Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
Doi:10.1016/j.amjcard.2003.12.056
parison with other chronic diseases and relation to
TABLE 2 Ejection Fraction–Dependent Short Form 36 Scores
functional variables. Heart 2002;87:235–241. 9. Cone DC, Niemann JT. What is the quality of life for
survivors of cardiac arrest? A prospective study. AnnEmerg Med 2000;35:201–202.
Mean Ϯ SD Median Mean Ϯ SD Median p Value
10. Dracup K, Walden JA, Stevenson LW, Brecht ML. Quality of life in patients with advanced heart failure. J Heart Lung Transplant 1992;11:273–279. 11. Gorkin L, Norvell NK, Rosen RC, Charles E, Shu-
maker SA, McIntyre KM, Capone RJ, Kostis J, Niaura
R, Woods P, et al. Assessment of quality of life as
observed from the baseline data of the Studies of LeftVentricular Dysfunction (SOLVD) trial quality-of-life
substudy. Am J Cardiol 1993;71:1069 –1073. 12. Jennett BM. Assessment of outcome after severe
brain damage: a practical scale. Lancet 1995;1:480 – 484. 13. Lombardi G, Gallagher EJ, Gennis P. Outcome of out-of-hospital cardiac arrest in New York City: the Pre-hospital arrest survival evaluation (Phase) study.
generic measures of health status (SF-36 and COOP charts). Age Ageing 1997;
14. White RD, Hankins DG, Atkinson EJ. Patient outcomes following defibril- 4. Ecochard R, Colin C, Rabilloud M, de Gevigney G, Cao D, Ducreux C,
lation with a low energy biphasic truncated exponential waveform in out-of-
Delaheye F, PRIMA Group. Indicators of myocardial dysfunction and quality of
hospital cardiac arrest. Resuscitation 2001;49:9 –14.
life, one year after acute infarction. Eur J Heart Fail 2001;3:561–568. 15. White RD, Hankins DG, Bugliosi TF. Seven years’ experience with early 5. AVID Investigators. A comparison of antiarrhythmic-drug therapy with im-
defibrillation by police and paramedics in an emergency medical services system.
plantable defibrillators in patients resuscitated from near-fatal ventricular arrhyth-
Resuscitation 1998;39:145–151.
mias. The Antiarrhythmics versus Implantable Defibrillators (AVID) Investiga-
16. Eisenberg MS, Mengert TJ. Cardiac resuscitation. N Engl J Med 2001;344:
tors. N Engl J Med 1997;337:1576 –1583. 17. Eisenberg MS, Horwood BT, Cummins RO, Reynolds-Haertle R, Hearne TR.
Connolly SJ, Gent M, Roberts RS, Dorian P, Roy D, Sheldon RS. Canadian
Cardiac arrest and resuscitation: a tale of 29 cities. Ann Emerg Med 1990;19:
implantable defibrillator study (CIDS): a randomized trial of the implantable
cardioverter defibrillator against amiodarone. Circulation 2000;101:1297–1302. 18. Kellerman AL, Hackman BB, Somes G, Kreth TK, Nail L, Dobyns P. Impact 7. Kuck KH, Cappato R, Siebels J, Ruppel R. Randomized comparison of
of first-responder defibrillation in an urban emergency medical services system.
antiarrhythmic drug therapy with implantable defibrillators in patients resusci-
tated from cardiac arrest: the Cardiac Arrest Study Hamburg (CASH). Circula-19. Myerburg RJ, Fenster J, Velez M, Rosenberg D, Lai S, Kurlansky P, Newton
S, Knox M, Castellano A. Impact of community-wide police car deployment of
8. Juenger J, Schellberg D, Kraemer S, Haunstetter A, Zugck C, Herzog W, Haass
automated external defibrillators on survival from out-of-hospital cardiac arrest.
M. Health related quality of life in patients with congestive heart failure: com-
Circulation 2002;106:1058 –1064. Effect of Carotid Atherosclerosis Screening on Risk Stratification During Primary Cardiovascular Disease Prevention
Robert L. Bard, MA, Henna Kalsi, MD, Melvyn Rubenfire, MD, Thomas Wakefield, MD,
Beverly Fex, RVT, Sanjay Rajagopalan, MD, and Robert D. Brook, MD
We investigated the effect that carotid plaque area risk, and 35% (IMT) and 27% (CPA) were identified (CPA) and intima media thickness (IMT) measure- as high risk. These tests adjust the risk strata of ments have on risk stratification in 95 patients with
>63% of patients deemed as having intermediate intermediate Framingham scores (6% to 19%). The risk by Framingham scores. ᮊ2004 by Excerpta risk status of each patient was adjusted to be low, Medica, Inc. intermediate, or high based on the results of carotid (Am J Cardiol 2004;93:1030 –1032) ultrasound. After carotid testing, 44% (IMT) and 45% (CPA) of the intermediate-risk patients were stratified as low risk, and 22% (IMT) and 40% (CPA) were stratified as high risk. Using the thresh- Measurement of carotid intima media thickness
(IMT) improves cardiovascular risk assessment,
old values derived from our laboratory, 28% (IMT)
particularly in patients with intermediate Framingham
and 45% (CPA) of patients were stratified as low
An abnormal IMT is an independent predic-tor of increased cardiovascular and it has
From the Division of Cardiovascular Medicine and Section of Vas-
been suggested that patients with values Ͼ1.0 mm
cular Surgery, Department of Surgery, University of Michigan, Ann
should be treated more aggressively than similar pa-
Arbor, Michigan. Dr. Brook’s address is: 3918 Taubman Center,
tients with a normal It is unknown how many
1500 East Medical Center Drive, Ann Arbor, Michigan 48109.
intermediate-risk patients’ therapies would change
E-mail: robdbrok@umich.edu. Manuscript received September 29,
based on carotid ultrasound results. Therefore, we
2003; revised manuscript received and accepted December 24,2003.
investigated the effect of carotid IMT and carotid
2004 by Excerpta Medica, Inc. All rights reserved.
The American Journal of Cardiology Vol. 93 April 15, 2004
TABLE 1 Clinical Characteristics of the Intermediate-risk
This project was approved by the institutional re-
view board of the University of Michigan Medical
School. We performed a retrospective analysis of the
first 200 consecutive patients who had carotid IMT
and CPA tests performed clinically. Data were ob-
tained from each patient to calculate a Framingham
Patients were risk stratifias low (Յ5%), inter-
Framingham risk scores. Only intermediate-risk pa-
tients (n ϭ 95) without established cardiovascular
disease or risk equivalents (peripheral vascular dis-
*Positive family history is equal to first-degree relative with documented
ease, diabetes mellitus, symptomatic carotid disease,
cardiovascular disease or event at Ͻ55 (male relative) or Ͻ65 (female
and aortic disease) were considered for this study
because this population’s medical management is the
†Hypertension denotes previous diagnosis of elevated blood pressure
most likely to be affected by the results of ultra-
and/or currently on antihypertensive medication.
‡Hyperlipidemia history denotes previous diagnosis of elevated serum li-
poproteins and/or currently on lipid-lowering medications.
Risk stratification was adjusted using established
and CPA9 values from the literature (IMT riskstrata: low Ͻ0.80 mm, intermediate 0.80 to 0.99 mm,high Ն1.0 mm; CPA risk strata: low 0 mm2, interme-
TABLE 2 Risk Assessment Results from the 95 Intermediate-
diate 0.01 to 12 mm2, high Ͼ12.0 mm2) and the 25th
and 75th percentile values from our laboratory. The
population of 200 patients included 62 low-, 95 inter-
mediate-, and 43 high-risk patients as defined by the
The carotid ultrasound tests were performed in an
*Framingham risk score is equal to the absolute risk of “hard” cardiovascu-
Intersocietal Commission for the Accreditation of
lar disease events (myocardial infarction, cardiovascular death, or new-onset
Vascular Laboratories-approved diagnostic vascular
unstable angina) within a 10-year period.
unit using a 7.5-MHz linear array transducer con-
nected to a Powervision ultrasounddevice (Toshiba, Inc., Tustin, Cali-fornia). On-screen measurements ofand were determined aspreviously described in the literature.
risk assessment results of the 95 in-termediate-risk
played in and respec-tively. The median Framingham riskscore was 9, the range was 6 to 18,and the 25th and 75th percentileswere 7 and 13, respectively.
rived from IMT and CPA assess-ments (using either threshold crite-rion) differed substantially from theresults of the clinical Framinghamrisk scores and respec-tively).
changed in most patients (Ն63% ofcases). IMT and CPA changed the
FIGURE 1. Effect of carotid IMT and CPA on subsequent risk stratification based on criteria from the research literature. Risk category criteria are listed above each bub- ble. Mean values for each category are listed below the bubbles in the flowchart. Absolute number and percentage of patients stratified by risk to each category are inside each bubble.
assessments differed in most patientsand respectively). IMTand CPA stratified patients identi-
plaque area (CPA) measurements on the risk stratifi-
cally in only 42% (literature review) and 38% (inter-
cation of patients with intermediate Framingham risk
nal laboratory data) of cases. However, risk stratifica-
tion differed by Ͼ1 level (e.g., low risk by IMT vs
high risk by CPA) in very few situ-ations (14% to 17% of cases).
IMT and CPA changed the risk stra-tum in most patients deemed as in-termediate risk by clinical criteriaalone. This result suggests that IMTand CPA may be useful modalities toenhance risk assessment beyond theFramingham risk score. Many pa-tients without known atheroscleroticdisease were found to have an abnor-mal IMT (22% to 35%) or CPA(27% to 40%), thus placing them inthe highest-risk category (equivalentto the risk of coronary heart disease).
values for IMT or CPA do not cur-rently exist. Different threshold cri-
FIGURE 2. Effect of carotid IMT and CPA on subsequent risk stratification based on threshold values from our vascular laboratory. Risk category criteria are listed above each bubble. Mean values for each category are listed below the bubbles in the flow- chart. Absolute number and percentage of patients stratified by risk to each category are inside each bubble.
very similar findings in our study. Additional research is necessary tobetter define clinically useful CPA
and IMT threshold values (e.g., age and risk factor
TABLE 3 Agreement Between Carotid IMT and CPA in the
adjusted risk categories) and to determine the long-
Cardiovascular Risk Stratification of Intermediate-risk Patients
term clinical outcome of tailoring medical therapy
According to Threshold Values Derived from the MedicalLiterature*
based upon risk assessment modalities. 1. Greenland P, Smith SC, Grundy SM. Improving coronary heart disease risk assessment in asymptomatic people. Role of traditional risk factors and nonin-
vasive cardiovascular tests. Circulation 2001;104:1863–1867. 2. Smith SC, Greenland P, Grundy SM. Prevention Conference V. Beyond
secondary prevention: identifying the high-risk patient for primary prevention. Executive summary. Circulation 2000;101:111–1116.
*Each value represents the number of patients (n ϭ 95). 3. Aminbakhsh A, Mancini GBJ. Carotid intima-media thickness measurements: what defines an abnormality? A systemic review. Clin Invest Med 1999;22:149 – 157. 4. Simon A, Gariepy J, Chironi G, Megnien JL, Levenson J. Intima-media thickness: a new tool for diagnosis and treatment of cardiovascular risk. J Hy- pertens 2002;20:159 –169. TABLE 4 Agreement Between Carotid IMT and CPA in the 5. Mukherjee D, Yadav JS. Carotid artery intimal-medial thickness: indicator of
Cardiovascular Risk Stratification of Intermediate-risk Patients
atherosclerotic burden and response to risk factor modification. Am Heart J
According to Threshold Values Derived from Our Vascular
6. O’Leary DH, Polak JF, Kronmal RA, Manolio TA, Burke GL, Wolfson SK. Carotid-artery intima and media thickness as a risk factor for myocardial infarc-
tion and stroke in older adults. N Engl J Med 1999;340:14 –22. 7. Hodis HN, Mack WJ, LaBree L, Selzer RH, Liu CR, Liu CL, Azen SP. The
role of carotid arterial intima-media thickness in predicting clinical coronary
events. Ann Intern Med 1998;128:262–269. 8. del Sol AI, Moons KGM, Hollander M, Hofman A, Koudstaal PJ, Grobbee DE,
Breteler MMB, Witteman JCM, Bots ML. Is carotid intima-media thickness
useful in cardiovascular disease risk assessment? The Rotterdam Study. Stroke
2001;32:1532–1538. 9. Spence JD. Ultrasound measurement of carotid plaque as a surrogate outcome
*Each value represents the number of patients (n ϭ 95).
for coronary artery disease. Am J Cardiol 2002;89(suppl):10B–16B. 1032 THE AMERICAN JOURNAL OF CARDIOLOGYா
Disease Fact Sheet Cyclospora What is Cyclospora ? Cyclospora cayetanensis is a parasite composed of one cell, too small to be seen without a microscope. The first known human cases of illness caused by Cyclospora infection (i.e., cyclosporiasis) were reported in 1979. Cases began being reported more often in the mid-1980s. In recent years, outbreaks of cyclosporiasis have been
Shin Splints Ouch! You have just started training for another event and a pain develops in the shin that never seems to go away. Sound like you? It‘s likely that you have developed one of the most common injuries seen in the lower leg. Shin pain accounts for 60% of injuries to the leg. This condition frequently occurs in high impact sports e.g. running, basketball, netball, aerobics. Commo
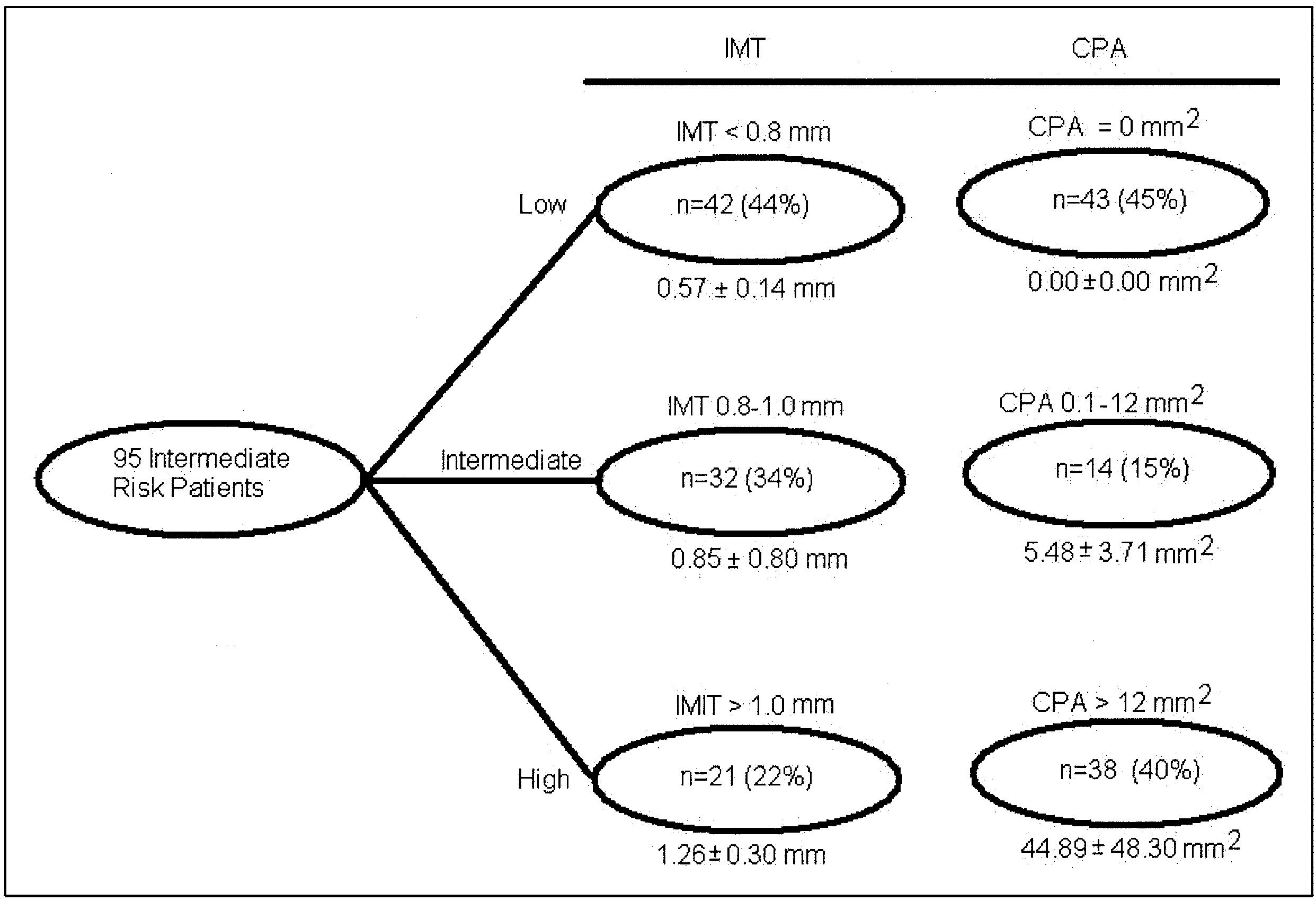 TABLE 1 Clinical Characteristics of the Intermediate-risk
TABLE 1 Clinical Characteristics of the Intermediate-risk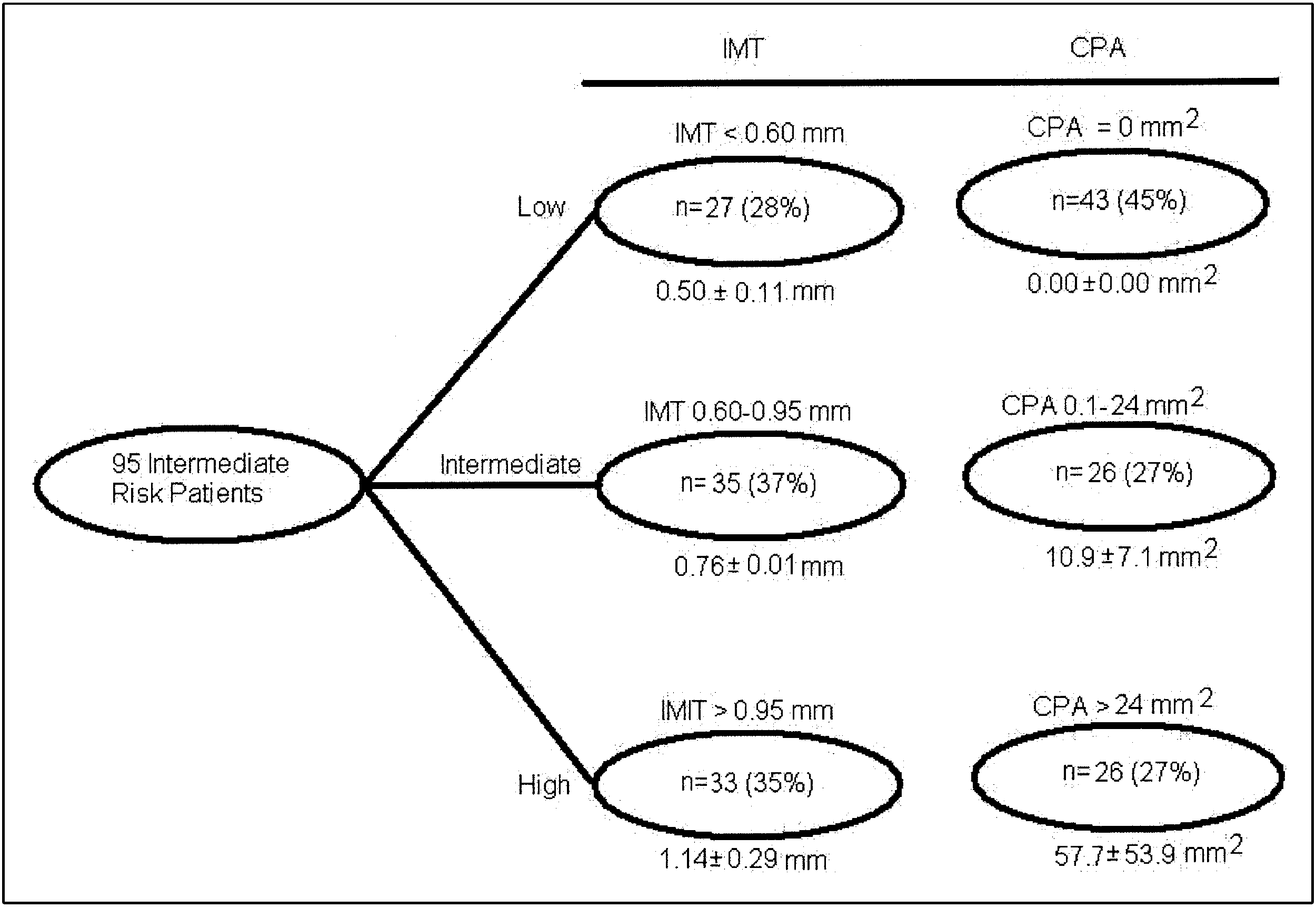 high risk by CPA) in very few situ-ations (14% to 17% of cases).
high risk by CPA) in very few situ-ations (14% to 17% of cases).