Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
Hepatitiscentral.com
Nadolol Plus Spironolactone in the Prophylaxis of First
Variceal Bleed in Nonascitic Cirrhotic Patients:
Raquel Abecasis,1 David Kravetz,1 Eduardo Fassio,2 Beatriz Ameigeiras,3 Daniel Garcia,4 Rogelio Isla,5
Graciela Landeira,2 Nora Dominguez,2 Gustavo Romero,1 Julio Argonz,1 and Ruben Terg1
Treatment with -blockers fails to decrease portal pressure in nearly 40% of cirrhotic patients. Recent studies have suggested that treatment with spironolactone reduces pressure and flow in the portal and variceal systems. This trial was designed to assess if nadolol plus spironolactone is more effective than nadolol alone to prevent the first variceal bleeding. One hundred patients with medium and large varices who had never bled and were without ascites were included in a prospective, randomized, multicenter, double-blind, placebo-controlled trial. The patients were randomized into 2 groups: 51 received nadolol plus placebo (N ؉ P) and 49 received nadolol plus spironolactone 100 mg/d (N ؉ S). Hepatic venous pressure gradient (HVPG) and activity of the renin-aldosterone system (plasma renin activity/plasma aldosterone levels) were measured in 24 patients. There were no significant differences in the appearance of variceal bleeding and ascites between groups at a mean follow-up of 22 ؎ 16 months. However, analyzing both complications together, the incidence was significantly higher in the N ؉ P group than in the N ؉ S group (39% vs. 20%; P < .04). Clinical ascites was also higher in patients in the N ؉ P group than in the N ؉ S group (21% vs. 6%; P < .04). Significant increases in plasma renin activity and plasma aldosterone levels were only observed in patients in the N ؉ S group (P < .01). The cumulative probabilities of remaining free of bleeding and ascites were similar in both groups after 70 months of follow-up. In conclusion, these results suggest that nadolol plus spironolactone does not increase the efficacy of nadolol alone in the prophylaxis of the first variceal bleeding. However, when bleeding and ascites were considered together, the combined therapy effectively reduced the incidence of both portal-hypertensive complications. (HEPATOLOGY 2003;37:359-365.)
Atpresent,nonselective-adrenergicblockers(- (HVPG)tolessthan12mmHgoradecreaseinHVPG
blockers) are the drugs of choice to prevent the
greater than 20% from basal values protects against
first variceal bleeding in cirrhotic patients with
variceal hemorrhage. However, such a decrease in portal
large esophageal varices.1 Previous studies have shown
pressure could be achieved in only 20% of patients receiv-
that reduction of the hepatic venous pressure gradient
ing -blockers.2 Moreover, 40% of treated patients donot have reduced portal pressure despite adequate
-blockade.3 Therefore, the addition of drugs to -block-
Abbreviations: HVPG, hepatic venous pressure gradient; N ϩ P, nadolol plus
ers has been investigated to achieve effective reductions in
placebo; N ϩ S, nadolol plus spironolactone.
portal pressure in a greater proportion of patients.4
From the 1Liver Unit, Hospital de Gastroenterologı´a B. Udaondo; 2Departmentof Gastroenterology, Hospital A. Posadas; 3Department of Gastroenterology, Hospi-
Recent data have shown that spironolactone signifi-
tal Ramos Mejia; 4Department of Gastroenterology, Hospital Municipal; and 5De-
cantly lowers portal and variceal pressures by reducing
partment of Gastroenterology, Hospital Israelita, Buenos Aires, Argentina.
plasma volume and splanchnic blood flow.5-9 Plasma vol-
Received June 11, 2002; accepted October 30, 2002.Supported by a grant from the Fundacio´n Argentina para el Estudio de las
ume depletion improves the hyperdynamic circulatory
state associated with the development and maintenance of
This study was presented as an oral presentation at the 2001 annual meeting of
portal hypertension.10,11 However, a correlation could
the American Gastroenterological Association.
not be shown between the decrease in circulating plasma
Address reprint requests to: Raquel Abecasis, M.D., 25 de Mayo 229, Bernal,Buenos Aires, Argentina (cp:1876). E-mail: raquelabecasisabril@hotmail.com;
volume and the decrease in HVPG.5,6,8 It has been sug-
gested that spironolactone may also have a direct vasoac-
Copyright 2003 by the American Association for the Study of Liver Diseases.
tive effect on the splanchnic circulation that is not
mediated by its antialdosteronic mechanism.12
The decrease in portal pressure achieved by adminis-
by the hospital ethical committee of each center, and pa-
tration of spironolactone could be found even in patients
tients gave their written informed consent to participate
without ascites5-7 and with or without a restricted sodium
in the investigation. Randomization was performed by
diet.6-8 The acute addition of intravenous propranolol to
tables of random numbers at the coordinating center and
long-term spironolactone therapy (100 mg/d) further de-
stratified according to participating hospitals.
creased HVPG.7 Furthermore, the combination of spi-
Protocol. After randomization, patients were treated
ronolactone and propranolol significantly reduced
with nadolol at increasing doses to reduce resting heart
variceal pressure in the subset of patients unresponsive to
rate by 25% or to 55 beats/min. Once the suitable dose
was achieved, 51 patients treated with nadolol alone (N ϩ
However, whether these hemodynamic effects have
P) received a placebo tablet and 49 patients treated with
any impact on the management of cirrhotic patients with
nadolol plus spironolactone (N ϩ S) received spironolac-
portal hypertension has never been assessed in long-term
tone at a fixed dosage of 100 mg/d for the whole study.
clinical trials. Therefore, the aim of this study was to
Spironolactone and placebo, in identical tablets, were
compare the nonselective -blocker nadolol with spi-
given by an assistant not directly involved with the pro-
ronolactone plus nadolol in the primary prophylaxis of
tocol to ensure study blindness. Treatment was adminis-
variceal bleeding. We also investigated whether the com-
tered once daily at breakfast. All patients were following
bined treatment would have a beneficial effect to prevent
an unrestricted-sodium diet. Compliance with treatment
the first appearance or recurrence of ascites.
was assessed by checking persistence of heart rate reduc-tion and counting the remaining tablets at each visit. Pa-
Patients and Methods
tients who consumed less than 85% of prescribed pillswere classified as noncompliant. Patients. From October 1993 to December 1999,
Patients were followed up monthly with a physical ex-
100 patients seen in 5 centers in Argentina were enrolled:
amination as well as measurement of heart rate and arte-
45 in Hospital B. Udaondo, 36 in Hospital Posadas, 8 in
rial blood pressure and every 2 and 6 months with
Hospital Ramos Mejı´a, 6 in Hospital Israelita, and 5 in
biochemical evaluation and abdominal ultrasonography,
Hospital Municipal. The inclusion criteria were as fol-
respectively, for the first 2 years. Thereafter, the clinical
lows: (1) a diagnosis of cirrhosis based on clinical and
evaluation was performed every 3 months and the bio-
biochemical data, ultrasonography, and liver biopsy when
chemical parameters and ultrasonography every 6 months
the procedure was not contraindicated; (2) medium and
large esophageal varices irrespective of the presence of red
A hemodynamic study was performed in 12 patients in
color signs13; (3) no history of variceal bleeding; (4) ultra-
each group before and after 2 to 3 months of treatment.
sonographic absence of ascites; and (5) no diuretic treat-
After an overnight fast and under local anesthesia, a 7F
ment for at least 1 month before inclusion in the trial. The
venous catheter introducer was placed in the right femoral
exclusion criteria were as follows: (1) contraindications to
vein by the Seldinger technique. Under fluoroscopy, a 7F
administration of -blockers (heart rate Ͻ55 beats/min,
balloon-tipped catheter (Medi Tech; Cooper Scientific
systolic blood pressure Ͻ85 mm Hg, chronic obstructive
Corp., Watertown, MA) was advanced into the main
lung disease, psychosis, insulin-dependent diabetes with
right hepatic vein. Wedge (occluded) and free hepatic
history of hypoglycemia, heart failure, and second- or
venous pressures were measured by inflating and deflating
third-degree atrioventricular blocks); (2) hepatocellular
the balloon. Afterward, a 7F Swan-Ganz catheter (Ed-
carcinoma or other malignancies; (3) serum urea and/or
wards Laboratory, Los Angeles, CA) was placed into the
creatinine levels greater than 50 and 1.5 mg/dL, respec-
pulmonary artery to measure cardiopulmonary pressures
tively; (4) bacterial infections; and (5) chronic hepatic
and cardiac output (thermodilution). Arterial pressure
encephalopathy. According to these criteria, 100 of 170
was recorded by a sphygmomanometer attached to the
consecutive patients were eligible for this study. Reasons
right arm of the patient, who was in the supine position,
for exclusion were as follows: small varices (n ϭ 10), pre-
and heart rate was derived from the continuous electro-
vious variceal bleeding (n ϭ 15), ascites (n ϭ 11), small
cardiographic monitoring. All parameters were measured
varices and ascites (n ϭ 10), contraindications to -block-
at least in triplicate, and tracings were obtained on a mul-
ers (n ϭ 12), chronic encephalopathy (n ϭ 3), tumors
tichannel recorder (Electronics Inc., Pleasantville, NY).
(n ϭ 6), and refusal to participate in the study (n ϭ 3).
Portal pressure was estimated from the HVPG, the differ-
The study was designed as a randomized, multicenter,
ence between wedge hepatic venous pressure and free he-
prospective, double-blinded trial. The protocol, which
patic venous pressure. Systemic vascular resistance (dyne ⅐
conformed with the Helsinki Declaration, was approved
s ⅐ cmϪ5) was calculated as (MAP Ϫ right atrial pressure)/
CO ϫ 80 in which MAP indicates mean arterial pressure
Table 1. General Characteristics of Included Patients
(mm Hg) and CO indicates cardiac output (L/min).14
After an overnight fast and 2 hours of bed rest, blood
samples from 12 patients in each group were taken to
measure plasma renin activity and plasma aldosterone lev-
els. Samples were collected in tubes containing ethyl-
enediaminetetraacetic acid that were placed on ice and
centrifuged at 4°C, and the plasma was frozen at Ϫ30°C
until assayed. Plasma renin activity (normal value, 0.2-2.8
ng/mL/h) and plasma aldosterone levels (normal value,
35-350 pg/mL) were measured by radioimmunoassay be-
NOTE. No significant difference was observed between groups.
fore and after 18 months of treatment.
*Range of 10-240 mg/d in both groups.
The primary end point of the trial was variceal bleed-
†Range of 3-60 months in the N ϩ P group and 1-70 months in the N ϩ S
ing. Secondary end points were appearance of ascites, ad-
verse effects requiring withdrawal from treatment, andsurvival. We diagnosed variceal bleeding when (1) a pa-
gression model. The following variables were assessed:
tient with hematemesis and/or melena showed varices ac-
type of treatment, age, sex, cause of cirrhosis, Child-Pugh
tively bleeding or with a white nipple or a clot on a varix or
score, previous ascites, and dosage of nadolol. P values less
(2) varices without another potential source of bleeding
than .05 were considered significant. Results are given as
were identified at emergency endoscopy performed
mean Ϯ SD. Data were analyzed according to the inten-
within the first 24 hours of the hemorrhage.1 These pa-
tients were treated with sclerotherapy and were with-drawn from the trial. Patients who developed either
minimal ascites, only detectable by ultrasonography, or
There were no significant differences in demographic,
clinical ascites were also withdrawn from the trial. Criteria
etiologic, clinical, and endoscopic characteristics; previ-
used for discontinuation of therapy were as follows: symp-
ous episodes of ascites; mean dosage of nadolol (78 Ϯ 61
tomatic arterial hypotension or systolic blood pressure less
mg/d); and mean follow-up (22 Ϯ 16 months) between
than 85 mm Hg; heart failure; encephalopathy without
improvement despite a low-protein diet and lactulose
During the study, 6 patients (3 in each group) were lost
therapy; bronchospasm; arrhythmia; severe painful gy-
to follow-up: 4 patients in the first 6 months and 2 pa-
necomastia; serum urea and/or creatinine levels greater
tients at 12 and 18 months, respectively.
than 50 and 1.5 mg/dL, respectively; hyponatremia (a
Five patients in the N ϩ P group and 4 patients in the
decrease in serum sodium Ͼ5 mEq/L to a level Ͻ130
N ϩ S group had to be withdrawn from treatment be-
mEq/L); or hyperkalemia (an increase Ͼ1.5 mEq/L to a
cause of adverse effects of -blockers: 3 because of brady-
arrhythmia, 3 because of bronchospasm, one because of
Statistical Analysis. Taking into account that no
symptomatic hypotension, one because of encephalopa-
long-term clinical data are available regarding the effects
thy, and one because of postural dizziness and severe as-
of spironolactone on portal pressure and that patients
thenia. Five patients were withdrawn during the first 6
with large esophageal varices treated with -blockers
months of treatment, and the remaining 4 were with-
would have an expected risk of bleeding of 31% during a
drawn after 24 months of follow-up. Two patients with
follow-up of at least 2 years, we considered it clinically
side effects of spironolactone (hyperkalemia [potassium, 6
relevant to decrease this risk to 12%. In that regard, we
mmol/L] and serum creatinine level of 1.7 mg/dL) were
estimated a sample size of 145 patients given an ␣ error of
withdrawn at 6 and 15 months of treatment. These com-
0.05 and a  error of 0.2 in a 2-tailed test. An interim
plications disappeared after discontinuation of the rele-
analysis was planned when most patients completed at
vant drug. Minor adverse effects that did not preclude
continuation with treatment included mild asthenia in 9
Comparisons between groups were performed using
patients, gynecomastia in 4 patients (2 in each group),
nested ANOVA test for quantitative variables and 2 test
dizziness in 3 patients, arterial hypotension in 7 patients,
for qualitative variables. The cumulative probabilities of
and encephalopathy stage I in 3 patients, with similar
variceal bleeding, ascites, and survival were calculated us-
distribution in both groups (Table 2).
ing the Kaplan-Meier method and compared by log-rank
Inadequate compliance was observed in 4 patients in
test. Predictors of bleeding were identified by Cox’s re-
the N ϩ P group and 5 patients in the N ϩ S group. Table 2. Side Effects During the Study
in the N ϩ S group (Table 3). There were no changes in
cardiopulmonary pressures in both groups of patients. Clinical Outcome. During follow-up, 7 patients in
the N ϩ P group (13.7%) and 3 patients in the N ϩ S
group (6%) had variceal bleeding, Eight patients bled
from esophageal varices (6 in the N ϩ P group and 2 in
the N ϩ S group), either on medium or large varices.
These patients were treated with sclerotherapy. The re-
maining 2 patients (one in each group) bled from gastric
varices, and one of them received a portocaval shunt. The
cumulative probabilities of patients to be free of bleeding
NOTE. No significant difference was observed between groups.
after 70 months of follow-up were 73% in the N ϩ Pgroup and 79% in the N ϩ S group (P ϭ NS) (Fig. 1).
Ascites developed in 13 patients in the N ϩ P group
(25%) and in 7 patients in the N ϩ S group (14%).
Hepatic and renal function test results and electrolyte
Although the incidence of ascites was similar between
levels were similar before and after treatment in both
groups, we observed that 11 patients in the N ϩ P group
groups. Treatment with nadolol alone did not produce
(21%) and 3 in the N ϩ S group (6%) had clinical ascites
any changes in plasma renin activity and plasma aldoste-
(P Ͻ .04); the number of remaining patients with mini-
rone levels. In contrast, the addition of spironolactone to
mal ascites was similar in both groups (P ϭ NS). Ascites
nadolol was associated with significant increases in both
de novo appeared in 10 of 13 patients in the N ϩ P group
and in 5 of 7 patients in the N ϩ S group (P ϭ NS). Of
Splanchnic Hemodynamics. In patients in the N ϩ P
group, HVPG decreased significantly from 16.3 Ϯ 3.7
the 19 patients with previous ascites, only 5 had a recur-
mm Hg at baseline to 14.3 Ϯ 3.5 mm Hg after treatment
rence during the study (3 in the N ϩ P group and 2 in the
(mean decrease, Ϫ11.5 Ϯ 14.4%; P Ͻ .05). Patients in
N ϩ S group). The cumulative probabilities of patients to
the N ϩ S group showed a significant reduction in HVPG
be free of ascites after 60 months of follow-up were 57%
from 17.9 Ϯ 2.7 to 15 Ϯ 3.3 mm Hg (mean decrease,
in the N ϩ P group and 73% in the N ϩ S group (P ϭ
Ϫ16 Ϯ 12.4%; P Ͻ .01). No significant differences were NS) (Fig. 2). observed when the decrease in HVPG was compared be-
Considering variceal bleeding and ascites together in
each group, 20 patients (39%) in the N ϩ P group and 10
Systemic Hemodynamics. Both groups of patients
patients (20%) in the N ϩ S group had both hypertensive
showed effective -blockade, evidenced by a significant
reduction in cardiac output and heart rate in addition to
Type of treatment, dosage of nadolol, age, sex, Child-
an increase in systemic vascular resistance. A small but
Pugh score, cause of cirrhosis, and previous episodes of
significant decrease in mean arterial pressure was observed
ascites did not have an independent predictive value of
Table 3. Biochemical Parameters and Endogenous Vasoactive System Before and After Both Treatments N ؉ P (n ؍ 51) N ؉ S (n ؍ 49)
Abbreviations: B, before both treatments; A, after both treatments. *Only measured in 12 patients in each group before and after 18 months of treatment. †P Ͻ .01. Table 4. Hemodynamic Effects of Nadolol or Nadolol Plus Spironolactone N ؉ P (n ؍ 12) N ؉ S (n ؍ 12)
NOTE. Four patients in the N ϩ P group and 5 patients in the N ϩ S group had a good HVPG response, without differences between groups. Abbreviations: HR, heart rate; MAP, mean arterial pressure; RAP, right atrial pressure; PAP, pulmonary artery pressure; PCP, pulmonary capillary pressure; CO, cardiac
output; SVR, systemic vascular resistance; WHVP, wedge hepatic venous pressure; FHVP, free hepatic venous pressure.
bleeding when tested by Cox’s multiple regression analy-
Discussion
Three patients in the N ϩ P group and one patient in
Hemodynamic studies have shown that spironolactone
the N ϩ S group died. A patient in the N ϩ P group died
may be effective in decreasing portal and variceal pres-
of variceal bleeding, and the other 2 died of lung and
sures.5,6,8,9 However, the clinical effectiveness of nadolol plus
bladder cancer, respectively. The cause of death in the
spironolactone to protect cirrhotic patients with esophageal
patient in the N ϩ S group was hepatic failure. The cu-
varices at risk for bleeding has not yet been investigated.
mulative probability of survival was 91% in the N ϩ P
We report the results of the first long-term, prospec-
group and 97% in the N ϩ S group (Fig. 3).
tive, double-blind, randomized clinical study comparing
When the results were analyzed at a mean follow-up of
the efficacy and safety of the association of nadolol and
22 Ϯ 16 months, the rates of bleeding and ascites were not
spironolactone with nadolol alone in the prophylaxis of
different between both groups of patients. Considering
first variceal bleeding in nonascitic cirrhotic patients.
that the cumulative risk of bleeding and ascites was 27%
Taking into account that a group of patients included
and 43%, respectively, in the N ϩ P group and 21% and
in this study would be treated with spironolactone, we
27% in the N ϩ S group, we estimated that a sample size
also examined its ability to prevent the development of
of 534 and 432 patients, respectively, would be necessary
to achieve a statistical difference between both groups
Previous hemodynamic studies have shown that treat-
(␣ ϭ 0.05 and  ϭ 0.20). Therefore, we decided to stop
ment with spironolactone decreased portal and variceal
the trial because we would be unable to recruit such a
pressures in human and experimental cirrhosis.5-9,15,16
Moreover, the acute intravenous addition of propranolol
Fig. 1. Cumulative probability of being free of bleeding in the N ϩ P
Fig. 2. Cumulative probability of being free of ascites in the N ϩ P
of plasma volume. However, it has also been shown thatspironolactone decreases portal and variceal pressures inpatients following a normal-sodium diet.5,9 Therefore, webelieve it is unlikely that intake of sodium plays a majorrole in our results.
We observed a low incidence of bleeding in the whole
group, particularly in patients treated with spironolactoneplus nadolol. In absolute terms, only 10 patients bled anddecreased almost by half in the combined treatmentgroup (7 vs. 3). This could be related to the inclusion ofpatients with less severe liver disease (mean Child-Pughscore of 5.9 Ϯ 1) and without ascites. In this regard, it hasbeen shown that ascites is an important prognostic factor
Fig. 3. Cumulative probability of survival in the N ϩ P and N ϩ S
increasing the risk of bleeding21 and was the most impor-
tant indicator of both bleeding and death risks in a trialcomparing patients with and without ascites treated with
to long-term administration of spironolactone further re-
propranolol.22 Vorobioff et al. observed that, after 3
duces HVPG.7 Nevens et al. showed that spironolactone
months of treatment with propranolol, portal pressure
also reduced variceal pressure in patients on long-term
decreased significantly more often in patients without as-
-blocker therapy.9 On the other hand, Sugano et al. did cites than in those with ascites.23 The effectiveness of pro-not find differences in the mean reduction of HVPG be-
pranolol in nonascitic cirrhotic patients is in keeping with
tween patients treated with low-dose transdermal nitro-
a pathophysiologic study reporting that the density of
glycerin alone or associated with spironolactone.17 In the
-adrenoreceptors in circulating mononuclear cells is re-
present trial, long-term administration of nadolol plus
duced in patients with ascites, probably resulting in a low
spironolactone produced a higher but not significant de-
hemodynamic response to -blockers.24 This evidence
crease in HVPG compared with nadolol alone (16% vs.
suggests that -blockers are more effective in reducing
11.5%). This effect could be related to a decrease in ef-
portal hypertension in compensated cirrhotic patients,
fective intravascular volume suggested by the significant
even more when administered at early stages before the
increases in plasma renin activity and plasma aldosterone
levels observed in patients treated with the combined
Although the development of ascites was similar in
therapy. Another possible explanation for the reduction
both groups, the subset of patients with clinical evidence
in HVPG could be a decrease in the intrahepatic vascular
of this complication was significantly higher in the group
resistance produced by the calcium channel blocking ac-
treated with nadolol alone than in those who received the
tion of spironolactone.12,18 This probable vasodilator
combined treatment. Ascites de novo was reduced by 50%
property of spironolactone would explain why short-term
in patients who received combined treatment compared
or long-term administration of furosemide did not pro-
with those treated with nadolol alone (12% vs. 25%);
duce any significant changes in HVPG, total blood vol-
however, this difference was not significant. The inci-
ume, or azygos blood flow despite a decrease in cardiac
dence of ascites de novo in patients treated with nadolol
alone was similar to that reported in long-term trials on
The different results of the current trial compared with
primary prophylaxis of variceal bleeding with -blockers
other hemodynamic studies could be attributed to the fact
ranging from 27% to 32%.22,26,27 All of these findings
that our patients followed an unrestricted-sodium diet.
show that a trend toward the association of nadolol and
We decided on this diet by taking into account the study
spironolactone may be useful in the prevention of clinical
design, which included patients without ascites and their
ascites that should be treated with sodium restriction and
poor compliance with a low-sodium diet for a long time.
diuretics, whereas minimal ascites, only detectable by ul-
It had been shown in portal-hypertensive rats20 and in
trasonography, does not necessitate specific treatment.28
cirrhotic patients6 that restriction of sodium produces a
A further analysis, according to the occurrence of
significant reduction in plasma volume and improves the
variceal bleeding and ascites in each group of patients,
hyperdynamic circulation associated with cirrhosis. In
showed that the incidence of both complications was sig-
this trial, treatment with spironolactone probably did not
nificantly higher in patients treated with nadolol alone
result in additional effects because the administered
than in those treated with spironolactone plus nadolol.
amount of sodium blunted a more pronounced decrease
This interesting finding supports the concept that the
prevention of ascites would increase the efficacy of nado-
9. Nevens F, Lijnen P, VanBilloen H, Fevery J. The effects of long-term
treatment with spironolactone on variceal pressure in patients with portalhypertension without ascites. HEPATOLOGY 1996;23:1047-1052.
Although withdrawals due to adverse effects were sim-
10. Colombato L, Albillos A, Groszmann R. Temporal relationship of periph-
ilar in both groups, most were related to -blockade
eral vasodilatation, plasma volume expansion and the hyperdynamic cir-
rather than to spironolactone (9 vs. 2). Only 2 patients in
culatory state in portal hypertension rats. HEPATOLOGY 1992;15:323-328.
11. Schrier R, Arroyo V, Bernardi M, Epstein M, Henriksen J, Rodes J. Pe-
the combined treatment group developed an increase in
ripheral arterial vasodilation hypothesis: a proposal for the initiation of
serum creatinine and urea levels associated, in one of the
renal sodium and water retention in cirrhosis. HEPATOLOGY 1988;8:1151-
patients, with hyperkalemia that improved with discon-
12. Dacquet C, Loirand G, Mironneau C, Mironneau J, Pacaud P. Spirono-
tinuation of the diuretic drug. Despite the concern that
lactone inhibition of contraction and calcium channels in rat portal vein.
serious gynecomastia might be a problem in male patients
receiving spironolactone therapy,9 none of the patients in
13. Japanese Research Society for Portal Hypertension. The general rules for
recording endoscopic findings on esophageal varices. Jpn J Surg 1980;10:
this trial had to be withdrawn for this adverse event.
In conclusion, these preliminary results suggest that
14. Romero G, Kravetz D, Argonz J, Bildozola M, Suarez A, Terg R. Terlip-
nadolol plus spironolactone is not more effective than
ressin is more effective in decreasing variceal pressure than portal pressurein cirrhotic patients. J Hepatol 2000;32:419-425.
nadolol alone in preventing the first variceal bleeding in
15. Van De Casteele M, Van Roel G, Nevens F, Fevery J. Effects of varying
nonascitic cirrhotic patients. However, this combined
doses of spironolactone without and with nitrates on portal vein pressure
treatment would prevent both complications of portal
and kidney function in partial portal vein ligated rats. HEPATOLOGY 1996;24:1492-1496.
hypertension, particularly the appearance of clinical as-
16. Oberti F, Pilette C, Rifflet H, Maiga MY, Moreau A, Gallois Y, Girault A,
cites. Future clinical trials with a greater number of pa-
et al. Effects of simvastatin, pentoxifylline and spironolactone on hepatic
tients will be necessary to define the role of spironolactone
fibrosis and portal hypertension in rats with bile duct ligation. J Hepatol1997;26:1363-1371.
in the prophylaxis of the first variceal bleeding.
17. Sugano S, Suzuki T, Nishio M, Makino H, Okajima T. Chronic splanch-
nic hemodynamic effects of low-dose transdermal nitroglycerin vs low-
dose transdermal nitroglycerin plus spironolactone in patients with
cirrhosis. Dig Dis Sci 1997;42:529-535.
18. Mironneau J. Calcium channel antagonist effects of spironolactone, an
References
aldosterone antagonist. Am J Cardiol 1990;65:7K-8K.
19. Sogni P, Soupison T, Moreau R, Le Moine O, Bacq Y, Hadengue A,
1. De Franchis R. Portal hypertension. Baveno III Consensus Statements.
Lebrec D. Hemodynamic effects of acute administration of furosemide in
Primary prophylaxis. Session 5. Oxford: Blackwell Science, 2001:127-131.
patients with cirrhosis receiving -adrenergic antagonist. J Hepatol 1994;
2. Groszmann RJ, Bosch J, Grace N, Conn HO, Garcı´a-Tsao G, Navasa M,
Alberts J, et al. Hemodynamic events in a prospective randomized trial of
20. Genecin P, Polio J, Groszmann R. Na restriction blunts expansion of
propranolol vs placebo in the prevention of the first variceal hemorrhage.
plasma volume and ameliorates hyperdynamic circulation in portal hyper-tension. Am J Physiol 1990;259:G498-G503.
21. Conn HO, Lindenmuth WW, May CJ, Ramsby GR. Prophylactic porto-
3. Feu F, Garcı´a-Paga´n JC, Bosch J, Luca A, Tere´s J, Escorcell A, Rodı´s J.
caval anastomosis. A tale of two studies. Medicine 1972;51:27-40.
Relation between portal pressure response to pharmacotherapy and risk of
22. The Italian Multicenter Project for Propranolol in Prevention of Bleeding.
recurrent variceal hemorrhage in patients with cirrhosis. Lancet 1995;346:
Propranolol prevents first gastrointestinal bleeding in non-ascitic cirrhotic
4. Bosch J, Garcı´a-Paga´n JC, Feu F, Luca A. New approaches in the pharma-
23. Vorobioff J, Picabea E, Villavicencio R, Puccini V, Rossi O, Bordato J,
cologic treatment of portal hypertension. J Hepatol 1993;17(Suppl 2):
Audano M. Acute and chronic hemodynamic effects of propranolol in
unselected cirrhotic patients. HEPATOLOGY 1987;7:648-653.
5. Okumura H, Arakami T, Katsuta Y, Satomura K, Akaike M, Sekiyama T,
24. Gerbes A, Remien J, Jungst D, Sauerbruch T, Paumgartner G. Evidence
Terada H, et al. Reduction in hepatic venous pressure gradient as a conse-
for down-regulation of beta-2-adrenoceptors in cirrhotic patients with se-
quence of volume contraction due to chronic administration of spirono-
vere ascites. Lancet 1986;1:1409-1411.
lactone in patients with cirrhosis and no ascites. Am J Gastroenterol 1991;
25. Escorsell A, Ferayorni L, Bosch J, Garcia-Pagan JC, Garcia-Tsao G, Grace
ND, Rodes J, et al. The portal pressure response to beta blockade is greater
6. Garcı´a-Paga´n J, Salmeron J, Feu F, Gines P, Pizcueta P, Claria J, Arroyo V,
in cirrhotic patients without varices than in those with varices. Gastroen-
et al. Effects of low-sodium diet and spironolactone on portal pressure in
patients with compensated cirrhosis. HEPATOLOGY 1994;19:1095-1099.
26. Angelico M, Carli L, Piat C, Gentile S, Capocaccia L. Effects of isosorbide-
7. Garcı´a-Paga´n J, Salmeron J, Feu F, Gines P, Pizcueta P, Claria J, Arroyo V,
5-mononitrate compared with propranolol on first bleeding and long-term
et al. Plasma volume reduction by spironolactone decreases portal pressure
survival in cirrhosis. Gastroenterology 1997;113:1632-1639.
in patients with compensated cirrhosis. Synergistic effect with propranolol
27. Merkel C, Marin R. Sacerdoti D, Donada C, Cavallarin G, Torboli P,
Amodio P, et al. Long-term results of a clinical trial of nadolol with or
8. Sugano S, Kawafune T, Okajima T, Ishii K, Watanabe M, Takamura N.
without isosorbide mononitrate for primary prophylaxis of variceal bleed-
Chronic splanchnic hemodynamic effects of spironolactone with unre-
ing in cirrhosis. HEPATOLOGY 2000;31:324-329.
stricted sodium diet in patients with compensated cirrhosis. Dig Dis Sci
28. Gines P. Uncomplicated ascites. International Ascites Club. Consensus
Document. 5th Meeting. Dallas, TX: AASLD, 1999.
STAT5602 ___________________________________________________________________________ Two - Way Contingency Tables Joint , Marginal and Conditional Distributions Consider X and Y two categorical response variables, with X having I levels and Y having J levels and suppose we classify each item in a population using both of these variables. Responses ( X , Y ) corresponding to
Confédération Générale du Travail FORCE OUVRIERE au Comité Central Hygiène et Sécurité Monsieur le Ministre Mesdames, Messieurs La FNEC FP FO vous a saisi à deux reprises sur le sujet qui nous intéresse aujourd’hui. Nous attendons de cette réunion qu’elle réponde à nos interrogations et donc à celles des personnels. Tout d’abord, la FNEC FP FO entend rappeler son a
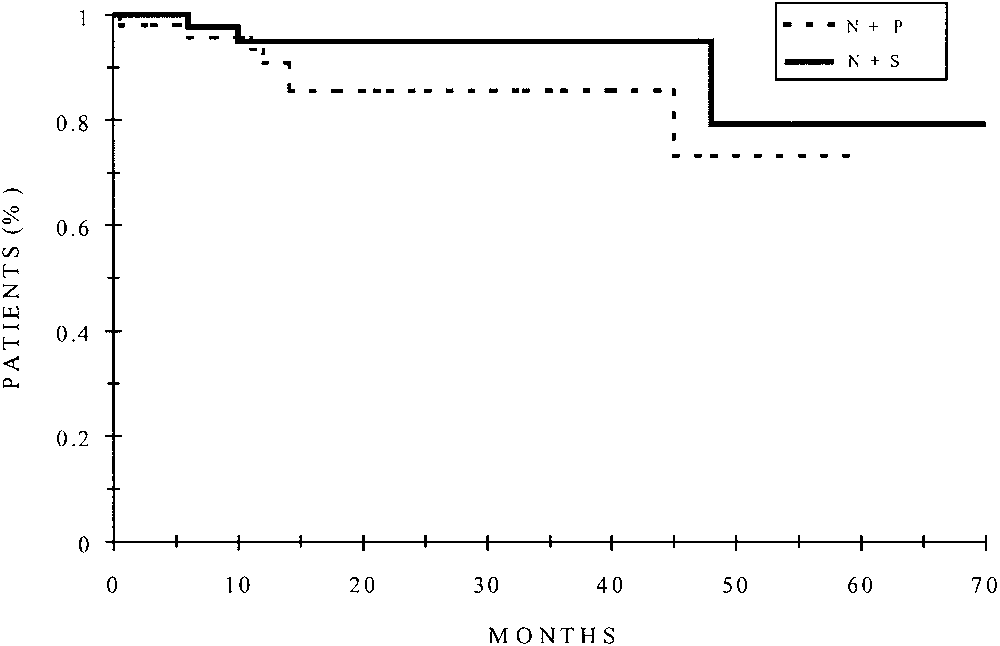
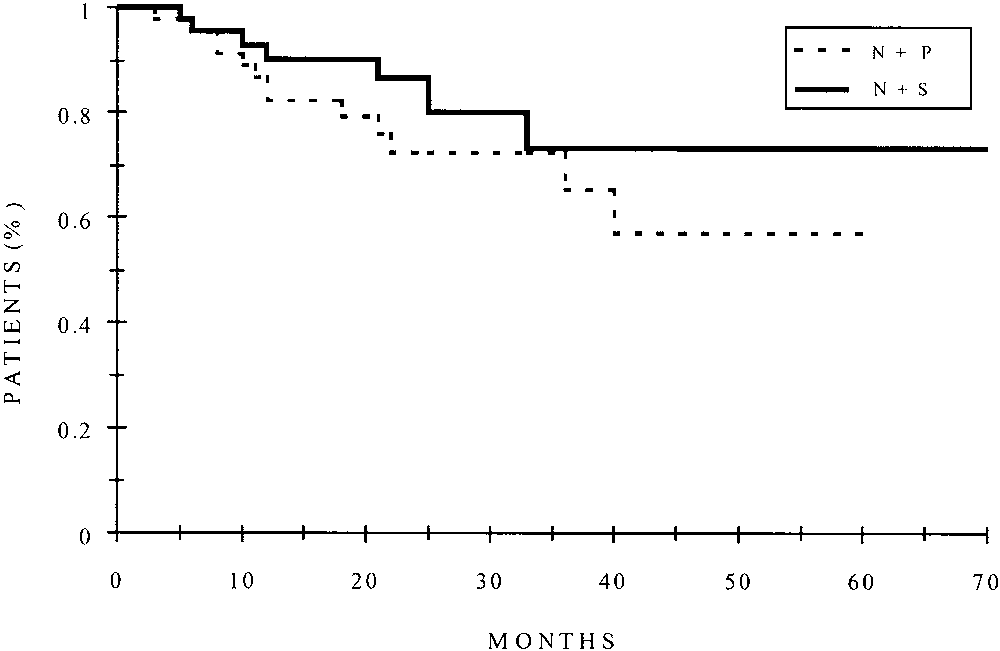 Table 4. Hemodynamic Effects of Nadolol or Nadolol Plus Spironolactone
Table 4. Hemodynamic Effects of Nadolol or Nadolol Plus Spironolactone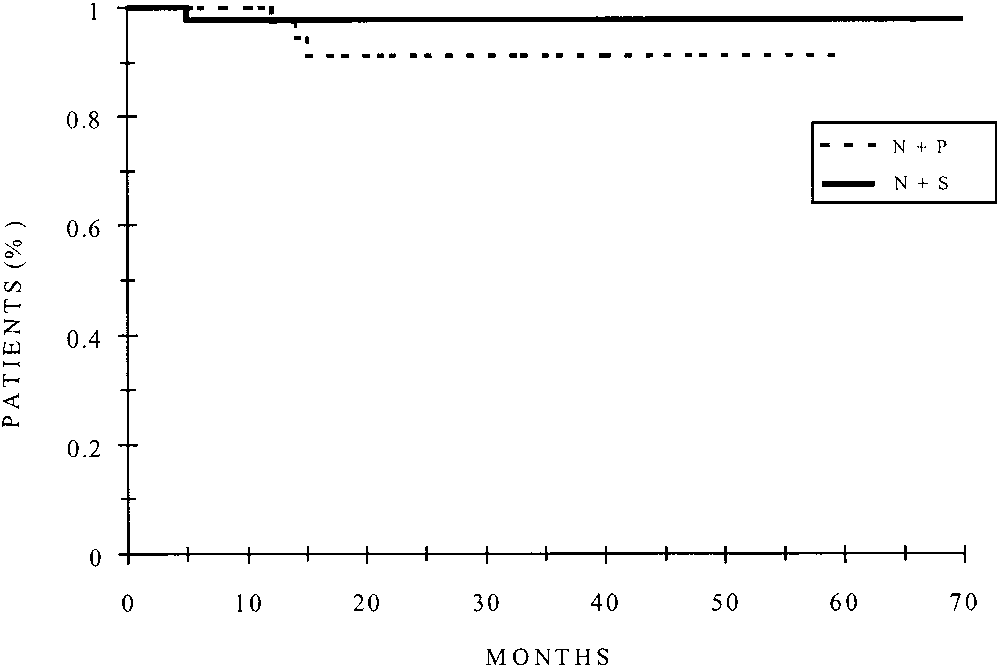 of plasma volume. However, it has also been shown thatspironolactone decreases portal and variceal pressures inpatients following a normal-sodium diet.5,9 Therefore, webelieve it is unlikely that intake of sodium plays a majorrole in our results.
of plasma volume. However, it has also been shown thatspironolactone decreases portal and variceal pressures inpatients following a normal-sodium diet.5,9 Therefore, webelieve it is unlikely that intake of sodium plays a majorrole in our results.