Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
Microsoft powerpoint - treatment of rem behavior disorder with acetylcholinesterase inhibitors - poster.ppt [compatibility mode
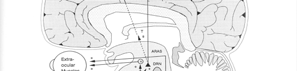
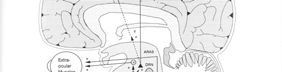
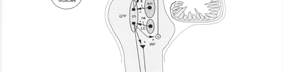
Treatment of REM Behavior Disorder with Acetylcholinesterase Inhibitors Jerald H. Simmons, MD (1,2,3) Brainstem regulation and control of REM Introduction: The author previously reported 3 cases of REM sleep behavior disorder (RBD) that improved by Treatment with acetylcholinesterase inhibitors (Neurology 2000 Sept. 26;55(6):870-1). Now a series of ten cases of RBD are presented that were similarly treated with acetylcholinesterase inhibitors and all of whom also demonstrated improvement in parasomnias. It has become clear that treatment of RBD with acetylcholinesterase inhibitors is a logical and effective treatment appraoch that can be utilized without the side effect profile of more customary approaches with benzodiazepines. pedunculopontine nucleus (acetylcholine) Methods : Patients ranged from 48 to 70 yrs old with an average age of 63.9 (5F / 5M). dorsal raphe nuclei (serotonin)
Treatment was with the acetylcholinesterase inhibitors donepezil (Aricept) or rivastigmine (Excelon),
typically used in the treatment of Alzheimer’s disease. Patients that were also found to have OSA
locus coeruleus
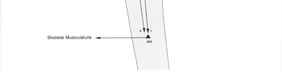
2. descending -skeletal muscle inhibition
(norepinepherine)
or PLMS were included in this study if they continued to exhibit REM parasomnias after Tx of the
OSA and PLMS. Duration of Tx at the time of this assessment ranged from 4 to 18 months, ave
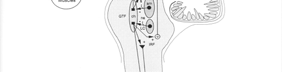
reticulo spinal tract
of 11.5 months. Responses to treatment were based on clinical follow-up, primarily from bed
(glycine)
send impulses down to the spinal cordCausing post synaptic inhibitionof the anterior horn cells by release of glycine
Results : All of the patients placed on acetylcholinesterase inhibitors demonstrated a significant improvement in the magnitude of parasomnic events and/or frequency of observed events. REM Behavior Disorder
Events in all patients reduced from almost nightly elaborate parasomnias down to subtle movements that were not deemed disturbing, and not on a nightly basis, with only occasional more elaborate breakthrough events. Dosages of medications were as high as 20 mg for donepezil, and if side effects, such as diarrhea developed, then they were switched to rivastigmine and dosages went as high as 6 mg qhs (not bid). Of note many patients with RBD
Corticospinal tract
who were also found to have OSA and / or PLMS demonstrated drastic improvement in their
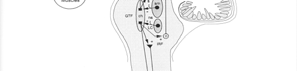
Phasic activity of REM is not inhibited by a dysfunctional
parasomnias by treatment of the OSA / PLMS alone and were not included in this study
peduculopontine nucleus
because further treatment was not necessary. Clonazepam was not initiated in any of our patients, but two came to our center already on clonazepam with persistent REM events. These patietents were still domonstrating REM parasomnias is spite of Clonazepam usage, but
pedunculopontine nucleus
Clonazapam was not withdrawn in these patients. They also demonstrated improvement with
(acetylcholine)
the addition of the acetylcholinesterase inhibitors.
In RBD patients is dysfunctional and does not produce the normal cholinergic activation to the reticulo-spinal tract
reticulo spinal tract Conclusion : This study provides additional evidence that RBD can be treated by (glycine)
enhancing cholinergic neurotransmission. There is considerable evidence that neurons
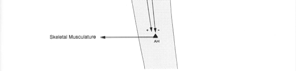
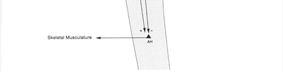
cortico-spinal tract activity descending to the anterior
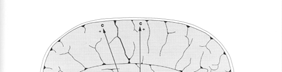
located in the pedunculopontine nuclei play a major role in producing REM sleep and the
related atonia of REM sleep. This region sends descending impulses to activate reticulospinal
tract nucleus. The reticulo-spinal tract nucleus sends impulses down the spinal cord to the anterior horn motor neurons releasing glycine that causes post synaptic inhibition of motor
REM Atonia reestablished in REM Behavior Disorder
neurons. Acetylcholinesterase inhibitors work by enhancing the cholinergic activity of the peduculopontine nucleus to restore the failing network during REM that leads to return of the post synaptic inhibition of the anterior horn cells. GABA neurons also play a role in the muscle atonia of REM, possibly by an interneuronal activity that is involved in this same system leading to post synaptic inhibition of the anterior horn cells. However, treatment to enhance this pathway with clonazepam is frequently accompanied by sedating side effects as well as all of the other long term negative effects on sleep associated with clonazepam. Therefore, it would be
Corticospinal tract
reasonable to consider the use of acetylcholinesterase inhibitors as a first line treatment in
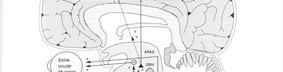
Acetylcholinesterase inhibitors enhances the acetylchone
patients with RBD and then switching to clonazepam if adequate clinical response is not
activity of the peduculopontine nucleus during REM to restore the descending inhibitory pathway that provides muscle pedunculopontine nucleus paralysis of REM sleep. (acetylcholine) Authors Affiliations: 1. Sadler Clinic Sleep Disorders Center , The Woodlands, TX, USA. 2. Comprehensive Sleep Medicine Associates , Houston, TX, USA. 3. Sleep Education Consortium, Inc, Houston, TX, USA. reticulo spinal tract (glycine)
HAMS Position Statement on Psychiatric Medications 1) HAMS recognizes that psychiatric medications can be great lifesavers for many people and we encourage people who are benefitting from psychiatric medications to continue taking them; we also encourage people who may benefit from them to consult with their doctor about giving them a try. 2) HAMS also recognizes that psychiatric medicati
Þizofrenide Klasik Antipsikotiklerle Prof. Dr. Seher SOFUOÐLU* 1. KONVANSÝYONEL ANTÝPSÝKOTÝK Klorpromazinin bir antipsikotik ajan olduðu ÝLAÇLARIN KEÞFÝ keþfedildikten sonra onun aksiyon mekanizmasýnýÝlk antipsikotik (AP) ilaç 1950'lerde rastlantý anlamak üzere eksperimental araþtýrmalarsonucu keþfedilmiþ olan ve antihistaminikyapýlýrken hayvanlarda "neu


 Treatment of REM Behavior Disorder with Acetylcholinesterase Inhibitors
Treatment of REM Behavior Disorder with Acetylcholinesterase Inhibitors