Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
Untitled
Rhinoscleroma Igor Teixeira Raymundo1, Sharlene Castanheira Pádua1, Thaís Gonçalves Pinheiro1, Ana Emília Borges de Azevedo2, Márcio Nakanishi3, Carlos Augusto Costa Pires de Oliveira4.
1) Resident Physician in Otolaryngology at University Hospital of Brasilia2) Resident Physician in Pathology at University Hospital of Brasilia3) Doctor in Otolaryngology. Otolaryngologist at University Hospital of Brasilia4) Doctorate in Medicine by University of Minnesota. Professor at University of Brasilia and Head of Otorhinolaryngology Department of University Hospital of Brasilia
University Hospital of Brasilia. Brasilia/DF - Brazil
Mailling address: Igor Teixeira Raymundo - SHIN QI 10 conj. 10 CS 08 Lago Norte - Brasília / DF - Brazil - Zip Code: 71525-100. Article received on September 3, 2009. Article accepted on October 3, 2009.
Introduction: Rhinoscleroma is a chronic granulomatous
Introdução: Rinoscleroma é uma doença infecciosa crônica
infectious disease caused by the bacterium Klebsiella
do tipo granulomatosa causada pela bactéria Klebsiella
rhinoscleromatis. It affects the respiratory tract mucosa, most
rhinoscleromatis. Acomete a mucosa do trato respiratório, mais
frequently in the nose. It is considered endemic to certain
frequentemente o nariz. É considerada endêmica em determi-
countries of Africa and Central America, but is rare in Brazil.
nadas regiões com África e América Central, porém é rara no
Nasal involvement occurs in 3 phases: catarrhal,
Brasil. O acometimento nasal ocorre em 3 fases: catarral,
granulomatous, and sclerotic. Throughout its course, the disease
granulomatosa e cicatricial. Em todo o seu curso a doença
presents nonspecific symptoms, making it difficult to diagnose.
apresenta sintomatologia inespecífica, daí a dificuldade em
Diagnosis is established by culture or by anatomopathological
ser diagnosticada. Seu diagnóstico é estabelecido através de
observation of Mikulicz cells or Russell corpuscles. Treatment
cultura ou pelo encontro de células de Mikulicz ou corpús-
consists of long-term antibiotic therapy and, occasionally,
culo de Russel no estudo anatomopatológico. O tratamento
consiste em antibioticoterapia por longo período, associada
Objective: We report a case of rhinoscleroma in a young woman
who complained of obstruction in both nostrils and persistent
Objetivo: Este relato tem por objetivo ilustrar um caso de
headache. Our intent is to enable otorhinolaryngologists to
rinoscleroma em uma paciente jovem com queixa de obstru-
diagnose this rare disease, which presents with nonspecific
ção nasal bilateral de longa data e cefaleia. O intuito é alertar
symptoms that resemble numerous pathologies of the nasal
os otorrinolaringologistas para o diagnóstico desta doença rara,
que se apresenta com sintomas inespecíficos e semelhantes
Keywords: rhinoscleroma, klebsiella infections, nasal acquired
a inúmeras patologias que acometem a região nasal.
Palavras-chave: rinoscleroma, infecções por klebsiella,deformidades adquiridas nasais.
Intl. Arch. Otorhinolaryngol., São Paulo - Brasil, v.15, n.4, p. 526-528, Oct/Nov/December - 2011.
Rhinoscleroma is a chronic granulomatous infectious
disease that compromises the respiratory tract mucosa(most frequently in the nose) and may eventually extendto the lower airways (the larynx, trachea, and bronchi). Recently, practitioners have adopted the term scleroma(1,2). It was first described by Ferdinando Von Hebra in1870 (3).
Rhinoscleroma is an infectious disease caused by
the bacterium Klebsiella rhinoscleromati, an encapsulatedgram-negative member of Enterobacteriaceae that can beisolated by culture medium. It is considered endemic tosome countries of Africa, Central America, and South
America, but is rare in Brazil (4). It is associated with somepredisposing factors such as low socioeconomic status,poor hygiene, immunodepression, and contact with infectedpatients (5).
The disease develops insidiously from the nasal
mucosa, and progression occurs in 3 phases: catarrhal(characterized by rhinorrhea, crusting, and nasal obstruction,often confused with simple rhinitis); granulomatous (wherenodes are found in the submucosa and infiltrating lesions);and sclerotic (marked by gross scar tissue, which may occurin the vestibule and/or in larynx stenosis) (1). The differential
diagnoses include neoplasms and other inflammatoryconditions such as leprosy, paracoccidioidomycosis,sarcoidosis, and Wegener granulomatosis (6).
Diagnosis can be confirmed by culture (with 50% to
60% positive specificity) or by histopathology. Treatment
On examination, she presented with significant
consists of antibiotic therapy and, in some cases, surgery
nasal pyramid bulging. Previous rhinoscopy showed a
lesion with a granulomatosis aspect, occupying both nasalcavities near the vestibule (Picture 1). Laryngoscopy wasnormal.
Computed tomography of the paranasal sinuses
showed soft tissue material occupying the lower
Otorhinolaryngology Service of Brasilia’s University Hospi-
portion of the nasal cavities without maxillary sinus
tal complained of obstruction in both nostrils since the past
involvement. There were no signs of bone destruction
3 years, significant loss of sleep, and frequent headaches in
the frontal region. She denied vocal alterations or dyspnea. She reported that 2 years ago she underwent unsuccessful
The patient underwent biopsy of the lesion under
nasal surgery for synechia resection. At that time, no biopsy
local anesthesia, and pathology revealed diffuse infiltration
of distended and vacuolated histiocytes with roundednuclei located eccentrically (Mikulicz cells) (Picture 3).
She denied drug use, nasal trauma, immunological
Giemsa, PAS, and Warthin-Starry staining revealed
deficiency, or family history of similar symptoms. She has
intracytoplasmic bacilli. These findings established the
never been a smoker or an alcoholic.
Intl. Arch. Otorhinolaryngol., São Paulo - Brasil, v.15, n.4, p. 526-528, Oct/Nov/December - 2011.
Several antibiotics can be used to treat rhinoscleroma.
Tetracycline or streptomycin is typically used for a minimumperiod of 4 weeks. Quinolones have also been proveneffective, with the advantage of fewer side effects (2). Wechose gemifloxacin in our case because it is the onlyrespiratory quinolone available freely to the patients in thisambulatory clinic.
In addition to its rarity in Brazil, the diagnosis of
rhinoscleroma can be especially difficult due to severalfactors such as differential diagnosis, limited sensitivity ofdiagnostic methods, and varying form of presentation
The treatment was tetracycline therapy (500 mg
There was partial reduction in the lesion size. We
1. Canalis FR, Zamboni L. An Interpretation of the Structural
added concomitant gemifloxacin (320 mg/day for 2 weeks).
Changes Responsible for the Chronicity of Rhinoscleroma.
After completing this antibiotic cycle, there was complete
lesion remission, although slight cicatricial stenosis of thenasal cavities remained. Given the significant clinical
2. Simons ME, Granato L, Oliveira RC, Alcantara MP.
improvement, the patient chose not to undergo further
Rinoscleroma: relato de caso. Rev Bras Otorrinolaringol. 2006,
3. Von Frisch A. The etiology of rhinoscleroma. Wien Med
The patient presented with the classical symptoms
4. Hart CA, Rao SK. Editorial: Rhinoscleroma. J Med Microbiol.
of rhinoscleroma, restricted to the nasal mucosa.
Nevertheless, the disease can affect other respiratory tractregions, such as the larynx (15-40%), nasopharynx (18–
5. Chan TV, Spiegel JH. Klebsiella rhinoscleromatis of the
43%), paranasal sinuses (26%), trachea (12%), and bronchi
membranous nasal septum. J Laryngol Otol. 2007, 121:998-
Histopathological analysis validated the diagnosis
6. Andraca R, Edson R, Kern E. Rhinoscleroma: a growing
by revealing the presence of classical Mikulicz cells
concern in the United States? Mayo Clinic experience. Mayo
(histiocytes containing bacillus) or Russell corpuscles (plas-
ma cells with hyaline degeneration). These findings areeasily recognized when the disease is in the granulomatous
7. Badia L, Lund VJ. A case of rhinoscleroma treat with
stage. The diagnosis can also be defined by culture medium,
ciprofloxacin. J Laryngol Otol. 2001, 115:220-2.
which has 50% to 60% specificity (3).
Intl. Arch. Otorhinolaryngol., São Paulo - Brasil, v.15, n.4, p. 526-528, Oct/Nov/December - 2011.
Biscayne Building 19 West Flagler Street, Suite 220 The Honorable Dr. Barbara Carey-Shuler, Chair and Members of the Board of County Commissioners OIG Investigation of Fraud Against the MDHA and Housing Recipients. Attached please find the Office of the Inspector General’s (OIG) Press Release regarding an OIG investigation of fraud perpetrated on the Miami-Dade Housing Agency (MDHA) and its


 Rhinoscleroma is a chronic granulomatous infectious
disease that compromises the respiratory tract mucosa(most frequently in the nose) and may eventually extendto the lower airways (the larynx, trachea, and bronchi).
Rhinoscleroma is a chronic granulomatous infectious
disease that compromises the respiratory tract mucosa(most frequently in the nose) and may eventually extendto the lower airways (the larynx, trachea, and bronchi).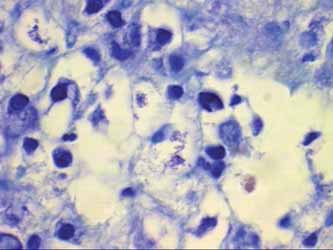 Several antibiotics can be used to treat rhinoscleroma.
Several antibiotics can be used to treat rhinoscleroma.