Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
Gomes et al., 2010 adm rhcg
L. Mramba et al. / International Journal of Gynecology and Obstetrics 108 (2010) 152–160
procedure and the injury was repaired shortly after the incarceration. In the first case the patient underwent hysteroscopy and laparoscopy5 years after the surgical termination [3].
When uterine perforation is suspected based on an abnormal
finding in the retrieved material, although rare, tubal incarcerationmust be considered—especially because it can be relatively asymp-tomatic. Prompt diagnosis may lead to preservation of the incarcer-ated tube.
No conflicts of interest to declare.
[1] Hakim-Elahi E, Tovell HM, Burnhill MS. Complications of first-trimester abortion: a
report of 170, 000 cases. Obstet Gynecol 1990;76(1):129–35.
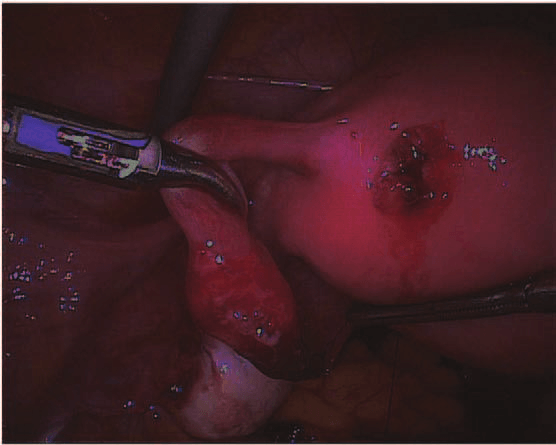
Fig. 3. Laparoscopic view of the fallopian tube extracted from the uterine wall lesion.
[2] Kaali SG, Szigetvari IA, Bartfai GS. The frequency and management of uterine
perforations during first-trimester abortions. Am J Obstet Gynecol 1989;161(2):406–8.
[3] Deffieux X, Kane A, Faivre E, Gervaise A, Frydman R, Fernandez H. Intrauterine
fallopian tube incarceration: an uncommon complication of termination of
suggested by the presence of a portion of the fallopian tube in the
pregnancy by vacuum aspiration. Fertil Steril 2008;90(5):1938–9.
material removed at the second vacuum aspiration.
This is the second reported case of fallopian tube incarceration, but
the first in which the complication was suspected at the time of the
0020-7292/$ – see front matter 2009 International Federation of Gynecology and Obstetrics. Published by Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.ijgo.2009.08.028
Administration of a pharmacophysiologic dose of recombinant human chorionicgonadotropin at menses promotes corpus luteum rescue
Claudia M. Gomes a,b, Paulo C. Serafini a,b,⁎, Eduardo L.A. Motta b,c, Andre M. Rocha b,Isaac M. Yadid d, Edmund C. Baracat a
a Center for Human Reproduction, Discipline of Gynecology, University of São Paulo Medical School, São Paulo, Brazilb Huntington Reproductive Medicine, São Paulo, Brazilc Department of Gynecology, Federal University of São Paulo Medical School, São Paulo, Brazild Huntington Reproductive Medicine, Rio de Janeiro, Brazil
fertilization (IVF), when rhCG was administered on the first day ofmenses in an effort to reduce the recruitment of a secondary follicle
cohort [2]. This tactic is aimed at increasing the pregnancy rate and
reducing the risk of ovarian hyperstimulation syndrome; however,
Received in revised form 1 September 2009Accepted 5 October 2009
rescuing a prior corpus luteum, which may result in the prematureelevation of progesterone levels during ovulation induction, could be
detrimental to IVF outcome by reducing endometrial receptivity and
interfering with follicle development [3]. Thus, the present study aimed
to evaluate whether rhCG administration on the first day of menses
promoted corpus luteum rescue and to determine the frequency of suchrescue.
Thirty women—all of whom signed approved Institutional Review
Recombinant human chorionic gonadotropin (rhCG) can be admin-
Board consent forms—were included in the present retrospective
istered during the late follicular phase of ovulation induction to promote
analysis. On their first day of full-flow menstruation, women undergo-
selection and growth of the most competent follicle cohort [1]. An
ing ovulation induction with a gonadotropin-releasing hormone
elevated pregnancy rate was observed recently, following in vitro
(GnRH) antagonist protocol were administered rhCG (250 mg; Ovidrel,Merck-Serono, Brazil). Serum levels of estradiol, progesterone, follicle-stimulating hormone (FSH), and luteinizing hormone (LH) weremeasured for all participants on their first and third menstrual days(D1 and D3, respectively). Rescued corpus luteum (rCL) was defined as a
⁎ Corresponding author. Avenida República do Líbano 529, São Paulo 04501-000,
serum progesterone level of 2 ng/mL or more on D3. Frequencies of rCL
E-mail address: pserafini@huntington.com.br (P.C. Serafini).
and non-rCL were compared via 2-proportion z tests, and differences
L. Mramba et al. / International Journal of Gynecology and Obstetrics 108 (2010) 152
Serum levels of FSH and LH did not differ significantly between the
Hormone levels on D1 and D3 in the rCL and non-rCL groups following administration
Rescued corpus luteum was observed in a surprisingly large
proportion—approximately two-thirds—of women undergoing ovu-lation induction with a GnRH antagonist who received a single
pharmacophysiologic dose of rhCG on D1. Although rCL was not a
universal feature among women who were administered rhCG on D1,
efforts to limit its occurrence should be made to prevent the possible
harmful effects on IVF outcome of a premature increase in progesterone
Abbreviations: D1, first menstrual day; D3, third menstrual day; E2, estradiol; FSH,
follicle-stimulating hormone; LH, luteinizing hormone; P, progesterone; rCL, rescuedcorpus luteum; rhCG, recombinant human chorionic gonadotropin.
The authors have no conflicts of interest.
a Values are given as mean± standard error unless otherwise indicated.
between the rCL and the non-rCL groups were analyzed, as appropriate,
[1] Filicori M, Fazleabas AT, Huhtaniemi I, Licht P, Rao ChV, Tesarik J, et al. Novel
with t tests or Mann-Whitney U tests. P < 0.05 was considered
concepts of human chorionic gonadotropin: reproductive system interactions and
potential in the management of infertility. Fertil Steril 2005;84(2):275–84.
Two women were excluded from the analysis because of corpus
[2] Motta EL, Smith GD, Serafini PC, Coslovsky M, Hassun P, Rocha AM, et al. Human
choriogonadotropin prior to controlled ovarian stimulation and in vitro fertilization
luteum persistence—as defined by serum progesterone levels of 2 ng/
improves implantation, and pregnancy rates. J Assist Reprod Genet 2009;26
mL or more on D1—before receiving rhCG. Rescued corpus luteum
occurred in 19 (67.9%) of the remaining 28 participants, with the
[3] Kolibianakis EM, Zikopoulos K, Smitz J, Camus M, Tournaye H, Van Steirteghem AC,
et al. Elevated progesterone at initiation of stimulation is associated with a lower
fied as having non-rCL. Serum progesterone and
ongoing pregnancy rate after IVF using GnRH antagonists. Hum Reprod 2004;19
estradiol levels following rhCG administration were significantly
greater in the rCL group than in the non-rCL group (P < 0.01; Table 1).
0020-7292/$ – see front matter 2009 International Federation of Gynecology and Obstetrics. Published by Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.ijgo.2009.09.015
Failure of cabergoline to prevent severe ovarian hyperstimulation syndrome inpatients with extremely high estradiol levels
Jiann-Loung Hwang a,b,c,⁎, Yu-Hung Lin a,c,d,⁎, Kok-Min Seow a,da Department of Obstetrics and Gynecology, Shin Kong Wu Ho-Su Memorial Hospital, Taipei Medical University, Taipei, Taiwanb School of Medicine, Taipei Medical University, Taipei, Taiwanc Department of Obstetrics and Gynecology, National Taiwan University Hospital, Taiwand School of Medicine, Fu Jen Catholic University, Taiwan
strategies to prevent OHSS, coasting—withholding gonadotropins anddelaying administration of human chorionic gonadotropin (hCG)—is
the most popular [1]. Although the pathophysiology is not fully
understood, vascular endothelial growth factor (VEGF) has been
Received in revised form 10 September 2009Accepted 14 October 2009
proposed to be the key mediator [2]. Several studies have shown thatcabergoline, which antagonizes VEGF effect on vascular permeability,
effectively prevented OHSS [2–4]. We report two patients at high risk
for OHSS who developed the complication despite undergoing
combined treatment with coasting and cabergoline.
A 29-year-old woman underwent in vitro fertilization for tubal factor
infertility. After pituitary suppression with 0.5 mg per day of buserelin(Supremon; Hoechst, Frankfurt, Germany) from day 21 of her previouscycle, the patient was stimulated for 7 days with recombinant follicle-
Ovarian hyperstimulatilon syndrome (OHSS) is a life-threatening
stimulating hormone (Gonal-f; Serono, Aubonne, Switzerland) follow-
complication associated with ovarian stimulation. Among the several
ing a dosage regimen of 150 IU for 4 days, 112.5 IU for 2 days, and 75 IUfor 1 day. Coasting was initiated to avoid OHSS. Over the 3 days ofcoasting, serum estradiol levels were 4568 pg/mL, 6555 pg/mL, and
⁎ Corresponding authors. Department of Obstetrics and Gynecology, Shin-Kong Wu
9713 pg/mL, respectively, and 13042 pg/mL on the day of hCG
Ho-Su Memorial Hospital, No. 95, Wen Chang Road, Shih Lin District, Taipei, Taiwan.
administration. The patient received 5000 IU of hCG (Pregnyl; Organon,
Tel.: +886 2 28332211x3879; fax: +886 2 28389416.
E-mail address: M002179@ms.skh.org.tw (Y.-H. Lin).
Roseland, USA) and oocyte retrieval was performed 36 hours later.
MARCH 11, 2008 MINUTES OF THE BEAVER CITY COUNCIL:The Beaver City Council met in regular session on the 11 daycommenced at 4:00 p.m. The following Council Members were present: Mayor Leonard Foster,City Council Members; Kari Draper, Connie Fails, Craig Wright, Gordon Roberts and Chris Smith. Also, present at the meeting: City Recorder Hal Lessing and City Manager Steve Atkin. Mayor Foster conduc
Journal of Advanced Pharmaceutical Sciences Prasad Neerati et. al 2011 Vol-1 Issue 1 INFLUENCE OF ITRACONAZOLE A P-GLYCOPROTEIN PRASAD NEERATI, * MURALIKRISHNA GADE. DMPK & Clinical Pharmacology Division Department of Pharmacology, University College of Pharmaceutical Sciences, Kakatiya University, Warangal, India-506 009. The present study was aimed at i
 L. Mramba et al. / International Journal of Gynecology and Obstetrics 108 (2010) 152–160
procedure and the injury was repaired shortly after the incarceration.
L. Mramba et al. / International Journal of Gynecology and Obstetrics 108 (2010) 152–160
procedure and the injury was repaired shortly after the incarceration.