Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
Effect of methylphenidate andor levodopa coupled with physiotherapy on functional and motor recovery after stroke a randomized, doubleblind, placebocontrolled trial
Acta Neurol Scand 2011: 123: 266–273 DOI: 10.1111/j.1600-0404.2010.01395.x
Effect of methylphenidate and⁄or levodopacoupled with physiotherapy on functionaland motor recovery after stroke – arandomized, double-blind,placebo-controlled trial
Lokk J, Salman Roghani R, Delbari A. Effect of methylphenidate and ⁄ or
levodopa coupled with physiotherapy on functional and motor recovery
after stroke – a randomized, double-blind, placebo-controlled trial.
1Department of Neurobiology, Care Sciences and
Acta Neurol Scand: 2011: 123: 266–273.
Society, Karolinska Institute, Stockholm, Sweden;
2Department of Clinical Sciences, University of SocialWelfare & Rehabilitation, Tehran, Iran; 3Iranian
Objective – Amphetamine-like drugs are reported to enhance motor
Research Center on Aging, University of Social Welfare
recovery and activities of daily living (ADL) in stroke rehabilitation,
but results from trials with humans are inconclusive. This study isaimed at investigating whether levodopa (LD) and ⁄ or methylphenidate(MPH) in combination with physiotherapy could improve functionalmotor recovery and ADL in patients with stroke. Material andmethods – A randomized, double-blind, placebo-controlled trial withischemic stroke patients randomly allocated to one of four treatmentgroups of either MPH, LD or MPH+LD or placebo combined withphysiotherapy was performed. Motor function, ADL, and strokeseverity were assessed by Fugl-Meyer (FM), Barthel index (BI), and
Key words: functional recovery; levodopa;methylphenidate; motor recovery; physiotherapy;
National Institute of Health Stroke Scale (NIHSS) at baseline, 15, 90,
and 180 days respectively. Results – All participants showed recoveryof motor function and ADL during treatment and at 6-month follow-
Ahmad Delbari, Department of Neurobiology, CareSciences and Society, Division of Clinical Geriatrics,
up. There were slightly but significant differences in BI and NIHSS
Huddinge Hospital 14183, B 62 Karolinska Institute,
compared to placebo at the 6-month follow-up. Conclusion – Ischemic
chronic stroke patients having MPH and ⁄ or LD in combination with
physiotherapy showed a slight ADL and stroke severity improvement
over time. Future studies should address the issue of the optimal
therapeutic window and dosage of medications to identify thosepatients who would benefit most.
been hypothesized that pharmacological inter-
ventions administered to stroke patients may have
The burden of stroke-related disability is enormous
the potential to modulate neuronal and synaptic
and expected to increase with our aging population
plasticity (4). In human clinical trials, there were
(1). Following stroke, 40–67% of patients may
inconsistent results regarding the effect of D-amphet-
have a persisting motor deficit which may not
amine (5), selective serotonin reuptake inhibitors
improve despite ongoing physiotherapy (2).
(6), donepezil (7), or levodopa (LD) (8) on post-stroke
Many novel therapeutic treatments in stroke
recovery. Previous investigations into the effective-
rehabilitation have recently been identified and are
ness of methylphenidate (MPH) during early post
currently being investigated in clinical trials (3). An
stroke rehabilitation have shown it be a safe
area of promise in stroke rehabilitation is that of
medication with the potential of advancing recovery
Ôrehabilitation pharmacologyÕ. The potential may
(9). However, the result of a study by Restemeyera
exist for these new pharmacological interventions to
et al. (10) suggested that a single dose of LD is not
expedite and improve the recovery process. It has
sufficient for improvement in motor function after
chronic stroke. There is a dose-response effect
and Qom, Iran, when being referred to outpatient
associated with the drug (11), and its effectiveness
rehabilitation treatment at the Neurorehabilitation
is improved after administration of multiple doses
Clinic of Rofeydeh Hospital affiliated to the
on an intermittent schedule (12). Although signi-
University of Social Welfare & Rehabilitation,
ficant advances have been made in development of
Tehran, Iran from March 2006 to September
potential pharmacotherapies for stroke rehabili-
tation, definitive scientific evidence of the clinical
In the beginning, a trained physician assessed all
effectiveness of such therapies is still lacking (13).
referred patients for inclusion and exclusion crite-
Much effort has been made to identify medica-
ria. Non-eligible patients were offered the standard
tions that could increase the capacity of CNS
rehabilitation care. All therapists were trained to
regeneration and maximize the gains of rehabili-
provide a standardized rehabilitation program to
tating motor and ⁄ or cognitive functions in inca-
all patients. Two trained physicians evaluated the
pacitated patients. The results of published studies
patients completely, initially, for medical history
to date, however, are not convincing.
and general, neurologic and outcome-specific phys-ical examination. These two physicians were fol-lowing up patients at all sessions, ensuring that all
patients received standard rehabilitation and the
We hypothesized that psychostimulant drugs com-
evaluation was performed adequately. The reha-
bined with physiotherapy would improve recovery
bilitation program was usually scheduled to be
from stroke. To investigate this hypothesis, a
administered in the morning. Blood pressure and
placebo-controlled comparative drug study with
heart rate were monitored immediately before
LD and ⁄ or MPH in combination with physiother-
Ischemic patients with a paretic arm and ⁄ or legfollowing a stroke that had occurred 15–180 days
previously and being able to follow the instructions
An interventional, randomized, double-blind, pla-
cebo-controlled trial on patients with chronic
As MPH is a potentially hypertensive agent,
ischemic stroke in a 2 · 2 factorial design with
comorbidities which could be negatively affected
patients being given four different treatments. With
by the drug implicated exclusion. The exclusion
an 80% power to detect a 20% difference from
criteria were hemorrhagic stroke, myocardial
baseline to 3 and ⁄ or 6 months a significance level
infarction or angina pectoris within the last
of 0.05, one hundred patients were needed.
A computerized randomization was performed
unstable metabolic disease, sequelae of earlier
by a person not involved in the research process.
cerebral lesion, non-controlled hypertension (sys-
Full written informed consent was obtained from
tolic blood pressure ‡170 mm Hg, diastolic blood
the patients before randomization or an assent was
pressure ‡110 mm Hg), tachycardia (‡100 bpm),
taken from a relative ⁄ caregiver if the participant
major cognitive deficit (aphasia, apraxia, neglect,
was incapable of giving his ⁄ her consent. Each
concentration, and memory deficits) or psychiatric
patientÕs treatment status was kept unavailable
disease that hindered adequate participation in the
from the patients themselves, the caregivers, the
study, glaucoma, uncontrolled epilepsy, hypersen-
study physicians, and the physiotherapists. The
sitivity to MPH or LD, prominent agitation, or
patientsÕ demographic data including age, gender,
current antidepressant treatment. Patients receiv-
established stroke risk factors, paretic side, stroke
ing alfa-adrenergic antagonists or agonists, neuro-
duration, and any history of stroke were collected.
leptics, benzodiazepines, or a MAO inhibitor were
The Ministry of Health in Iran and University of
Social Welfare and Rehabilitation Ethics Commit-tee approved the study, and it was performed
according to the Declaration of Helsinki (14).
The MPH ⁄ LD ⁄ placebo drugs were randomly dis-tributed in boxes labeled 1–100. A computerized
random-number generator was used by a person
Participants were consecutively enrolled from
not involved in the study, to generate the random
eight acute care hospitals in the cities of Tehran
allocation sequence list with four groups.
The drug protocol developed for this study was
based on what was prescribed and suggested inprevious studies (15). The reasons for choosing
assessed quantitatively using the FM scale which
suggested from animal and human experiments
is developed for use in clinical rehabilitation
(16–18), they had rare side effects (19), and they
settings. It is a stroke-specific impairment index
were readily available in Iran when compared to
that is widely used for assessment of motor
recovery. Its reliability and validity are well doc-
MPH does not cause addiction, and doses of
umented (23–25). On this scale, a score of 0 means
£40 mg do not lead to insomnia or loss of
no motor function (flaccid hemiplegia) and a score
appetite in adults (13). In this four-group inter-
of 100 indicates normal motor function (divided
vention model, drug treatment was given in the
into 66 points for normal arm motor function and
form of identical white tablets of 2 · 10 mg of
34 points for normal leg motor function). Each
either MPH or placebo of identical appearance
item is scored on a 3-point ordinal scale (0 cannot
and a tablet with either 125 mg LD or placebo. It
perform, 1 performs partially, and two performs
was administrated at least 60 min before the
fully). Motor function was assessed by a physio-
training session to coincide with the timing of
therapist at baseline, at the end of the 15th session,
peak pharmacological action of drugs (20). Treat-
and at follow-up (3 and 6 months after baseline).
ments continued 5 days a week for a total of 15drug therapy sessions, a frequency often used in
Activities of daily living – Autonomy in ADL was
evaluated using the Barthel index (BI) (26). BI was
Patients received the boxes in consecutive order.
developed as a scoring technique measuring the
Placebo and drugs were prepared by a hospital
patientÕs performance in 10 ADL. The BI is
pharmacist independent of the investigators to be
considered a reliable disability scale for patients
with stroke (27). The items can be divided into one
The potential side effects of LD, including
group that is related to self-care (feeding, groom-
ing, bathing, dressing, bowel and bladder care, and
toilet use) and one group related to mobility
Also for MPH, the possible side effects were
(ambulation, transfers, and stair climbing) (15).
closely monitored including insomnia, nausea,
The maximal score is 100 in five-point increments.
or nervousness, over the first 24 h after adminis-
The lowest score is 0, representing a totally
Stroke severity – The National Institute of Health
Stroke Scale (NIHSS) is used to assess stroke
Patients received daily 45-min physical therapy
severity (29). It consists of 11 items and the
sessions. A goal-oriented approach was used in
maximum possible score is 31. A score of 0
each session to accomplish a range of activities
indicates no clinically relevant neurological abnor-
encompassed in a standard treatment: mobiliza-
mality. The NIHSS is not time-consuming to
tion, selective movements exercise, sensory-motor,
administer, taking <8 min to perform (30).
Good overall interrater reliability has been shown
in multicenter stroke trials (31), and the NIHSS
transfer, ambulatory activities, and other activities
has shown a very good sensitivity, specificity, and
of daily living (21). The theoretical framework of
accuracy in predicting clinical results at 3 months
treatment was neurodevelopmental wherein the
facilitation versus abnormal movement inhibition
(22). Increasingly, complex functional activities
these data were means, standard deviations, fre-
were introduced over time to cause progressive
quencies, and percentages used to describe age,
improvements in trunk and limb muscle control
gender, days since stroke onset, history of previous
(22). The content, not the volume of the training,
stroke, paretic side, and risk factors. Data of the
varied from each patient depending of the sever-
four treatment groups and the mean change from
ity of his or her paresis. Individuals received
baseline to 15, 90, and 180 days of BI, FM, and
additional rehabilitation treatment depending on
NIHSS were compared by ANOVA or Kruskal–
their neurological impairments such as speech
Wallis test, as appropriate. Significant results were
further investigated with post hoc test (Tukey).
One-Sample Kolmogorov–Smirnov was used to
different to the other patients with regard to
check normality of distribution of variables. The
demographic, motor function, stroke severity, or
significance level was established at 0.05.
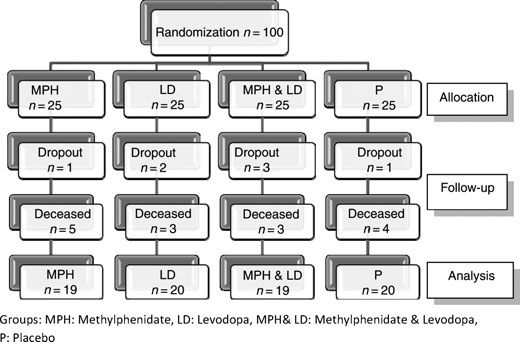
ADL. Seventy-eight patients completed the treat-ment and follow-up process with data included inthe analysis (Fig. 1). Baseline characteristics of the
patients of the respective group are presented inTable 1. Patients were compared regarding age,
gender, risk factors, stroke duration, history of
Hundred patients, diagnosed with ischemic stroke,
stroke, and paretic side. The mean age of patients
were recruited from March 2006 to September
was 64 Æ 9.8(65.4 Æ 9.2 for men and 61.8 Æ 10.6
2008. During 6-month follow-up, 15 patients died
for women), and 2.6% were younger than 45,
and seven patients dropped out, data which were
46.1% were 45–64 years of age and 51.3%
not included in the analysis. They were not
‡65 years. Through logistic regression analysis,
Figure 1. Patients flow chart, describing subjects excluded and included in treatment process; MPH, methylphenidate; LD, levodopa;MPH & LD, methylphenidate & levodopa; P, placebo.
MPH, methylphenidate; LD, levodopa; MPH & LD, methylphenidate & levodopa; P: placebo; HTN, hypertension; DM, diabetes mellitus; HLP, hyperlipidemia; HD, heart disease;SD, standard deviation.
Table 2 Mean and standard deviation of Baseline Barthel Index, Fugl-Meyer, and
Table 3 Mean and standard deviation of Baseline Barthel Index, Fugl-Meyer, and
NIHSS scores of three actively treated and placebo-treated groups
NIHSS scores in 3 and 6 months and mean changed scores of three actively -treated and placebo-treated groups
Mean changes scores: 6 months to baseline
MPH, methylphenidate; LD, levodopa; MPH & LD, methylphenidate & levodopa; P:
hypertension (HTN) was the most common risk
factor, 73.1%, followed by diabetes mellitus,
28.2%, and smoking 23.1%. Right-side paresis
Mean changes scores: 6 months to baseline
Baseline data of motor function (FM), ADL (BI),
and stroke severity (NIHSS) were homogeneous
and well balanced in all four groups. Separate
model for arm and leg motor scores in FM, self-
care, and mobility in BI revealed no significant
Mean changes scores: 6 months to baseline
differences in baseline data (Table 2).
All participants showed recovery of motor
MPH, methylphenidate; LD, levodopa; MPH & LD, methylphenidate & levodopa;
function (FM), ADL (BI), and stroke severity
(NIHSS) during the observation period. Accordingto post hoc test, there were no significant differ-ences between the active drug and placebo groups
significant, and according to a secondary power
between follow-ups (3 and 6 months) in BI, FM,
analysis, for a 80% power with 50% higher
and NIHSS scores, but there were significant
differences between groups, there would be a
between-group differences in scores of mean
need for at least 30 patients in each group.
changes of total BI and NIHSS on 6 monthsto baseline (F (3, 74) = 4.000, P = 0.011) and
(F (3, 74) = 5.728, P = 0.001), respectively, witha greater gain in the combined MPH & LD groups.
We found a significant recovery of the BI and
Table 3 shows the scores and outcome at follow-
ups for FM (total score, arm, and leg), BI scores
from baseline to 6 months compared to placebo.
(total score, self-care, and mobility), and NIHSS.
This addition of LD and ⁄ or MPH in combination
Mean improvement to first follow-up (baseline to
with physiotherapy was safe and well tolerated
3 months) of the FM was not significant, 23.9,
and indicated a slight but significant ADL
19.9, 18.7, 12.3 in the LD + MPH; LD, MPH and
improvement over time. However, all patients
placebo group, respectively. There were no signif-
improved their motor recovery and independence
icant differences between the active drug groups
as measured by the ADL as expected as most
and placebo groups between follow-ups (3 and
post-ischemic patients have a natural recovery
potential over time (15, 33). The interpretation of
adverse side effects were observed. Differences in
this result is complicated by the fact that the
gain of motor function between groups were not
corresponding mean change in the FM motor
score was not significant. It could be that the drug
or 120 min (35) or 60 min (37), as in this study,
effect has more of a fortifying effect on the
patient with ischemic stroke resulting in improved
Different drug regimes have been tested earlier;
functioning rather than a specific motor effect. As
the regime utilized here, and pioneered by others
patients in this study were recruited on average
(8, 15, 19), was driven by concern for potential
2 months after stroke, and there are large vari-
adverse effects. As we did not find any side effects,
ables in motor abilities in patients, one could
it is possible that higher and more frequent doses
assume that the motor function prior to active
are possible, as tested in experimental models by
drug intake was too ÔgoodÕ to show further
Scheidmann and Grade (8, 9) MPH is originally
improvement in some patients. The potential of
prescribed for attention deficit hyperactivity disor-
achieving further improvement and catching it
der patients and often administrated at 0.5–
through the scales could be reduced by a ceiling
0.75 mg ⁄ kg bodyweight with a maximum of
effect. However, FM seems to be more sensitive
60 mg daily. Then, it would most probably be
than the BI to changes in disability. It is well-
safe and possibly have a more powerful effect with
pronounced ceiling effect; and therefore, should
Pharmacological intervention may be beneficial in
be carefully utilized for distinguishing between
patients who have previously failed to respond to
severely affected patients and not for patients at a
motor training in isolation (42). The question of
whether using pharmacologic interventions com-
There was no significant benefit on total motor
bined with physiotherapy is of any clinical value
scores compared with physiotherapy alone when
remains unclear. In this study, we have investigated
given for 15 treatments over 15 days. The results
the effect of norepinephrine-facilitating drugs on
of this investigation are in line with those reported
ischemic stroke patients in motor function and ADL
by Sonde et al. (15), Platz (35), Restemeyer (10),
during chronic phases. LD and ⁄ or MPH were
and Sprigg (36), where patients were unable to
administered in the current study as amphetamine
demonstrate a superiority of LD and ⁄ or MPH
has documented deleterious cardiovascular side
compared to placebo. Sonde et al. (15) used an
effects (40). Catecholamine neurons have been
identical trial design as in our study and also
shown in animal models of brain injury to possibly
found no benefit in 36 patients on the FM motor
alter motor recovery (43), and drugs that antagonize
scale or the BI. In a study by Treig et al. (37), no
catecholamine receptors (e.g., haloperidol (44) and
significant differences were found between the
phenoxybenzamine (45) may have negative effects
placebo-control and amphetamine-treated group
on rehabilitation. Norepinephrine was shown to be
on either the Rivermead Motor Assessment or
the active chemical in clinical trials involving
amphetamine (46); therefore, a combination of LD
The effectiveness of amphetamine-like drugs on
and decarboxylase inhibitor was administered to
motor recovery might depend on the stage of
increase norepinephrine levels in the synapse (8).
disease. Studies that reported a beneficial effect of
MPH acts by directly stimulating release of
dopamine and norepinephrine, as well as blocking
patients early after stroke, i.e. 3–30-day post-
catecholamine reuptake (47) thereby having effects
stroke (5, 22) while in this study patients in the
on both dopaminergic and noradrenergic modula-
LD and ⁄ or MPH groups entered the trial on
average 9.3 weeks after stroke. Comparable inves-
tigations did not speak to the optimal recruitment
number of patients; we experienced similar diffi-
period or the most effective treatment timeline (36).
culty with patient recruitment that other studies
In trials that did not report an improvement in
have faced because of a wide range of exclusion
motor recovery after amphetamine treatment,
criteria (15). Although we chose wide inclusion
patient recruitment occurred commonly 3–10 days
criteria of patients with stroke, the majority of
post stroke (38–39). In a review by Goldstein, it
screened stroke patients did not meet the initial
was confirmed that pharmacotherapy success
eligibility criteria, and they were excluded from
depends heavily on proper timing of drug admin-
entering the study. However, 78 of the 100 eligible
patients terminated the study. There is significant
potential of benefits from an increase in regimented
Furthermore, timing between medication and
physical therapy (22). Fifteen 45-min sessions of
exercise therapy has been similar in positive and
physiotherapy may not have been sufficient to
negative trials, i.e. exercise therapy has been
induce or support plastic brain changes. In a study
provided within 3 h of drug administration (41),
by Scheidtmann et al. (8) stroke patients receiving
100 mg LD per day for 3 weeks improved signif-
4. Losseff N. Neurological rehabilitation of stroke. London:
icantly more than the placebo-treated control
group. Furthermore, to date, no clinical study
5. Walker-Batson D, Smith P, Curtis S, Unwin H, Greenlee R.
Amphetamine paired with physical therapy accelerates
testing amphetamine in stroke has taken into
motor recovery after stroke: further evidence. Stroke
account ischemic lesion size or localization (15, 36).
Although patients followed a standardized
6. Pariente J, Loubinoux I, Carel C et al. Fluoxetine modu-
physical therapy schedule, it was still necessary to
lates motor performance and cerebral activation of pa-
individualize therapy sessions based on patient
tients recovering from stroke. Ann Neurol 2001;50:718–29.
7. Berthier M, Pujol J, Gironell A et al. Beneficial effect of
donepezil on sensorimotor function after stroke. Am J
It remains to be clarified why the results of animal
experiments and the positive results of some clinical
8. Scheidtmann K, Fries W, Mu¨ller F, Koenig E. Effect of
trials could not be replicated in other clinical trials
levodopa in combination with physiotherapy on functional
including this study. Clinical efficacy of LD and ⁄ or
motor recovery after stroke: a prospective, randomised,double-blind study. Lancet 2001;358:787–90.
MPH in combination with physiotherapy may
9. Grade C, Redford B, Chrostowski J, Toussaint L, Black-
require higher drug doses, more frequent and
well B. Methylphenidate in early poststroke recovery: a
longer duration of treatments, improved patient
double-blind, placebo-controlled study. Arch Phys Med
selection regarding stroke localization and duration
i.e. arteries affected and appropriate time window
Restemeyer C, Weiller C, Liepert J. No effect of a levodopasingle dose on motor performance and motor excitability
in chronic stroke. A double-blind placebo-controlled cross-over pilot study. Restor Neurol Neurosci 2007;25:143–50.
11. Goldstein L. Pharmacology of recovery after stroke.
Stroke, 1990;21(11 Suppl):III139–42.
Ischemic chronic stroke patients having MPH
12. Hovda D, Feeney D. Amphetamine with experience
promotes recovery of locomotor function after unilateral
and ⁄ or LD in combination with physiotherapy
frontal cortex injury in the cat. Brain Res 1984;298:358–
showed a slight ADL and stroke severity improve-
ment over time. There were no side effects
13. Czlonkowska A, Lesniak M. Pharmacotherapy in stroke
reported, and our findings will redirect attention
rehabilitation. Expert Opin Pharmacother 2009;10:1249–
to the clinical benefits of this type of drug
14. World Medical Association Declaration of Helsinki
treatment in rehabilitation. Future studies should
abttWGA, Helsinki, Finland, last amended in 2004.
address the issue of the optimal therapeutic
WMA – Ethics Unit – Declaration of Helsinki. Available
window and dosage of medications, as well as to
from: http: ⁄ ⁄ www.wma.net ⁄ en ⁄ 30publications ⁄ 10policies ⁄
identify those patients with stroke must probable
b3 ⁄ index.html. Accessed: Jan 27, 2010.
Sonde L, Lokk J. Effects of amphetamine and ⁄ or L-dopaand physiotherapy after stroke-a blinded randomizedstudy. Acta Neurol Scand 2007;115:55–9.
16. Leonard B, McCartan D, White J, King D. Methylpheni-
date: a review of its neuropharmacological, neuropsycho-
The authors gratefully acknowledge the financial support of
logical and adverse clinical effects. Hum Psychopharmacol
Iranian Welfare Organization, Dr. Mehdi Rahgozar, and
Pouria Reza Soltani for their help in statistical analysis, Dr.
17. Kline A, Chen M, Tso-Olivas D, Feeney D. Methylpheni-
Sayed Shahaboddin Tabatabaei, Dr. Robab Sahaf, Dr. Narges
date treatment following ablation-induced hemiplegia in
Dalili and Dr. Sehar maleki for their help with data gathering
rat: experience during drug action alters effects on recovery
of function. Pharmacol Biochem Behav 1994;48:773–9.
18. Nutl J, Fellman J. Pharmacokinetics of levodopa. Clin
19. Tardy J, Pariente J, Leger A et al.
modulates cerebral post-stroke reorganization. Neuro-
20. Kempster P, Frankel J, Bovingdon M, Webster R, Lees A,
Stern G. Levodopa peripheral pharmacokinetics and
duration of motor response in ParkinsonÕs disease. Br Med
D, Black S. Enhancing recovery after stroke
with noradrenergic pharmacotherapy: a new frontier? Can
21. De Wit L, Kamsteegt H, Yadav B, Verheyden G, Feys H,
e Weerdt W. Defining the content of individual physio-
therapy and occupational therapy sessions for stroke
Broeks J, Lankhorst G, Rumping K, Prevo A. The long-term outcome of arm function after stroke: results of a
patients in an inpatient rehabilitation setting. Develop-
ment, validation and inter-rater reliability of a scoring list.
S, De Angelis D. New developments on drug
treatment rehabilitation. Clin Exp Hypertens 2006;
Gladstone D, Danells C, Armesto A et al.
coupled with dextroamphetamine for rehabilitation after
hemiparetic stroke: a randomized, double-blind, placebo-
36. Sprigg N, Willmot M, Gray L et al.
controlled trial. Stroke 2006;37:179–85.
creases blood pressure and heart rate but has no effect on
23. Fugl-Meyer A, Ja¨a¨sko¨ L, Leyman I, Olsson S, Steglind S.
motor recovery or cerebral haemodynamics in ischaemic
The post-stroke hemiplegic patient. 1. A method for eval-
stroke: a randomized controlled trial (ISRCTN 36285333).
uation of physical performance. Scand J Rehabil Med
37. Treig T, Werner C, Sachse M, Hesse S. No benefit from
24. Gladstone D, Danells C, Black S. The Fugl-Meyer
D-amphetamine when added to physiotherapy after
assessment of motor recovery after stroke: a critical review
stroke: a randomized, placebo-controlled study. Clin
of its measurement properties. Neurorehabil Neural
38. Martinsson L, Eksborg S, Wahlgren N. Intensive early
25. Duncan P, Propst M, Nelson S. Reliability of the Fugl-
physiotherapy combined with dexamphetamine treatment
Meyer assessment of sensorimotor recovery following
in severe stroke: a randomized, controlled pilot study.
cerebrovascular accident. Phys Ther 1983;63:1606–10.
26. Collin C, Wade D, Davies S, Horne V. The Barthel ADL
39. Sonde L, Nordstro¨m M, Nilsson C, Lo¨kk J, Viitanen M. A
Index: a reliability study. Disabil Rehabil 1988;10:61–3.
double-blind placebo-controlled study of the effects of
27. Mahoney FI, WD B. Functional evaluation: the Barthel
amphetamine and physiotherapy after stroke. Cerebrovasc
index. Md State Med J 1965;14:61–5.
28. Sulter G, Steen C. Use of the Barthel index and modified
40. Goldstein L. Amphetamine trials and tribulations. Stroke
Rankin scale in acute stroke trials. Stroke 1999;30:1538–
41. Crisostomo E, Duncan P, Propst M, Dawson D, Davis J.
29. Fischer U, Arnold M, Nedeltchev K et al. NIHSS score
Evidence that amphetamine with physical therapy pro-
and arteriographic findings in acute ischemic stroke.
motes recovery of motor function in stroke patients. Ann
30. Brott T, Adams H Jr, Olinger C et al. Measurements of
42. Sawaki L, Cohen L, Classen J, Davis B, Butefisch C.
acute cerebral infarction: a clinical examination scale.
Enhancement of use-dependent plasticity by D-amphet-
31. Schmulling S, Grond M, Rudolf J, Kiencke P. Training as a
43. Feeney D. The locus coeruleus and cerebral metabolism:
prerequisite for reliable use of NIH stroke scale. Stroke
recovery of function after cortical injury. Physiol Psychol
32. Muir K, Weir C, Murray G, Povey C, Lees K. Comparison
44. Feeney D, Gonzalez A, Law W. Amphetamine, haloperi-
of neurological scales and scoring systems for acute stroke
dol, and experience interact to affect rate of recovery after
prognosis. Stroke 1996;27:1817–20.
motor cortex injury. Science 1982;217:855–7.
33. Hendricks H, van Limbeek J, Geurts A, Zwarts M. Motor
45. Hovda D, Feeney D, Salo A, Boyeson M, eds. Phenoxy-
recovery after stroke: a systematic review of the literature.
benzamine but not haloperidol reinstates all motor and
Arch Phys Med Rehabil 2002;83:1629–37.
sensory deficits in cats fully recovered from sensorimotor
34. Weimar C, Kurth T, Kraywinkel K et al. Assessment of
cortex ablations. Soc Neurosci Abstr 1983;9:1001–2.
functioning and disability after ischemic stroke. Stroke
46. Sutton RL, DM F. Alpha – noradrenergic agonists and
antagonists affected recovery and maintenance of beam-
35. Platz T, Kim I, Engel U, Pinkowski C, Eickhof C, Kutzner
walking ability after sensorimotor restor. Neurol Neurosci
M. Amphetamine fails to facilitate motor performance and
to enhance motor recovery among stroke patients with
47. Biel JH, Bopp BA. Amphetamines: structure activity rela-
mild arm paresis: interim analysis and termination of a
tionships. In: Iverson L, Synder S, eds. Handbook of psy-
double blind, randomised, placebo-controlled trial. Restor
chopharmacology. New York: Plenum Press, 1979;131.
Rodica TALMACI, PhD Hematology Department – “Fundeni” Clinical Institute University of Medicine and Pharmacy “Carol Davila” BIRTH DATE and PLACE: 1973 September 9th, Chisinau, Moldova CITIZENSHIP: Romanian AREA OF INTEREST: Management of development and research activity in Molecular Biology Molecular investigation of haematological malignancies Molecular
PRODUCTION OF DRUG NANOPARTICLES OF CONTROLLABLE SIZE USING SUPERCRITICAL FLUID ANTISOLVENT TECHNIQUE WITH ENHANCED MASS TRANSFER Gupta R.B1, and Chattopadhyay P.*2 1-Auburn University, 2-Ferro Corporation. Ferro Corporation, 7500, E. Pleasant Valley Road, Independence, OH 44133. U.S.A. Email: chattopadhyayb@ferro.com Fax: (216) 7506915 ABSTRACT The use of supercritical
 One-Sample Kolmogorov–Smirnov was used to
different to the other patients with regard to
check normality of distribution of variables. The
demographic, motor function, stroke severity, or
significance level was established at 0.05.
One-Sample Kolmogorov–Smirnov was used to
different to the other patients with regard to
check normality of distribution of variables. The
demographic, motor function, stroke severity, or
significance level was established at 0.05.