Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
Informe_alfa_2005_cubasept05.rtf
Becario ALFA: Sandra Lisdee Benítez Uzcátegui INFORME TÉCNICO (Re sumen general de actividades realizadas)
La becaria Sandra Benítez realizó durante su estancia de investigación en la
Universidad de Murcia estudios sobre gestión de conocimiento en organizaciones
relacionadas con dominios clínicos, particularmente en la Unidad de Oncología del
Hospital “Virgen de la Arrixaca” de la comunidad autónoma de Murcia. El trabajo de
investigación consistió en diseñar y desarrollar un Sistema Basado en Conocimiento
(SBC) o Sistema de Soporte a Decisiones (SSD) para asignar tratamientos de cáncer
de mamas. La finalidad del trabajo fue la de facilitar una herramienta de soporte que
permitiera a los oncólogos (expertos) la toma de decisiones en el momento de inferir
tratamientos de cáncer. El SSD utiliza como Base de Conocimiento (BC) protocolos
clínicos reconocidos por la comunidad científica internacional tales como National
Comprehensive Cancer Network (NCCN) y ha sido validado por los expertos de la
unidad oncológica objeto de estudio. El sistema fue diseñado de tal forma que la BC
es independiente del motor de inferencia desarrollado, lo cual permiten que pueda ser
aplicado a otros dominios y en otras organizaciones (unidades oncológicas) con
características afines. El trabajo fue realizado en conjunto con dos becarios alfa
provenientes de: Bolivia (Teddy Miranda) y México (José Luis Ochoa); y el mismo ha
sido resumido en un artículo científico denominado: “A Knowledge-based approach to
assign breast cancer treatments in oncology units” (ver anexo).
Actualmente, se tiene previsto desarrollar trabajos de investigación (dominios
tecnológicos y financieros) en la Universidad de Los Andes (ULA) a nivel de
master/tesis y doctorado, utilizando como base tecnológica (gestión del conocimiento)
el Sistema de Soporte a Decisiones desarrollado en la Universidad de Murcia -
España. Los nombres preliminares de los trabajos de investigación se mencionan a
continuación: “Modelo alternativo de gestión de sistemas financieros para el desarrollo
económico local, basado en metodologías de gestión de conocimiento”, “Sistema de
soporte a decisiones para el control de fallas en la red de datos de la ULA” y “Sistema
de control de alarmas del Centro de Servicios de Teleinformación del Consejo de
Adicionalmente, la becaria Benítez curso en la Facultad de Informática de la
Universidad de Murcia, como parte del programa de intercambio ALFA, las siguientes
materias: “Modelado y gestión de conocimiento corporativo” y “Tecnologías del
conocimiento”. Dichas materias pueden ser reconocidas como materias electivas de
los Post-grado de Simulación y Post-grado en Administración y Gerencia de la
Con lo anterior se deja constancia de que la estancia de investigación realizada en la
Universidad de Murcia, es reconocida como un aporte significativo para la Universidad
de Los Andes; ya que promueve nuevas líneas de investigación en el Post grado de la
ULA, tales como: Post-Grado de Administración y Gerencia de la Facultad de
Economía y Ciencias Sociales, Post-Grado de Simulación de la Facultad de Ingeniería,
entre otros; así como también permite facilitar la transferencia tecnológica en nuevas
áreas del conocimiento como es la Gestión de Tecnologías del Conocimiento.
OPINIÓN SOBRE EL PROGRAMA
Una vez finalizada la estancia de investigación en la Universidad de Murcia – España,
y cumpliendo lo establecido en el programa ALFA Nº II0477FA durante el periodo 2003
y 2004, se presenta a continuación los comentarios sobre el desarrollo del mismo:
1.- El programa fue una oportunidad para adquirir conocimiento en una nueva área de
investigación como es la Gestión de tecnologías del conocimiento. Particularmente, en
la universidad de Murcia se realizó estudios de gestión de conocimiento orientados a
dominios clínicos (unidades de oncológicas).
2.- El programa permitió que se estableciera un intercambio de conocimiento y
experiencias entre los investigadores que formaban parte del programa ALFA y los
investigadores de la universidad de Murcia. Este intercambio facilitó las actividades de
investigación emprendidas y en crear un ambiente de trabajo colaborativo y
3.- Los investigadores de la universidad de Murcia y el tutor encargado, facilitaron a los
becarios ALFA los recursos y materiales de apoyo necesarios para realizar los trabajos
4.- El programa tuvo en su fase inicial (Febrero 2003 a Abril 2003) inconvenientes
administrativos que afectaron el normal desarrollo de la cancelación de la beca. Sin
embargo, éstos inconvenientes se resolvieron progresivamente y los becarios
5.- El programa permitió adicionalmente que los becarios alfa desarrollarán proyectos
de cooperación entre las instituciones participantes. Algunos de los proyectos fueron
aprobados otros no, por la comunidad autónoma de Murcia y otros entes participantes.
Esto ayudo a los becarios alfa a que tuvieran la oportunidad de conocer distintas
alternativas de financiamiento de proyectos de investigación; lo cual podría beneficiar
a las instituciones participantes del programa ALFA.
6.- En la fase inicial no existió un plan explícito que aclarara las responsabilidades del
becario alfa durante la estadía de investigación. Sin embargo, en la medida que se
desarrollaba la investigación se fue despejando los compromisos y aportando los
Con lo anterior, manifiesto mi satisfacción con el programa ALFA, y considero que la
experiencia e intercambio cultural es enriquecedor y positivo para el profesional que lo
A knowledge-based approach to assign breast cancer treatments in oncology units
Teddy G. Miranda-Mena1, Sandra L. Benítez U.1, José Luis Ochoa1, Rodrigo Martínez-Béjar1,
Jesualdo Tomás Fernández-Breis 2*, Juan Salinas3
1Departamento de Ingeniería de la Información y las Comunicaciones, Universidad de
Murcia, 30071 - Espinardo (Murcia), España. Teléfono: +34 968364634 Fax: +34
emails:{tegomime@yahoo.com; sandrabenitez6@hotmail.com;
2Departamento de Informática y Sistemas, Universidad de Murcia, 30071 - Espinardo
(Murcia), España. Teléfono: +34 968364613 Fax: +34 968364151 email:
3Servicio de Oncología y Radioterapia. Hospital Virgen de la Arrixaca, 30120 – El
Palmar (Murcia), España, Teléfono: +34 968369502
Abstract. The aim of this work is to present a developed knowledge-based approach for breast cancer
treatment. This Decision Support System (DSS) uses an incremental knowledge acquisition technique
called Multiple Classification Ripple Down Rules (MCRDR) and a breast cancer treatments
knowledge base. This system integrate MCRDR inference engine and use knowledge bases to reach
advanced reasoning level during the decision making process. The knowledge base will be built from
clinical protocols, and its content will be updated by the doctor using the MCRDR component. This
DSS infers a cancer treatment from the (clinical or pathological) input data supplied by the physician
and it also allows the maintenance of the knowledge base.
Keywords : Knowledge acquisition; knowledge representation; Decision Support
System; Breast cancer; protocols and guidelines; validation and verification
1 Introduction
The detection and treatment in early stages of breast cancer in women and men are
fundamental for the survival of the patient. Given the difficulty of defining early breast
cancer, some doctors decided to focus on the diagnosis and treatment of small invasive
breast cancer. A small invasive breast cancer is defined as an invasive lesion with a
diameter of 10 mm or less–in other words (Silverstein, 1997). The past 20-30 years
have seen dramatic changes in the treatment of breast cancer. This has provoked the
generation of vast amounts of knowledge about breast cancer treatments, mainly in tacit
nature, that is, kept in the mind of oncologists. So, there is a need for mechanisms and
systems allowing for making all this knowledge explicit. The explicit knowledge of
breast cancer treatments is usually stored and organized as clinical protocols (Amrit,
2002). This is the case of the guide known as “National Comprehensive Cancer
Network” (NCCN) (http://www.nccn.org/). Many oncologists currently use NCCN as a
clinical protocol to learn about cancer treatments, because they act as digital medical
guides (explicit knowledge) through which the expert browses through a set of
algorithms showing the steps that must be followed in a specific treatment. However,
these guides do not permit the experts the extracting knowledge quickly, so becoming
not efficient when time is critical. On the other hand, when oncologists assign cancer
treatments, they use to complement the knowledge of clinical protocols with tacit
knowledge (Amrit, 2002). This tacit knowledge has been accumulated by the oncologist
with the experience of historical cases and alternative knowledge that may reinforce the
decision made. In this sense, there is a need for mechanisms to manage the (tacit and
explicit) knowledge in oncology units when cancer treatments are assigned. An
adequate solution to manage oncological knowledge might be the creation of
mechanisms, in cooperation with experts, for managing knowledge bases (Loshin,
2001) for different types of cancer treatment (i.e., breast, lung, skin, and so on). The
benefits of knowledge-based systems in medical units are very significant, such as:
decision making time reduction, historical cases-based support to the decision making,
update and maintenance of the specialized knowledge, the reuse and storing of the
corporative knowledge of the unit, and tutoring capabilities for non-experts (Hayes &
In this paper, a Decision Support System (DSS) that uses an incremental knowledge
acquisition technique called Multiple Classification Ripple Down Rules (MCRDR)
(Kang, 1996), is presented. MCRDR allows for solving multiple classification
problems. The knowledge acquisition is based on the justification provided by the
oncologist when (s)he makes a diagnosis, but no t in the explanation of the steps to draw
that diagnosis. MCRDR offers benefits for the knowledge base maintenance, because
the correction of a wrong conclusion is carried out by refining the rule that inferred the
wrong conclusion. So, the oncologist does not have to modify the MCRDR structure to
remove the wrong conclusion and to add the correct one. In this paper, MCRDR is used
as a black box whose input is clinical information and whose output is the suggestion of
a set of breast cancer treatments. The internal structure of MCRDR falls beyond the
scope of this paper. When wrong treatments are inferred or no treatment is suggested, it
is necessary to active the knowledge acquisition procedure. The MCRDR knowledge
acquisition procedure provides a natural technique through which the oncologist must
supply the system with the correct treatment and the rules explaining the decision; the
MCRDR corrects the knowledge base, allocating the rules and the treatment in their
correct positions. This makes the acquisition of a new treatment trivial. The oncologist
decides which treatments assigned by the system are wrong and must be removed.
Provided that the oncology treatments are large and explicative texts, the system must
allow experts to use this type of explanations.
Finally, this paper is structured as follows. Section 2 presents the concepts modelled in
the knowledge-based system. The construction of the breast cancer treatments
knowledge based is the target of Section 3. The Decision Support Systems is presented
in section 4. The section 5 contains the validation of the tool and finally, related work,
further work and the conclusions are put forward in Section 6.
2 Modelling the concepts of the knowledge-based system
In oncology, the concept “patient” has the following attributes: healthcare record
number, name(s), surname(s), age, gender, date of birth, and marital status. An episode
can be defined as a session in which the oncologist performs these actions: (1) analysis
of the patient’s records, diagnosis, evaluation of the stage of the cancer tumor and other
clinical and/or pathological data; (2) assignment of a primary treatment. The attributes
of the concept “episode” are: healthcare record number, episode number, type of
episode, episode date, observations, primary treatment. At this point, other concepts
such as “clinical condition”, “clinical case”, and “treatment” must be defined. A clinical
condition may be defined as the pair (description , value), for instance ( tumor size, 5
cm), and they are used by the oncologist to provide a partial description of the stage of
the disease, for instance{(age,35), (gender, male), (marital status, married), (tumor size,
5 cm),…}. A clinical case may be defined as a set of clinical conditions that provides a
comple te description of the disease stage. They are defined by the oncologist during an
episode. Clinical cases are the input data for the MCRDR inference engine. Breast
cancer treatments are defined by the oncologist as a set of rules. Each rule is defined as
a set of clinical conditions, and the rule is fired if and only if all the conditions are met.
For instance, the oncologist can assign a primary treatment “A” to a patient in case the
following clinical conditions stand: age >=50, gender=male, size tumor>=5 cm. If the
clinical conditions of the patient meet this rule, then the primary treatment A is assigned
to the patient. It must be noticed that several treatments can be assigned to the same
3 Construction of the Breast Cancer Treatments Knowledge Base
The breast cancer treatments knowledge base is the source of the knowledge-based
system. In this research work, the knowledge is built from widely recognized oncology
protocols. In particular, the oncology NCCN clinical protocols are used. There, the
cancer treatments are represented by means of algorithms. Through this work, a
knowledge base for non- invasive breast cancer treatments (DCIS) was developed. Next,
each step of the knowledge base construction is detailed:
(Step 1) Knowledge delimitation: Selection of the DICS algorithm (see Figure 2)
amongst the ones presented in the NCCN clinical protocols. Then, the knowledge to
consider is constrained and delimited by following this procedure:
Select the breast cancer stage: This stage is determined by physicians gathering
information from examinations and tests on the tumor, lymph nodes, and distant organs.
The TNM staging system, also known as the American Joint Committee on Cancer
(AJCC) system, is the most widespread to describe the growth and spread of breast
cancer. Information about the tumor, nearby lymph nodes, and distant organ metastases
is combined and a stage is assigned to specific TNM groupings, from I to IV. The
clinical stage is determined by what the doctor learns from the physical examination and
tests. The pathologic stage includes the findings of the pathologist after surgery. Most of
the time, the pathologic stage is the most important one because it is not usually known
whether the cancer has spread to lymph nodes until the pathologist examines them
under the microscope. TNM includes different categories with associated possible
conditions. The T category is based on the size and the spread to nearby tissue. The N
category is based on which of the lymph nodes near the breast, if any, are affected by
the cancer, for instance, the cancer has not spread to lymph nodes or the cancer has
spread to lymph nodes under the arm on the same side as the breast cancer. Lymph
nodes have not yet attached to one another or to the surrounding tissue. Finally, the M
category depends on the cancer spread to any distant tissues and organs, such as, no
distant cancer spread or the cancer has spread to distant organs. Once the T, N, and M
categories have been assigned, this information is combined to assign an overall stage
of 0, I, II, III, or IV. For instance, the stage 0 corresponding to Ductal Carcinoma In Situ
(DCIS) is chosen, so, the values for clinical stage are T = Tis, N = “the cancer has not
spread to lymph nodes” and M = “no distant cancer spread”.
Identifying the knowledge fractions to the breast cancer stage: For DCIS cancer, the
next six knowledge fractions are identified (see Figure 1): a) clinical stage, b)
evaluation, c) findings, d) primary treatments, e) post surgical treatment and f)
Knowledge representation. According to the given definition for treatment rules (in
section 2), the knowledge of clinical conditions and treatments for DCIS cancer is
(1) Clinical Conditions = <clinical stage + evaluation + findings + age + gender> (2) Treatment = <Primary Treatment + Post surgical Treatment + Surveillance/Follow- (Step 2) Knowledge codification: Each clinical condition and treatment for DCIS is
identified from the NCCN algorithm and assigned a code; their possible values are
determined. These are used to build the explanation tables (code, values), which are
used by the explanation module of the knowledge-based system. Table 3 shows clinical
conditions codes and treatments codes. Now, the steps to codify knowledge for DCIS
Knowledge codification: For each identified knowledge fragment, a code is assigned.
Table 1 contains examples of these codes for evaluation and primary treatment. For
instance, the code “E1” corresponds to Evaluation knowledge fraction and its value is
“Medical history and physical exam”.
Table 1. Examples of knowledge codification for DCIS Knowledge Codes Values Observations and Fraction Comments
Total mastectomy without extirpation of the lymphatic
radiation therapy of the breast, as well
ganglions with or without reconstruction of the breast
Grouping codes for construction of clinical cases: Codes of “clinical conditions” and
“treatments” are grouped for an easy knowledge base’s construction. Table 2 presents a
Table 2. Summary of codes for clinical conditions and treatments (some examples). Description (Step 3) Construction of Clinical Cases: The knowledge is consistently grouped and
contextualized in concepts to create the clinical cases with their respective clinical
conditions and treatments. Here, some examples of the possible clinical conditions and
treatments are identified for each clinical cases appearing in the algorithm, shown in
Figure 2. An example for the triple <clinical case number, clinical conditions,
treatments> might be <1,{ Stage=0, T=Tis, N=N0, M=M0, Age=Age0,
Eval=Eval1,H=H1, S=S1} , {PT2, PostT1, CST}>
(Step 4) Use of a knowledge acquisition tool: The knowledge base is created using
the knowledge acquisition module of the knowledge based system and the cases, which
have previously been identified and coded. The result of this process is a decision tree
4 The Oncology Decision Support Tool
A software tool called “Oncology Decision Support Tool” was developed by following
the principles described in previous sections. This system is comp rised of the three
modules shown in Figure 3. The first module implements the MCRDR engine to extract
the knowledge stored in cases in clinical protocols. The second module allows for
inferring clinical treatments. The third module is used to format the explanation of the
inferred treatments. The three modules were developed by using Java and MySQL. The
programming tool and the database management system were connected through the
4.1 Patients.
The tool offers the oncologist the option to assign treatments to the patient. For this
purpose, the oncologist has to select the type of cancer, then the types of cancer related
to (invasive and non- invasive) breast cancer, and finally the oncologist select the stage
LCIS or DCIS. Then, the tool displays a list of patients to treat, and if the patient no
exist the oncologist can add new patients.
4.2 Inference engine
The implementation of the inference engine is based on MCRDR. The algorithm of the
inference module is: 1) Capturing data from the clinical records of the patient; 2)
Capturing the clinical conditions of the clinical case of the patient; 3) Formatting the
clinical case and 4) inferring the treatment by using MCRDR. Figure 4 shows an
example of use of the tool for infer a treatment of a breast cancer clinical case, having
three main areas: 1) the clinical conditions according to NCCN; 2) the values of the
conditions; and 3) the clinical conditions of this clinical case, which will be the input
clinical case for the knowledge-based system. The button “Treatment Inference” allows
the oncologist for inferring the treatment that will be assigned to the input clinical case.
The result of the inference is processed by the explanation module described next.
4.3 Knowledge acquisition and maintenance
The knowledge acquisition module is based on MCRDR and it allows oncologists to
maintain the case-based knowledge base. Figure 5 shows a working session with the
tool. There, a knowledge base of breast cancer cases and treatments is created. The
background window contains the input case {T = Tis, N = N0, M = MO, Age = Age0, H
= H1, Est = Est0, Eval = Eval1}. The inference results are modified in the intermediate
window (“PosT1” and “PT2”). The foreground window shows the cases that are
involved in the result (“CST”). The tool also allows for loading and saving files from
and in different knowledge bases, so the oncologist can work with different knowledge
4.4 Explaining conclusions
The explanation module processes the conclusions produced by the knowledge-based
system inference engine. Each conclusion is an abstraction of the inferred treatment.
This module builds the explanations for the inferred treatments in natural language,
which is understandable by the expert and uses oncology terms. So, for each
conclusion, the following operations are performed: (1) retrieval of the explanation from
the base of treatments; (2) generation of the natural language explanation; (3) display to
5 Validation
The goal of the tool is the generation of a correct treatment for the patient. In particular,
given a set of patient’s clinical conditions (a clinical case), the system has to assign the
correct treatment. Determining the appropriate validation criteria is an important
consideration (Tsai, 1999). In our tool, the proposed treatment by the system implies a
critical decision, because this treatment must be assigned to a patient. Consequently, it
is only possible to validate the performance of the knowledge-based system against the
opinion of oncologists. So, reliability (Guida & Mauri, 1993) has been the validation
criterion in this case. Reliability tests checks whether the system conforms to its
specifications and if all expected requirements by oncologists are satisfied by the
system. In our case, the system was installed in the Radiotherapy service at the Hospital
“Virgen de la Arrixaca” in Murcia (Spain), and it has been used by oncologists. For the
validation, clinical test cases were generated extracting information from healthcare
records from n patients. Each clinical test case was structured according to the
description given in section 2. For each patient, m clinical conditions and their k
corresponding treatments were generated. Hence, for each clinical test case, he
following operations were performed: (1) the oncologist inputs the clinical test case to
the system; (2) a set of treatments for the clinical test case are proposed; (3) the
oncologist revises the set of treatments; (4) if the oncologist finds wrong treatments
then, he/she corrects the error; (5) the decisions of the oncologist are documented. After
some running time, some feedback was obtained from the oncologists. Apart from the
comments about the usability and friendliness of the user interface, they stated that the
systems performs correctly according to the reference protocol, but they do not
generally follow the protocol, so they would be happier with a system that combines the
protocol and their proper knowledge to suggest treatments. And this is exactly what
allows MCRDR to do. The system is still under validation before being incorporated to
daily practice but the degree of satisfaction of the oncologist increases as the system is
capable of incorporating their knowledge.
6 Conclusions
In this paper, a knowledge-based system to assign breast cancer treatments is described.
The system makes use of the incremental knowledge acquisition capabilities of
MCRDR to transform the oncological clinical protocols in a rules-based knowledge
base. This knowledge base is used to infer the treatment, so using the MCRDR
inference capabilities. The tool developed has been validated in an oncological domain
for breast cancer treatments. For this purpose, the NCCN clinical protocol was used.
The algorithm corresponding to the non- invasive breast cancer was specifically used.
The knowledge-based system intends to facilitate oncologists the maintenance of the
knowledge base, thus guaranteeing that its content is updated and efficient decisions can
be made. Some decision support systems (DSS) based on artificial intelligent
techniques such as neural networks (Zhou et al., 2002), probabilistic events networks
(Galán et al., 2002) or hybrid systems (Papadopoulos, Fotiadisb & Likas, 2002) have
been put into oncology clinical practice. The main advantage of our knowledge-based
system proposed in this paper with respect with those is the use of technologies that
facilitate an easy maintenance of the knowledge base. As further work, the following
issues should be pointed out: automatic generation of cases and treatments from clinical
protocols stored in pdf; knowledge acquisition and inference from cases with alternative
treatments and allowing oncologists to select one according to effectiveness degrees;
and multiple treatments inference from a concrete historical cases base.
Acknowledge ments
We thank the Spanish Ministry for Science and Technology for its support for the
development of the system through projects TIC2002-03879, FIT-350100-2004-32 and
TSI2004-06475-C02-02; the Seneca Foundation through the Project 00670/PI/04; and
FUNDESOCO through project FDS-2004-001-01. We also thank the European
Commission for its support under projects ALFA II0092FA and ALFA II0477FA.
References
Amrit, T. (2002). The knowledge management toolkit: orchestrating IT, strategy, and
knowledge platforms, Prentice Hall PTR, second edition p. 35-63.
Galán, S.F., Aguado, F., Diéz, F.J., & Mira, J. (2002). NasoNet, modeling the spread of
nasopharyngeal cancer with networks of probabilistic events in discrete time.
Artificial Intelligence in Medicine 25:247-264.
Guida, G., & Mauri, G. (1993). Evaluating Performance and Quality of Knowledge-
Based Systems: Foundation and Methodology, IEEE Transactions on Knowledge
Hayes Roth F., & Jacobstein N. (1994). The State of Knowledge-Bases Systes,
Comunications of the ACM, Vol 37, Nº 3, pp 27-39.
Kang, B.H. (1996). Validating Knowledge Acquisition: Multiple Classification Ripple
Down Rules. School of Copmputer Science and Engineering University of New
Loshin, D. (2001). Enterprise knowledge management: The data quality approach,
Papadopoulos, P., Fotiadisb, D.I., & Likas A. (2002). An automatic microcalcification
detection system based on a hybrid neural network classifier. Artificial
Intelligence in Medicine (25) : 149–167.
Silverstein, M. (1997). Recent advance: Diagnosis and treatment of early breast cancer.
Tsai, W.T. (1999). Vishnuvajjala, R., & Zhang, D.: Verification and Validation of
Knowledge-Based Systems. IEEE Transactions on Knowledge and Data
Zhou, Z.H., Jiang, Y., Yang, Y.B., & Chen, S.F. (2002). Lung cancer cell identification
based on artificial neural network ensembles. Artificial Intelligence in Medicine
Figures Captions
Fig. 1. Algorithm of treatments for DCIS in Non- invasive breast cancer
Fig. 4. A particular case for the Inference: 1) the clinical conditions according to
NCCN; 2) the values of the conditions; and 3) the clinical conditions of this
clinical case, which will be the input clinical case for the knowledge-based system
M e d i c a l h i s t o r y a n d p h y s i c a l e x a mM a m m o g r a m ( b o t h b r e a s t s )
P a t h o l o g y r e v i e w o f b i o p s y s a m p l e
M e a s u r e h o r m o n e r e c e p t o r o f t u m o r
1 . L u m p e c t o m y f o l l o w e d b y
1 . L u m p e c t o m y f o l l o w e d b y
2 . T o t a l m a s t e c t o m y w i t h o u t
l y m p h n o d e r e m o v a l a n d w i t h o r
l y m p h n o d e r e m o v a l a n d w i t h o r
w i t h o u t b r e a s t r e c o n s t r u c t i o n
w i t h o u t b r e a s t r e c o n s t r u c t i o n
3 . L u m p e c t o m y w i t h n o r a d i a t i o n
C o n s i d e r t a m o x i f e n f o r 5 y e a r s :
For women treated with lumpectomy with or without radiation,
( e s p e c i a l l y i f c a n c e r c o n t a i n s h o r m o n e r e c e p t o r s ) .
T o r e d u c e c a n c e r r i s k i n o t h e r b r e a s t f o r a l l w o m e n r e g a r d l e s s o f
M e d i c a l h i s t o r y a n d p h y s i c a l e x a m e v e r y 6 m o n t h s f o r 5 y e a r s , t h e n e v e r y
Y e a r l y p e l v i c e x a m f o r w o m e n t a k i n g t a m o x i f e n
Fig. 1. Algorithm of treatments for DCIS in Non-invasive breast cancer Fig. 2. Decision tree of treatments Fig. 3. Architecture of the System Fig. 4. A particular case for the Inference: 1) the clinical conditions according to NCCN; 2) the values of the conditions; and 3) the clinical conditions of this clinical case, which will be the input clinical case for the knowledge-based system Fig. 5. Knowledge acquisition session
FIRST AID ON BOARD Introduction : In coming times, for the health of all merchant seamen and others at sea, the world has been changing significantly. Continual “real-time” communication, more sophisticated tele-medicine capabilities, including video and audio components, as well as internet and satellite communication have greatly expanded the immediately available knowledge base. Alt
BPZ Uriduct 2 mg (21843) 04.11. 2010 GEBRAUCHSINFORMATION: INFORMATION FÜR DEN ANWENDER Uriduct® 2 mg Tabletten Wirkstoff: Doxazosinmesilat Lesen Sie die gesamte Packungsbeilage sorgfältig durch, bevor Sie mit der Einnahme dieses Arzneimittels beginnen. - Heben Sie die Packungsbeilage auf. Viel eicht möchten Sie diese später nochmals lesen. - Wenn Sie weitere Fragen haben, wenden S
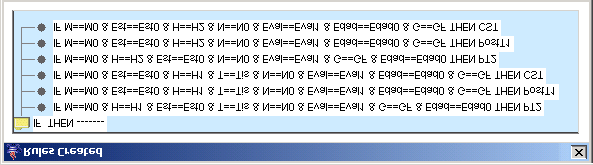 Fig. 2. Decision tree of treatments
Fig. 2. Decision tree of treatments 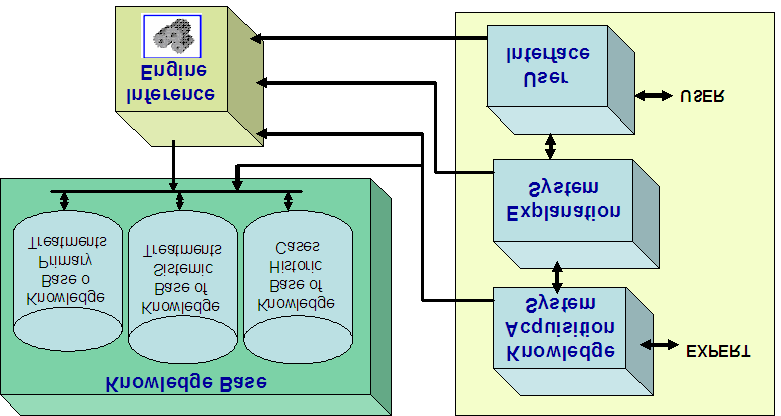 Fig. 3. Architecture of the System
Fig. 3. Architecture of the System 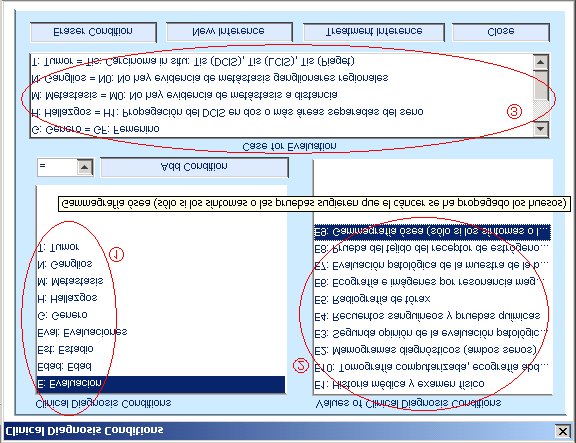 Fig. 4. A particular case for the Inference: 1) the clinical conditions according to
Fig. 4. A particular case for the Inference: 1) the clinical conditions according to 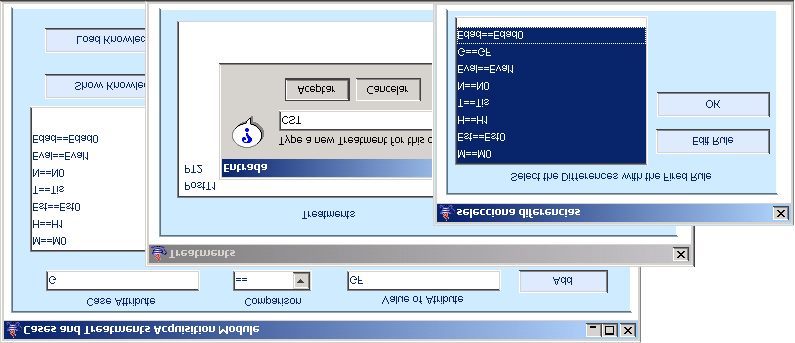 Fig. 5. Knowledge acquisition session
Fig. 5. Knowledge acquisition session