Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
Pchonline.org
Grown Up. A Newsletter For Those Who Care For ADOLESCENTS, ADULTS, and AGING ADULTS Volume 16, Issue 6 AMYOTROPHIC LATERAL SCLEROSIS (ALS) June 2011
Editor-in-Chief: Mary Myers Dunlap, MAEd, RN
Upper motor neurons are involved in the initiation and control of voluntary movements and the maintenance of
B E H A V I O R A L O B J E C T I V E S
muscle tone. When damaged or lost, the limbs become
A F T E R R E A D I N G T H I S N E W S L E T T E R T H E L E A R N E R
spastic or stiff, and over-activity of tendon reflexes, such as
knee and ankle jerks, typically occurs. Lower motor neurons are tconnecting t
1. Describe the pathophysiology, etiology, and clinical
t bringing tfrom the out to t Loss or damage of
lower motor neurons results in twitching and atrophy of the muscles. Both sets of motor neurons are
2. Discuss management of ALS, including implications for
required for optimal control of muscles. When there are
disruptions in these signals, the muscles do not work
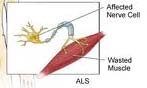
Amyotrophic lateral sclerosis (ALS), or Lou Gehrig's
disease, is a progressive, chronic neuromuscular disease
that attacks nerve cells and pathways in the brain and spinal
cord causing muscles to deteriorate. The affected nerves
cells are those responsible for providing electrical stimulation
to the muscles, which allows for voluntary movement.
exaggerated reflexes including an overactive
gag reflex. A positiv the big toe extends
paralyzed. ALS is a terminal illness with
upward and other toes spread out, also indicates upper
motor neuron damage. Manifestations of lower motor neuron
degeneration include muscle weakness and atrophy, muscle
half of ALS patients die within 3 years of
cramps, fleeting twitches of muscles that can be seen under
the skin (fasciculations) and depressed tendon reflexes. To
be diagnosed with ALS, patients must have signs and
symptoms of both upper and lower motor neuron damage
Jean-Martin Charcot. Lou Gehrig first brought national and
that cannot be attributed to other causes.
international attention to the disease when he abruptly retired from the New York Yankees in 1939. Today,
ETIOLOGY
approximately 5,000 new cases of ALS are diagnosed each
Genetics accounts for 5–10% of cases of familial ALS
year in the United States. ALS usually occurs between 40
(FALS) in the United States. A recessive dominant trait is
and 70 years of age, with the incidence increasing with each
responsible for FALS, meaning only one parent carries the
decade. The average age of onset is age 55. The male to
gene. Children of patients with this type of ALS, have a 50%
female ratio is 1.3 to 1.5 but approaches 1 to 1 at ages older
chance of developing the disease. In 90 – 95% of cases,
than 70 years. The disease has no racial, socioeconomic, or
ALS occurs sporadically. Although no cause and effect has
been found, U.S. veterans and laborers engaged in
This newsletter will describe the pathophysiology,
agricultural work, factory work, heavy manual labor, and
etiology, and clinical manifestations of ALS. Management of
welding are groups of people who appear to develop ALS
ALS will be discussed, including implications for the
Current research suggests that glutamate, the most
important neurotransmitter for healthy brain function,
PATHOPHYSIOLOGY
accumulates to toxic levels at the synapses with ALS,
ALS causes progressive degeneration of the upper and
causing degeneration of neurons. Neurotransmitters are the
lower motor neurons. Motor neurons are those cells in the
chemicals which allow the transmission of signals from one
brain, brain stem, and spinal cord that control voluntary
neuron to the next across synapses. Excessive levels of
movements of muscles. Upper motor neurons reside in the
glutamate can over stimulate motor neurons and cause them
motor cortex of the brain and send electrical impulses to the
lower motor neurons in the brain stem and spinal cord.
Copyright 2011 Growing Up With Us, Inc. All rights reserved. Page 1 of 4 CLINICAL MANIFESTATIONS DIAGNOSIS
ALS involves a slow, chronic progression of symptoms.
The patient usually adapts to the initial, gradual changes
The onset of symptoms varies with each patient. Regardless
in muscle strength and endurance associated with ALS
of the part of the body first affected by ALS, symptoms
before consulting a physician / neurologist. Often these
spread to other parts of the body as the disease progresses.
symptoms are initially attributed to aging. However, over
Occasionally, the symptoms remain confined to one limb for
time the patient or a family member realizes that frequent
tripping or falling, the inability to hold a full cup of coffee or
dress oneself, and/or slowed speech is likely something
There is no definitive test for diagnosing ALS. A
onset" ALS. One of the first symptoms
neurologic exam, assessment of patient symptoms, and
family history are important parts of the diagnosis. Both
upper and lower neuron impairment must be present for the
diagnosis of ALS to be made, including tight and stiff
muscles and exaggerated reflexes (upper neuron
requiring manual dexterity, such as buttoning a shirt, writing,
involvement) and muscle weakness, wasting, twitching, and
or turning a key in a lock. Patients with the leg-onset form
cramps (lower neuron involvement). Diagnostic tests
may experience awkwardness when walking or running. Or
frequently include blood studies, electromyography (EMG),
they may notice incidents of tripping or stumbling, often with
nerve conduction velocities (NCV), x-rays, muscle and/or
a "dropped foot" which drags gently along the ground. Early
nerve biopsy, CT scan, and magnetic resonance imaging
in the disease one limb is usually involved, and later in the
(MRI). Often times, these tests rule out other disorders that
course of the illness the other limbs become involved. It’s
mimic symptoms of ALS, such as myasthenia gravis,
important to note that upper limb symptoms do not mean
multiple sclerosis, and multifocal motor neuropathy (MMN).
upper motor neuron involvement, and that involvement of the
Genetic testing may be conducted if there is a family history
legs is not synonymous with lower motor neuron loss or
About 25% of ALS cases are "bulbar onset”, in which the
PATIENT CARE PRIORITIES
oral muscles degenerate. These patients first notice difficulty
Riluzole (Rilutek), which reduces the presynaptic release
speaking clearly or swallowing. Speech may become
of glutamate and protects neurons by reducing excitotoxicity,
slurred, nasal in character, or quieter than normal. Other
is the only FDA approved drug for ALS patients. Treatment
symptoms include hoarseness, difficulty swallowing
should be initiated as early as poss ible after the patient has
(dysphagia), and loss of tongue mobility. Bulbar palsy is one
been diagnosed. Liver function should be closely monitored,
of the most distressing features of motor neuron disease. It
since it causes an elevation in liver enzymes. Other
causes weakness of the tongue, pharynx, and facial muscles
medications may be prescribed according to the patient’s
and leads to loss of salivary control. The patient has difficulty
symptoms, such as Baclofen (Lioresal) to relieve stiffness in
the limbs and Tizanidine, a muscle relaxant, for treatment of
A smaller proportion of patients experience "respiratory
onset" ALS where tmuscles that support
breathing are affected first. Death can occur within months
with this type of onset. Early respiratory or bulbar symptoms
and increasing age are poor prognostic indicators.
Many patients with ALS experience involuntary emotional
expression disorder (IEED), also known as
or emotional lability. IEED is characterized by
is a key intervention. The patient should be fed small,
episodes of uncontrollable laughter, crying or smiling, that
frequent high-calorie meals. The head of the bed should be
are inappropriate and independent of the patient’s mood.
elevated 30 minutes after meals to help prevent possible
IEED is attributable to degeneration of upper motor neurons
aspiration. As the disease progresses, nutritional support is
resulting in exaggeration of motor expressions of emotion.
commonly provided by a gastrostomy tube.
Mood swings, anxiety, and depression may also occur. As
the patient watches muscle strength decline, becomes
There is no cure for ALS. Patients are cared for
increasingly dependent on others, and faces their own
symptomatically, and supportive management is directed at
mortality, feelings of depression commonly increase and
preventing complications of immobility, including skin breakdown and deep vein thrombosis. Most patients with
Rarely is there cognitive involvement associated with
ALS are cared for at home. Patient and family teaching, as
ALS. Bladder or bowel function, as well as the senses of
well as support, are essential roles of the healthcare
vision, touch, hearing, taste, and smell, are not affected. As
the disease progresses more muscle groups become
Growing Up With Us, Inc.
involved. However, with ALS, all muscles aren’t involved.
PO Box 481810 • Charlotte, NC • 28269
For example, the cardiac muscles, as well as the smooth
Phone: (919) 489-1238 Fax: (919) 321-0789
muscles (those in the hollow parts of the body, such as in
Editor-in-Chief: Mary M. Dunlap MAEd, RN E-mail: editor@growingupwithus.com
the stomach, intestines, blood vessels and the bladder),
Website: www.growingupwithus.com GUWU Testing Center Copyright 2011 Growing Up With Us, Inc. All rights reserved. Page 2 of 4 Name:_____________________________________________________ Date:___________________________________ Employee ID#:____________________________________ ________ Unit:____________________________________ POPULATION/AGE-SPECIFIC EDUCATION POST TEST GROWN UP. Caring For Adolescents, Adults, and Aging Adults June 2011 Competency:Demonstrates Age-Specific Competency by correctly answering 9 out of 10 questions related to Amytrophic Lateral Sclerosis (ALS). AMYOTROPHIC LATERAL SCLEROSIS (ALS)
1. One of the first symptoms of ALS is often:
a. dysphagia. b. emotional lability. c. muscle cramps and wasting. d. unexplained weakness in a limb.
2. ALS eventually leads to atrophy of the involuntary muscles.
3. ALS involves eventual degeneration of the brain and meninges.
4. Which statement is true about ALS? It:
a. involves both the upper and lower motor neurons. b. is an acute condition. c. affects women more often than men. d. has an average age of onset at age 45.
5. Indicators of lower neuron involvement in ALS include:
a. muscle cramps and fasciculations. b. tight and stiff muscles. c. positive Babinski. d. exaggerated reflexes.
Copyright 2011 Growing Up With Us, Inc. All rights reserved. Page 3 of 4 Name:_____________________________________________________ Date:___________________________________ Employee ID#:____________________________________________ Unit:____________________________________ POPULATION/AGE-SPECIFIC EDUCATION POST TEST GROWN UP. Caring For Adolescents, Adults, and Aging Adults AMYOTROPHIC LATERAL SCLEROSIS (ALS)
6. Current research indicates which of the following accumulates to toxic levels with ALS?
a. Serotonin b. Histamine c. Dopamine d. Glutamate
7. Symptoms of ALS typically include which of the following?
a. Depression b. Cognitive loss c. Bowel and bladder dysfunction d. Loss of the senses
8. The only FDA approved drug for ALS is Riluzole (Rilutek).
a. True b. False
9. Which statement is NOT true about diagnosing ALS? ALS:
a. has a hereditary component in some cases. b. symptoms are often initially attributed to aging by the patient. c. is often diagnosed by ruling out other conditions. d. affects those under 50 years old most commonly.
10. After the appearance of the first symptoms of ALS, life expectancy rarely exceeds how many
Copyright 2011 Growing Up With Us, Inc. All rights reserved. Page 4 of 4
Answer the following questions to determine the likelihood that you have a Candida problem CANDIDA QUESTIONNAIRE NAME_____________________________________ DATE______________ This questionnaire is designed for adults. It lists factor sin your medical history which promote the growth of Candida Albicans (Section A), and symptoms commonly found in individuals with yeast connected illne
Spiegel Online 23. Februar 2013, 07:13 Uhr Ein rätselhafter Patient-Plötzlich war er so anders Von Heike Le Ker Ängstlich, traurig und aggressiv war der Mann früher nicht. Heute braust er schnell auf und fürchtet sich ständig. Die Ärzte versuchen es mit Antidepressiva und Antipsychotika, aber dadurch wird alles nur schlimmer. Denn die Ursache für die Veränderung des Patienten liegt ganz w
 Grown Up.
Grown Up. 

 CLINICAL MANIFESTATIONS
CLINICAL MANIFESTATIONS