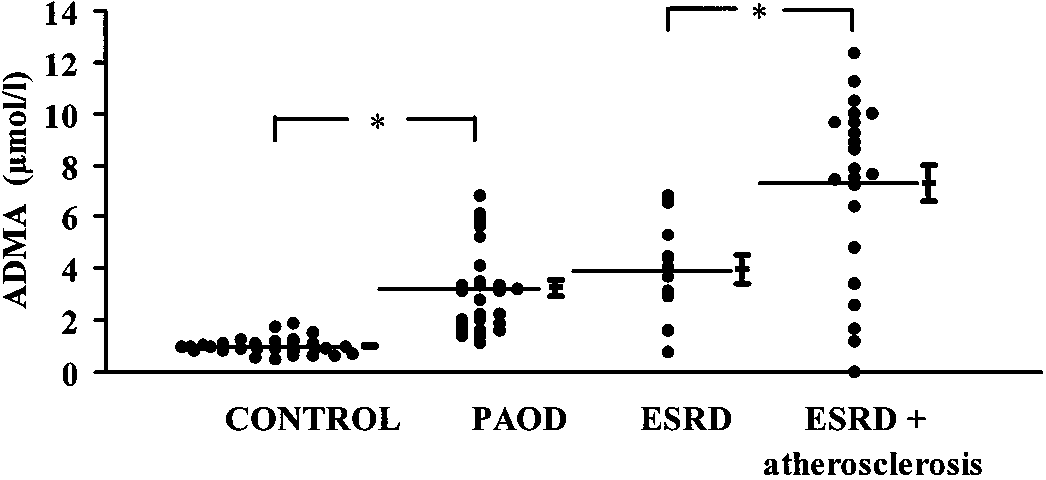 Journal of the American Society of Nephrology
thors reported the exact time point of blood withdrawal, withrespect to the end of dialysis session. The data presented hereshow that the timing of blood withdrawal is very important forassessing the effects of HD on DMA levels.
Journal of the American Society of Nephrology
thors reported the exact time point of blood withdrawal, withrespect to the end of dialysis session. The data presented hereshow that the timing of blood withdrawal is very important forassessing the effects of HD on DMA levels.