Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
Spliceosomal peptide p140 for immunotherapy of systemic lupus erythematosus: results of an early phase ii clinical trial
Vol. 58, No. 12, December 2008, pp 3873–3883
2008, American College of Rheumatology
Spliceosomal Peptide P140 for Immunotherapy of
Results of an Early Phase II Clinical Trial
Sylviane Muller,1 Fanny Monneaux,1 Nicolas Schall,1 Rasho K. Rashkov,2
Boycho A. Oparanov,3 Philippe Wiesel,4 Jean-Marie Geiger,5 and Robert Zimmer5
Objective. To assess the safety, tolerability, and double-stranded DNA (anti-dsDNA), chromatin, cardi- efficacy of spliceosomal peptide P140 (IPP-201101; se- olipin, and peptides of the U1-70K protein, was tested by quence 131–151 of the U1-70K protein phosphorylated enzyme-linked immunosorbent assay (ELISA). The at Ser140), which is recognized by lupus CD4؉ T cells, in plasma levels of C-reactive protein, total Ig, IgG, IgG the treatment of patients with systemic lupus erythem- subclasses, IgM, IgA, and IgE, and of the cytokines atosus (SLE). interleukin-2 and tumor necrosis factor ␣ were mea- Methods. An open-label, dose-escalation phase II sured by ELISA and nephelometry. study was conducted in two centers in Bulgaria. Twenty Results. IgG anti-dsDNA antibody levels de- patients (2 male and 18 female) with moderately active creased by at least 20% in 7 of 10 patients who received SLE received 3 subcutaneous (SC) administrations of a 3 ؋ 200 g IPP-201101 (group 1), but only in 1 patient clinical batch of P140 peptide at 2-week intervals. in the group receiving 3 ؋ 1,000 g IPP-201101 (group Clinical evaluation was performed using approved 2). Physician’s global assessment of disease activity scales. A panel of autoantibodies, including antinuclear scores and scores on the SLE Disease Activity Index antibodies, antibodies to extractable nuclear antigens were significantly decreased in group 1. The changes (U1 RNP, SmD1, Ro/SSA, La/SSB), and antibodies to occurred progressively in the population of responders, increased in magnitude during the treatment period,
Clinical trial approval no. 143/14.06.2006 (Bulgaria). and were sustained. No clinical or biologic adverse
Supported by ImmuPharma France, an affiliate of Immu-
effects were observed in the individuals, except for some
Pharma PLC, as part of a full clinical development program. local irritation at the highest concentration.
Sylviane Muller, PhD, Fanny Monneaux, PhD, Nicolas
Schall, BSc: CNRS, Institut de Biologie Mole
Conclusion. IPP-201101 was found to be safe and
Strasbourg, France; 2Rasho K. Rashkov, MD: Medical University
well tolerated by subjects. Three SC doses of IPP-201101
Sofia, Sofia, Bulgaria; 3Boycho A. Oparanov, MD: Medical Military
Academy, Sofia, Bulgaria; 4Philippe Wiesel, MD: Genexion SA,
g significantly improved the clinical and bio-
Geneva, Switzerland; 5Jean-Marie Geiger, MD, PharmD, Robert
logic status of lupus patients.
Zimmer, MD, PhD: ImmuPharma France SA, Mulhouse, France.
Dr. Muller has received consulting fees, speaking fees, and/or
Systemic lupus erythematosus (SLE) is a chronic
honoraria from ImmuPharma (less than $10,000); she owns stock orstock options in ImmuPharma PLC and is coinventor of P140 peptide.
inflammatory disease of multifactorial etiology. It is a
Dr. Wiesel is Managing Director of Genexion SA; he owns stock or
prototypic autoimmune disease characterized by in-
stock options in Genexion SA. Dr. Geiger is Vice President of clinical
creased production of autoantibodies, immune complex
development with ImmuPharma; he owns stock or stock options inImmuPharma PLC. Dr. Zimmer is President and Chief Scientific
deposition in the microvasculature, leukocyte infiltra-
Officer of ImmuPharma PLC; he owns stock or stock options in
tion, and, finally, progressive tissue damage in certain
organs (1). The clinical course of the disease is episodic
Address correspondence and reprint requests to Sylviane
with unpredictable periods of activity flares. Current treat-
Centre National de la Recherche Scientifique, 15 Rue Rene
ments of the disease are mainly based on immunosup-
67000 Strasbourg, France. E-mail: S.Muller@ibmc.u-strasbg.fr.
pressive drugs such as corticosteroids and cyclophospha-
Submitted for publication May 13, 2008; accepted in revised
mide, which are often administered at high doses in
acute exacerbation phases (1–3). Although these treat-
(10) and reorient, at least transiently, the deleterious
ments have significantly reduced mortality and length-
autoimmune response by a mechanism that remains to
ened patients’ life expectancies, they have important side
effects, particularly when they are applied for long-term
The recognition of P140 or peptide 131–151 by T
management of disease. Adverse effects such as obesity,
cells from patients with other autoimmune diseases
diabetes mellitus, hyperlipidemia, and hypertension are
reversible and generally improve after reducing the
myositis, primary biliary cirrhosis, autoimmune hepati-
corticoid dosage. These drugs may also contribute to late
tis) could not be demonstrated (8). No increase in IL-10
irreversible complications such as bone marrow depres-
was observed. Further, it was demonstrated that P140-
sion, ovarian failure, or enhanced risk of bladder cancer.
treated and untreated lupus mice behaved similarly
To avoid such important side effects, we focus our efforts
when infected by a flu virus (9). This indicates that the
on the development of alternative therapeutic strategies,
tolerogenic effect of P140 peptide was limited to certain
which are specific, targeted, and less toxic.
autoreactive T cell clones and that the overall immune
An epitope has been identified that is present in
system was maintained unaffected. The present study
residues 131–151 of the 70K spliceosomal protein within
was designed to examine the safety, tolerability, and
the U1 small nuclear RNP (the U1-70K spliceosomal
efficacy of peptide P140 (IPP-201101) in lupus patients.
protein) and that is recognized very early by IgG anti-bodies and CD4ϩ lymph node (LN) T cells from bothH-2k MRL/lpr and H-2d/z (NZB ϫ NZW)F lupus-prone
PATIENTS AND METHODS
mice (4,5). It was shown further that an analog of this
Study design. This phase II study was an open-label,
sequence, phosphorylated on Ser140 (named peptide
dose-escalation, add-on study in two centers in Bulgaria in-
P140), was also recognized by LN and peripheral CD4ϩ
cluding 20 patients with moderately active SLE who received 3
T cells as well as by IgG antibodies from MRL/lpr mice
subcutaneous (SC) administrations of IPP-201101 2 weeks
(6,7). In a therapeutic protocol in which peptides were
apart. In addition to standard care, patients received 3 ϫ 200
g of IPP-201101 (group 1) or 3 ϫ 1,000 g of IPP-201101
administered intravenously (IV) in saline (three injec-
(group 2). The primary objective was to evaluate the effect of
tions at 2-week intervals and a fourth injection 1 month
treatment on anti-dsDNA antibodies in the plasma of lupus
later), the P140 peptide, but not the cognate nonphos-
patients. In this initial phase II study, a positive response was
phorylated peptide 131–151, significantly reduced pro-
defined as a decrease in levels of anti-dsDNA antibodies by
teinuria and anti–double-stranded DNA (anti-dsDNA)
20% compared with the respective baseline level in eachpatient enrolled in the study. Secondary objectives were to
IgG antibody levels, delayed mortality, and enhanced
ascertain the effectiveness of IPP-201101 on other biologic
the survival rate of treated MRL/lpr mice (6). Unit
parameters as well as on the clinical signs of lupus patients as
peptide doses of 100 g and 50 g were effective,
determined by the SLE Disease Activity Index (SLEDAI) (11).
whereas the effectiveness of the 25-g dose was similar
The physician’s global assessment of disease activity was also
to that of saline (Monneaux F, Muller S: unpublished
recorded using a 100-mm visual analog scale. Values areexpressed in length (0–25 mm ϭ no active disease, Ͼ25–50
mm ϭ mild disease, Ͼ50–75 mm ϭ moderate disease, Ͼ75–
Peptide 131–151, the sequence of which is com-
100 mm ϭ severe disease). Detailed informed consent was
pletely conserved in mice and humans, was able to
obtained from all patients in accordance with the Declaration
induce ex vivo the proliferation of CD4ϩ T cells from
of Helsinki, the International Conference of Harmonization
lupus patients (8). Interestingly, however, when lupus
guideline for Good Clinical Practice, and application of localregulations.
patients’ peripheral CD4ϩ T cells were incubated in the
Patients. Male and female subjects (age 18–70 years)
presence of the P140 analog, the phosphorylation of
with an established diagnosis of SLE according to American
Ser140 prevented the proliferation while favoring the
College of Rheumatology (ACR) classification criteria (12)
secretion of high levels of interleukin-10 (IL-10).
and with elevated titers of anti-dsDNA antibodies (Ͼ50 IU/ml
Although the precise mode of action of P140
at screening visit) were eligible. If subjects were receiving oralcorticosteroids, the daily dose could not exceed 10 mg of
peptide is not fully understood, repeated administration
prednisolone or equivalent, the start date had to be at least 3
of P140 peptide in saline into preautoimmune MRL/lpr
months prior to the start of study treatment, and the daily dose
mice transiently abolishes both T cell intramolecular
had to be stable during the 4 weeks preceding the start of study
spreading to other regions of the U1-70K protein (7)
treatment. If subjects were receiving antimalarials, methotrex-
and T cell intermolecular spreading to regions of other
ate, or azathioprine, the start date had to be at least 3 monthsprior to the start of study treatment, and the daily dose had to
spliceosomal proteins such as SmD1 (9). These impor-
be stable during the 4 weeks preceding the start of study
tant observations suggest that the P140 analog might
initiate a mechanism of so-called tolerance spreading
Patients were excluded if they were undergoing a flare
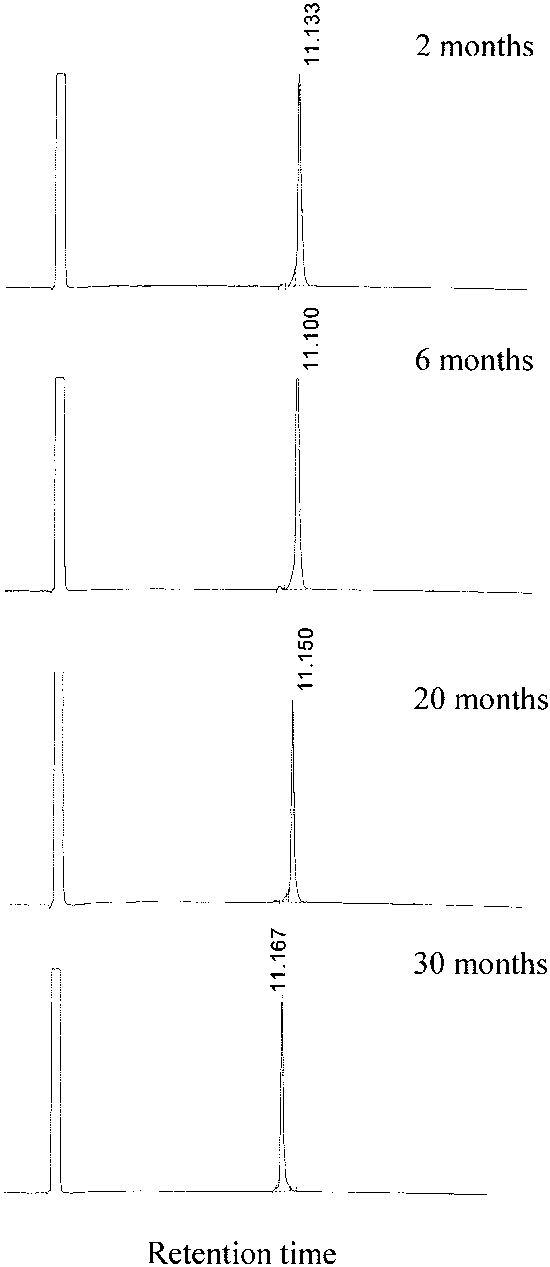
phy on a Beckman Coulter (Roissy, France) instrument. Thelinear gradient was from 5% to 65% solvent B (acetonitrile/0.08% trifluoroacetic acid). Data have shown that the shelf lifeof the product is at least 30 months (Figure 1). Prior toadministration to patients, a subchronic toxicity study wasconducted in rats and dogs under standard Good LaboratoryPractice conditions. No adverse reactions were recorded, andthe no observable effects limit level was set at Ͼ1 mg/kg bodyweight. Segment 2 studies were also performed in rats andrabbits. No deleterious events were recorded. The total expo-sure during this study was equivalent to 130 years of the an-ticipated human therapeutic exposure on a body weight basis. Measurements. Patients were assessed for adverse
effects. The complete blood cell counts were checked, as werechemistry parameters (blood/urine), blood pressure, heartrate, body temperature, and electrocardiographic parameters. The same laboratory carried out the serologic measurementsperformed with the samples obtained from patients in groups1 and 2. Anti-dsDNA antibodies were determined by enzyme-linked immunosorbent assay (ELISA) (Varelisa and EliA;Pharmacia, Uppsala, Sweden). The total levels of Ig as well asthe individual levels of IgG, IgG subclasses (from IgG1 toIgG4), and IgE were measured by ELISA. A nephelometricmethod was also used to measure IgG, IgM, and IgA levels(MININEPH Human IgG, IgM, IgA kits; The Binding Site,Birmingham, UK). The serum samples were tested by ELISAfor antinuclear antibodies (ANAs) (ReCombi ANA Screen
Characteristics of the SLE patients at baseline*
Figure 1. Shelf life of P140 peptide. Each batch of P140 peptide was
stored lyophilized at Ϫ20°C in glass tubes. Peptide integrity was
checked by analytic reverse-phase high-performance liquid chromatog-
raphy on a Beckman Coulter instrument using a Nucleosil C18 5-m
column (150 ϫ 4.6 mm). Linear gradients detected at 215 nm were
5–65% solvent B (acetonitrile/0.08% trifluoroacetic acid). Retention
of disease activity (SLEDAI score Ͼ15) requiring treatment
with immunosuppressive drugs, as were patients with severe
central nervous system, hematologic, cardiac, or renal mani-
festations of SLE, patients with cytopenia with hemoglobin
Ͻ7.5 gm/dl, white blood cell (WBC) count Ͻ2,000/ml, and/or
platelet count Ͻ50,000/ml, and patients undergoing hemodia-
lysis. We also excluded patients who were previously being treated
with immunosuppressives (cyclophosphamide, mycophenolate
mofetil, rituximab, or any other immunosuppressive drug)
within 4 months of the start of study treatment as well as
patients with any concomitant medical condition which, in the
opinion of the investigator, might have interfered with the
safety or with the evaluation of the study. Investigational drug. The peptide IPP-201101 was
synthesized by NeoMPS (Strasbourg, France) and manufac-
tured by Innotech Labor (Basel, Switzerland), all in compli-ance with current Good Manufacturing Practice conditions. It
* Except where indicated otherwise, values are the number of patients. SLE ϭ systemic lupus erythematosus; BMI ϭ body mass index;
is soluble in water (Ͼ25 gm/liter), 5% (weight/volume) sucrose
ANAs ϭ antinuclear antibodies; SLEDAI ϭ SLE Disease Activity
(12 gm/liter), and saline (between 0.5 gm/liter and 1 gm/liter).
Index; MP ϭ methylprednisolone; AZA ϭ azathioprine; HCQ ϭ
Several stability studies have been performed with different
batches of P140 peptide. Peptide integrity was checked by
† Patients in group 1 received 3 ϫ 200 g IPP-201101. Patients in
analytic reverse-phase high-performance liquid chromatogra-
group 2 received 3 ϫ 1,000 g IPP-201101.
Evolution of anti-dsDNA antibody levels during the study period*
* Values in parentheses are the mean of differences, expressed as percent change versus day 1. In the group receiving 200 g IPP-201101, there were7 patients with a Ն20% decrease of anti–double-stranded DNA (anti-dsDNA) antibody levels on day 43 (patients 2–6, 9, and 10), termed responders. In the group receiving 1,000 g IPP-201101, there was 1 responder (patient 15). † P ϭ 0.1823 versus day 1. ‡ P ϭ 0.0006 versus day 1. § P ϭ 0.0028 versus day 1. ¶ P ϭ 0.0014 versus day 1. # P ϭ 0.0767 versus day 1. ** P ϭ 0.0176 versus day 1.
Varelisa) and for antibodies to U1 RNP, SmD1, Ro/SSA, and
Statistical analysis. Percent reduction in levels of
La/SSB antigens (ReCombi ANA 4-Profile Varelisa). Specific
anti-dsDNA antibodies compared with baseline was computed
ELISAs were used to measure levels of antibody to cardiolipin
by subject and by study day. Student’s t-test was applied to
(antigen ref. C-0563; Sigma, St. Louis, MO), chromatin
detect a positive mean reduction compared with baseline. The
(QUANTA Lite; Inova Diagnostics, San Diego, CA), and
Mann-Whitney nonparametric test was used to evaluate the
peptides of the U1-70K protein (adapted for human sera [6]).
number of responders in the 2 groups of patients. P values less
Plasma levels of C-reactive protein (CRP) were mea-
than 0.05 were considered significant.
sured using a nephelometric method (MININEPH humanC-reactive protein kit). Plasma levels of IL-2 and tumornecrosis factor ␣ (TNF␣) were measured by double-sandwich
ELISA. Standard curves performed with known concentra-tions of cytokines (PharMingen, San Diego, CA) were used for
Patient characteristics. The study population
the test calibration. In the test conditions, the minimal levels of
consisted of 20 white patients (2 male, 18 female) age
detectable cytokines were 8 pg/ml IL-2 and 2 pg/ml TNF␣.
Ͼ18 years (mean Ϯ SD 34.8 Ϯ 10.0 years, median 33.5
of at least 20% in anti-dsDNA antibody levels (Table 2)compared with only 1 of 10 patients in group 2 (P Ͻ0.03). Other immunologic parameters. During the ob-
servation period, total Ig (IgM, IgG, and IgA) and IgGlevels slowly decreased in all group 1 patients except inpatient 1, in whom the total Ig and IgG levels remainedstable (not shown). A similar kinetic was observed whenIgG1 levels were measured in the consecutive serumsamples. In some patients, the level of Ig increased againafter the last administration on day 43 and/or day 57. Good positive correlations (R2 ϭ 0.752, 0.733, 0.685,and 0.579) between the levels of IgG and anti-dsDNA
Figure 2. Evolution of anti–double-stranded DNA (anti-dsDNA) anti-
antibody were observed in 4 patients (patients 2, 3, 6,
body levels during the study period. Administration of IPP-201101 was
and 9, respectively). IgM and IgA levels decreased
on days 1, 15, and 29. The results are expressed as the mean percent
slightly or showed no change during the study period.
reduction with regard to baseline values (horizontal bar at the zerolevel). Error bars are shown.
IgE levels remained very low and largely below the limitof positivity in all samples (not shown).
A panel of typical autoantibodies was measured
years) with a mean Ϯ SD body mass index of 22.8 Ϯ 4.5
in the samples. The levels of ANAs present in all 10
kg/m2 (median 21.3). All patients met the ACR criteria
patients of group 1 did not change significantly during
for the classification of SLE (12) and had moderately
the study period except in patient 3 (Figure 3A). The
active disease as defined by SLEDAI scores between 2
levels of antibodies to U1 RNP and SmD1 present at low
and 14 (Table 1). Duration of IPP-201101 treatment was
levels in 3 patients and 1 patient, respectively, also
4 weeks (SC injections on days 1, 15, and 29), and
remained unchanged (Figures 3B and C). Antibodies to
followup visits were on days 8, 43, and 57. Long-term
Ro (positive in 3 patients) and La (positive in 1 patient)
followup visits were at months 4, 5, and 6. The concom-
also remained at their initial levels during the study
itant treatment received by patients in groups 1 and 2 is
period (Figures 3D and E). Antichromatin IgG antibody
indicated in Table 1. There was no change in doses of
levels, which were high in 6 of 10 patients in group 1,
medication for lupus disease during the study period (57
slightly decreased with time or remained unchanged
(Figure 4A). Anticardiolipin antibody levels were weakly
Anti-dsDNA antibody levels. The efficacy objec-
positive in 3 of 10 patients and showed no significant
tive of this open-label add-on phase II study was to
fluctuation in these patients (Figure 4B). IgG antibodies
examine the relationship between IPP-201101 treatment
to peptide 131–151 and P140 were absent on day 1 in the
and biologic and clinical markers of disease activity.
serum of our entire cohort, and their titers remained
Specifically, the predefined primary efficacy end point
unchanged during the treatment period (not shown).
was a significant reduction in anti-dsDNA antibody
Plasma levels of IL-2 remained below the threshold of
titers. Anti-dsDNA antibody levels, as measured by
detection during the entire study. TNF␣ levels remained
ELISA, decreased during the treatment period in group
ϳ15 pg/ml in all samples and were not different from
1, with a nadir of 112 IU/ml on day 43 (Table 2). When
those measured in normal individuals tested in parallel
expressed as the mean percent reduction from baseline,
the changes in anti-dsDNA antibody levels seen in group
SLEDAI score and physician’s global assessment
1 were time dependent and statistically significant (Ta-
of disease activity score. SLEDAI data were collected
ble 2 and Figure 2). A 24% reduction was observed on
and assessed in order to explore the initial therapeutic
day 43 (P ϭ 0.0014 compared with day 1). Remarkably,
profile of IPP-201101 in SLE patients. In this analysis,
a 17% decrease (P ϭ 0.0006) was already observed after
we discarded data from patient 13 (group 2), who had a
the first administration of IPP-201101. A more limited
low SLEDAI score of 2.0 at entry. Regarding the other
reduction was observed in group 2 (a transient but
patients (SLEDAI scores Ն6), the mean SLEDAI score
statistically significant decrease was observed on day 15
was found to decrease from 7.8 to 4.8 in a progressive
only) (Table 2). Thus, in the course of treatment with the
and sustained manner in the 200 g dose group (group
200 g IPP-201101 dose, 7 of 10 patients had a reduction
1) during the course of the study, while it decreased only
Figure 3. Evolution of levels of antinuclear antibodies (ANAs) (A) and of levels of anti–U1 RNP (B), anti-SmD1 (anti-Sm) (C), anti-Ro/SSA (D), and anti-La/SSB (E) antibodies in the 10 patients of group 1 during the study period. Administration of IPP-201101 was on days 1, 15, and 29; the 3 consecutive samples were obtained from each patient on days 1, 29, and 57 (gray, red, and yellow bars, respectively). An enzyme-linked immunosorbent assay (ELISA) was used to measure levels of ANAs (ReCombi ANA Screen Varelisa) and levels of antibodies to U1 RNP, SmD1, Ro/SSA, and La/SSB antigens (ReCombi ANA 4-Profile Varelisa). The lower horizontal line corresponds to the cutoff value of positivity Ͻ1.0 IU/ml); between the lower and upper horizontal lines are serum sample data with positivity considered equivocal (1.0 Ͻ value Ͻ 1.4) according to the ELISA manufacturer’s recommendations.
slightly from 9.0 to 7.0 in the 1,000 g dose group (group
was observed in group 2 (19%). Similarly, the proportion
2) (Table 3). When expressed as the mean percent
of patients achieving a reduction of at least 4 points in
reduction from baseline, these changes represented a
the SLEDAI score was 60% (6 of 10 patients) and 44%
40% reduction at the end of the observation period
(4 of 9 patients) in the 200 g and 1,000 g IPP-201101
(days 43 and 57) in group 1. In contrast, but in accor-
dose groups, respectively (Table 3).
dance with the data obtained for anti-dsDNA antibody
It is worth noting that 5 of 6 patients in group 1
titers, a more limited improvement in the SLEDAI score
showed both a decrease of anti-dsDNA antibody levels
Figure 4. Evolution of antichromatin (A) and anticardiolipin (B) IgG antibody levels in the 10 patients of group 1 during the study period. Administration of IPP-201101 was on days 1, 15, and 29; the 6 consecutive samples were obtained from each patient on days 1, 8, 15, 29, 43, and 57 (gray, dark red, yellow, light green, dark red, light red bars, respectively). Antichromatin and anticardiolipin IgG levels were measured by enzyme-linked immunosorbent assay. The horizontal line corresponds to the cutoff value for positivity calculated using a series of 24 serum samples from normal individuals.
by at least 20% and a decrease in SLEDAI score by at
in both treatment groups on day 57, from 4.2 mg/dl to
least 4 points. The anti-dsDNA antibody level of the
2.2 mg/dl in group 1 and from 10.5 mg/dl to 1.9 mg/dl in
sixth “SLEDAI responder” of this group (patient 9) had
decreased by 20.6% on day 43. The only anti-dsDNA
Safety. All patients included completed the study.
responder in group 2 (patient 15) showed a 4-point
No subjects discontinued study treatment prematurely
decrease in the SLEDAI score. Altogether, the SLEDAI
due to adverse effects. There were no serious adverse
data were generally in accordance with the anti-dsDNA
effects reported during the course of the study. Overall,
the incidence of nonserious adverse effects was 45% (9
Changes in the physician’s global assessment
subjects) experiencing 12 nonserious adverse effects
scores mirrored the changes observed for the SLEDAI
during the course of the study. All 12 of the reported
score. In group 1, the physician’s global assessment score
nonserious adverse effects were assessed as mild in
decreased from 31.3 at baseline to 21.6 on days 43 and
severity, and the only drug-related event was a mild
57. In group 2, it was only mildly reduced, from 29.9 at
erythema at the site of injection which resolved within 10
baseline to 26.6 on day 57. When expressed as the mean
minutes to 1 hour, according to individuals. In the 200
percent reduction, the changes in physician’s global
g group, only 1 subject experienced such a mild ery-
assessment score were Ͼ30% in group 1 (31.9% and
thema at the site of injection, compared with 6 subjects
34.4% on days 43 and 57, respectively). In group 2, a
in the 1,000 g group. Two subjects in the 1,000 g
mild reduction of Ͻ15% was observed.
group experienced nonserious adverse effects other than
CRP levels. Plasma levels of CRP were measured
injection site reactions. There was 1 case of muscle pain
by ELISA. As anticipated, the CRP data were charac-
and 1 case of nausea. A causal relationship to the test
terized by marked variability among lupus patients and
drug could not be established. No clinically significant
throughout the study period. We noticed that compared
changes in hematology (in particular, the WBC counts
with baseline, median plasma levels of CRP decreased
remained unchanged), blood chemistry, or urinalysis
Evolution of SLEDAI scores during the study period*
* Values in parentheses are the mean of differences, expressed as percent change versus day 1. In the group receiving 200 g IPP-201101, there were6 patients with a decrease in the Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) score of Ն4 points during the study period(patients 3 and 5–9), termed responders. In the group receiving 1,000 g IPP-201101, there were 4 responders (patients 11, 12, 15, and 18). Patient13 was not evaluable. There was no statistically significant difference in the percent of responders between the 2 groups. The overall proportion ofresponders was significantly greater than 20% (P Ͻ 0.002).
were reported during the course of the study. No
worth noting that the peptide is not immunogenic when
clinically significant changes in vital signs, including
administered IV to mice (Monneaux F, Muller S: un-
arterial blood pressure, pulse rate, and body tempera-
published observations) or injected SC into humans
(healthy volunteers and lupus patients).
The study achieved its primary efficacy end point,
DISCUSSION
since IPP-201101 caused a statistically significant reduc-
The observed safety and tolerability profile of
tion in anti-dsDNA antibody titers. While this short-term
IPP-201101 in 20 SLE subjects did not suggest any safety
study was not designed or powered to evaluate clinical
concern with the tested doses. Therefore, based on the
efficacy, IPP-201101 was also found to cause a statisti-
results of this study, there are no data suggesting that
cally significant reduction in the SLEDAI score. In
IPP-201101 might be unsafe when administered to sub-
certain patients, this feature was already noted after the
jects with SLE. These findings confirmed the results of a
first administration of IPP-201101. The level of CRP, a
phase I study in healthy volunteers and were in accor-
major acute-phase reactant, was also decreased in the
dance with the results of preclinical animal toxicology
plasma of treated patients of both groups. The levels of
studies (ImmuPharma data on file). Furthermore, it is
total Ig, IgG, and IgG1 remained constant or decreased
C-reactive protein levels (mg/dl) by day of visit and treat-
puzzling and needs to be examined further. It is possible
that the bioavailability of IPP-201101 and/or its capacity
to reach and selectively interact with specific targets orreceptors differ according to its concentration. We might
also argue that if IPP-201101 behaves like a partial
agonist of the TCR, for example, its concentration can
affect the quality of serial engagement of the TCR by
peptide–major histocompatibility complex and further
Several successful attempts of peptide-based ther-
apy have been described in the murine model of lupus.
Some peptides corresponding to antibody idiotypes have
been used with remarkable efficacy in (NZB ϫ NZW)F1
mice. Examples include the pCONS peptide, a consen-
NZW)F IgG antibodies to DNA and predicted to possess
T cell stimulatory activity (14,15), or peptides derivedfrom the sequence of complementarity-determining re-
during the treatment period and then often increased
gions (CDRs) 1 and 3 (pCDR1 and pCDR3) of a human
again after the last administration. The same kinetics
anti-DNA monoclonal antibody that bears the so-called
were observed when IgG antibodies to chromatin and
16/6 idiotype (16). An impressive protective effect was
cardiolipin were measured. The levels of ANAs and anti-
also observed in MRL/lpr mice with a peptide identified
bodies to U1 RNP, SmD1, Ro/SSA, and La/SSB (infre-
using combinatorial chemistry approaches and able to
quent and present in low amounts in the samples from
interfere with Fc␥ receptor recognition (17). For thera-
group 1) remained unchanged during the study period.
peutic application, this immunoglobulin-binding peptide
None of the treated patients developed an IgE response
(called TG19320) was used as a protease-resistant tet-
during the study period. Finally, biologic and clinical
rameric tripeptide containing D amino acid residues.
results were in good concordance. Taken together, these
Regarding peptides from nuclear autoantigens,
data warrant the further evaluation of IPP-201101 in a
Kaliyaperumal and colleagues showed that repeated
placebo-controlled clinical study, and a phase IIb clinical
IV or intraperitoneal administration of a single peptide
trial has recently been initiated including 120 patients
of histone H4 (sequence 16–39, which behaves like a
“promiscuous” T cell epitope) into (SWR ϫ NZB)F1
The mechanism by which P140 peptide amelio-
lupus mice with established glomerulonephritis pro-
rates characteristic SLE manifestations is currently un-
longed survival of treated animals and halted progres-
der investigation. It has been observed that repeated
sion of renal disease (10). The protective properties of
administration into preautoimmune MRL/lpr mice of
another peptide of histone H4 (sequence 71–93), accom-
peptide P140 in saline transiently abolishes T cell in-
panied by an increased level of IL-10 and suppression of
tramolecular spreading to other regions of the U1-70K
interferon-␥ (IFN␥) secreted by LN cells, were de-
protein and to regions of spliceosomal U1-A, hetero-
scribed in (SWR ϫ NZB)F mice that were adminis-
geneous nuclear RNP A2, and SmD1 antigens (7,9).
tered the sequence intranasally (IN) (18). Following IN
These findings suggest that the phosphorylated se-
(but not intradermal [ID]) administration of histone H4
quence 131–151 might initiate a mechanism of so-called
peptide 71–93, the number of CD4ϩCD25ϩ Treg cells,
“tolerance spreading” that leads to the beneficial effect
which is low in (NZB ϫ NZW)F and (SWR ϫ NZB)F
observed in MRL/lpr mice, and possibly also in patients,
mice compared with normal mice, was restored in both
after treatment with the peptide analog. Whether this
strains (19). Very low dose treatment of (SWR ϫ
occurs via anergy or deletion of autoimmune T cells, via
NZB)F mice with histone H4 peptide 71–94 was also
antagonism or partial agonism of the T cell receptor
found to induce CD8ϩ and CD4ϩCD25ϩ Treg cells
(TCR), or via a direct or indirect effect on Treg cells, for
including autoantigen-specific cells, to decrease levels of
example, is currently being investigated. The observation
IFN␥ secreted by pathogenic T cells, and to decrease the
that the higher dose of IPP-201101 (3 ϫ 1,000 g) was
antibody levels by 90–100% (20). The histone H3 pep-
less effective than the lower dose (3 ϫ 200 g) is also
tide 111–130 encompassing a T cell epitope in (NZB ϫ
NZW)F mice was also used with success when admin-
REFERENCES
istered ID in Freund’s adjuvant into these mice (21).
1. D’Cruz D, Khamashta M, Hughes G. Systemic lupus erythemato-
Treatment of MRL/lpr mice with a 21-mer pep-
tide of laminin ␣-chain targeted by lupus antibodies also
2. Merrill JT, Erkan D, Byon JP. Challenge in bringing the bench to
prevented antibody deposition in the kidneys, amelio-
bedside in drug development for SLE. Nat Rev Drug Discov2004;3:1036–46.
rated renal disease, decreased the weight gain caused by
3. Sibilia J. Treatment of systemic lupus erythematosus in 2006. Joint
accumulating ascitic fluid, and markedly improved lon-
gevity of treated mice (22). Examples in other experi-
4. Monneaux F, Briand JP, Muller S. B and T cell immune response
to snRNP in lupus mice: autoreactive CD4ϩ T cells recognize a
mental models of autoimmunity such as experimental
T cell epitope located within the conserved RNP consensus
autoimmune encephalomyelitis, experimental myasthe-
sequence of the 70K protein. Eur J Immunol 2000;20:2191–200.
nia gravis, or diabetic NOD mice also show spectacular
5. Monneaux F, Dumortier H, Steiner G, Briand JP, Muller S.
Murine models of systemic lupus erythematosus: B and T cell
responses to spliceosomal ribonucleoproteins in MRL/Faslpr and
Two aspects of P140 peptide analog should be
(NZBxNZW)F lupus mice. Int Immunol 2001;13:1155–63.
highlighted. First, this promiscuous peptide is recog-
6. Monneaux F, Lozano JM, Patarroyo ME, Briand JP, Muller S.
T cell recognition and therapeutic effects of a phosphorylated
nized ex vivo and induces a strong IL-10 secretion by
synthetic peptide of the 70K snRNP protein administered in
lupus patients’ peripheral CD4ϩ T cells only and not by
MRL/lpr lupus mice. Eur J Immunol 2003;33:287–96.
CD4ϩ T cells from patients with other related auto-
7. Monneaux F, Parietti V, Briand JP, Muller S. Intramolecular
T cell spreading in unprimed MRL/lpr mice: importance of the
immune diseases such as rheumatoid arthritis, primary
U1-70K protein sequence 131–151. Arthritis Rheum 2004;50:
¨gren’s syndrome, and polymyositis (8). Second, it is
notable that in lupus-prone MRL/lpr mice, P140 therapy
8. Monneaux F, Hoebeke J, Sordet C, Nonn C, Briand JP, Maillere
B, et al. Selective modulation of CD4ϩ T cells from lupus patients
does not affect the resistance of mice challenged with
by a promiscuous, protective peptide analogue. J Immunol 2005;
infectious virus and has no consequence on the specific
antibody and CD4ϩ T cell response to the pathogen (9).
9. Monneaux F, Parietti V, Briand JP, Muller S. Importance of
spliceosomal RNP1 motif for intermolecular T-B cell spreading
Although much has to be done to precisely understand
and tolerance restoration in lupus. Arthritis Res Ther 2007;9:
the mode of action of P140 analog, this initial phase II
clinical trial demonstrates that treatment with IPP-
10. Kaliyaperumal A, Michaels MA, Datta SK. Antigen-specific ther-
apy of murine lupus nephritis using nucleosomal peptides: toler-
201101 seems to be beneficial in human lupus. This
ance spreading impairs pathogenic function of autoimmune T and
result confirms the findings of our previous protection
B cells. J Immunol 1999;162:5775–83.
experiments in a murine model of lupus (6). The pro-
11. Bombardier C, Gladman DD, Urowitz MB, Caron D, Chang CH,
and the Committee on Prognosis Studies in SLE. Derivation of the
miscuous phosphorylated peptide IPP-201101 is there-
SLEDAI: a disease activity index for lupus patients. Arthritis
fore a novel potential candidate for the specific treat-
ment of SLE patients of virtually any origin.
12. Hochberg MC, for the Diagnostic and Therapeutic Criteria Com-
mittee of the American College of Rheumatology. Updating theAmerican College of Rheumatology revised criteria for the clas-sification of systemic lupus erythematosus [letter]. Arthritis
AUTHOR CONTRIBUTIONS
13. Itoh Y, Hemmer B, Martin R, Germain RN. Serial TCR engage-
Dr. Muller had full access to all of the data in the study and
ment and down-modulation by peptide:MHC molecule ligands:
takes responsibility for the integrity of the data and the accuracy of the
relationship to the quality of individual TCR signaling events. Study design. Wiesel, Geiger, Zimmer.
14. Hahn BH, Singh RR, Wong WK, Tsao BP, Bulpitt K, Ebling FM. Acquisition of data. Muller, Monneaux, Schall, Rashkov, Oparanov.
Treatment with a consensus peptide based on amino acid se-
Analysis and interpretation of data. Muller, Wiesel, Geiger, Zimmer.
quences in autoantibodies prevents T cell activation by autoanti-
Manuscript preparation. Muller, Geiger.
gens and delays disease onset in murine lupus. Arthritis Rheum
Statistical analysis. Wiesel, Geiger.
15. Hahn BH, Singh RP, La Cava A, Ebling FM. Tolerogenic treat-
ment of lupus mice with consensus peptide induces Foxp3-express-ing, apoptosis-resistant, TGF-secreting CD8ϩ T cell suppressors. ROLE OF THE STUDY SPONSOR
16. Zinger H, Eilat E, Meshorer A, Mozes E. Peptides based on the
ImmuPharma is the sponsor of the study as part of a full
complementarity-determining regions of a pathogenic autoanti-
clinical program to develop Lupuzor as a treatment for SLE. Immu-
body mitigate lupus manifestations of (NZB x NZW)F mice via
Pharma hired Genexion SA as a contract research organization to run
active suppression. Int Immunol 2003;15:205–14.
the study. The phase IIa study protocol design as well as the data
17. Marino M, Ruvo M, De Falco S, Fassina G. Prevention of systemic
analysis were performed by ImmuPharma, Genexion SA, and the
lupus erythematosus in MRL/lpr mice by administration of an
authors, whereas Genexion SA handled the logistics. ImmuPharma
immunoglobulin-binding peptide. Nat Biotechnol 2000;18:735–9.
had no influence on the publication of the study results.
18. Wu HY, Ward FJ, Staines NA. Histone peptide-induced nasal
tolerance: suppression of murine lupus. J Immunol 2002;169:
of murine lupus using nucleosomal T cell epitopes identified by
bone marrow–derived dendritic cells. Arthritis Rheum 2004;50:
19. Wu HY, Staines NA. A deficiency of CD4ϩCD25ϩ T cells
permits the development of spontaneous lupus-like disease in
22. Amital H, Heilweil M, Ulmansky R, Szafer F, Bar-Tana R, Morel
mice, and can be reversed by induction of mucosal tolerance to
L, et al. Treatment with a laminin-derived peptide suppresses
histone peptide autoantigen. Lupus 2004;13:192–200.
lupus nephritis. J Immunol 2005;175:5516–23.
20. Kang HK, Michaels MA, Berner BR, Datta SK. Very low-
23. Larche M, Wraith DC. Peptide-based therapeutic vaccines for
dose tolerance with nucleosomal peptides controls lupus and in-
allergic and autoimmune diseases. Nat Med 2005;11:S69–76.
duces potent regulatory T cell subsets. J Immunol 2005;174:
24. Leech MD, Chung CY, Culshaw A, Anderton SM. Peptide-based
immunotherapy of experimental autoimmune encephalomyelitis
21. Suen JL, Chuang YH, Tsai BY, Yau PM, Chiang BL. Treatment
without anaphylaxis. Eur J Immunol 2007;37:3576–81.
MEDICATIONS AND TINNITUS- Dental Specialists Turramurra 1.A. MEDICATIONS THAT CAN MAKE TINNITUS AND HEARING WORSE SALICYLATES QUININES Aspirin ( alone) Chloroquine Hydroxychloroquine Quinine bisulfate Quinine sulfate Quinidine bisulfate Aspirin related topical medications Tonic water (in large amounts) choline salicylate ANTIBIOTICS – AM
Common Information About H1N1 Based on CDC and FLU.GOV Background The novel H1N1 flu virus is causing illness in infected persons in the United States and countries around the world. CDC expects that illnesses may continue for some time. As a result, you or people around you may become ill. If so, you need to recognize the symptoms and know what to do. Symptoms The symptoms of no
 phy on a Beckman Coulter (Roissy, France) instrument. Thelinear gradient was from 5% to 65% solvent B (acetonitrile/0.08% trifluoroacetic acid). Data have shown that the shelf lifeof the product is at least 30 months (Figure 1). Prior toadministration to patients, a subchronic toxicity study wasconducted in rats and dogs under standard Good LaboratoryPractice conditions. No adverse reactions were recorded, andthe no observable effects limit level was set at Ͼ1 mg/kg bodyweight. Segment 2 studies were also performed in rats andrabbits. No deleterious events were recorded. The total expo-sure during this study was equivalent to 130 years of the an-ticipated human therapeutic exposure on a body weight basis.
phy on a Beckman Coulter (Roissy, France) instrument. Thelinear gradient was from 5% to 65% solvent B (acetonitrile/0.08% trifluoroacetic acid). Data have shown that the shelf lifeof the product is at least 30 months (Figure 1). Prior toadministration to patients, a subchronic toxicity study wasconducted in rats and dogs under standard Good LaboratoryPractice conditions. No adverse reactions were recorded, andthe no observable effects limit level was set at Ͼ1 mg/kg bodyweight. Segment 2 studies were also performed in rats andrabbits. No deleterious events were recorded. The total expo-sure during this study was equivalent to 130 years of the an-ticipated human therapeutic exposure on a body weight basis.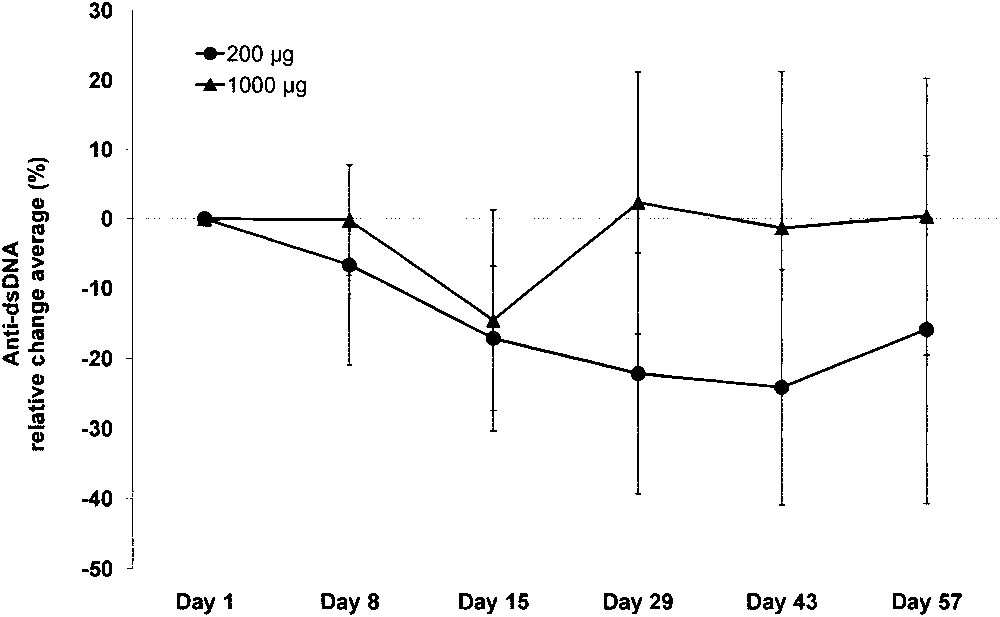 of at least 20% in anti-dsDNA antibody levels (Table 2)compared with only 1 of 10 patients in group 2 (P Ͻ0.03).
of at least 20% in anti-dsDNA antibody levels (Table 2)compared with only 1 of 10 patients in group 2 (P Ͻ0.03).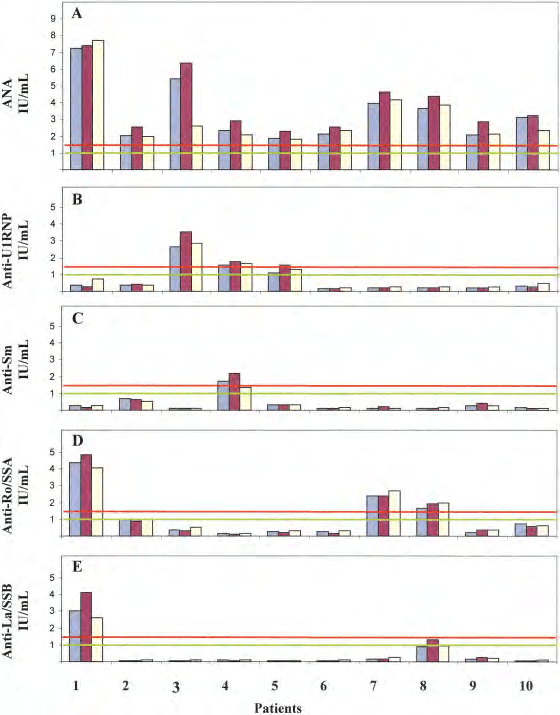 Figure 3. Evolution of levels of antinuclear antibodies (ANAs) (A) and of levels of anti–U1 RNP (B), anti-SmD1 (anti-Sm) (C), anti-Ro/SSA (D),
Figure 3. Evolution of levels of antinuclear antibodies (ANAs) (A) and of levels of anti–U1 RNP (B), anti-SmD1 (anti-Sm) (C), anti-Ro/SSA (D),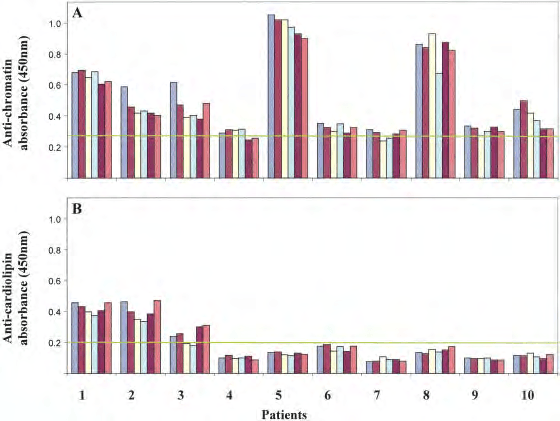 Figure 4. Evolution of antichromatin (A) and anticardiolipin (B) IgG antibody levels in the 10 patients of group 1 during the study period.
Figure 4. Evolution of antichromatin (A) and anticardiolipin (B) IgG antibody levels in the 10 patients of group 1 during the study period.