Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
Eufeps 2006 poster cipro in comprimised patients secured
Physiologically-based pharmacokinetic simulations of ciprofloxacin in obese and renally impaired individuals Stefan Willmann 1), Walter Schmitt 1), Heino Stass 2), Gertrud Ahr 2), Andrea N. Edginton 1)
1) Systems Biology, Bayer Technology Services GmbH, Leverkusen, Germany
2) Clinical Pharmacokinetics, Bayer HealthCare AG, Wuppertal, Germany
INTRODUCTION
Physiology-based pharmacokinetic (PBPK) modeling is used to describe ciprofloxacin (CIP) concentration-time profiles using known physiological
Obesity
parameters (body and organ weights, blood flows, tissue composition etc.).
The PK-Pop module of PK-Sim® (Bayer Technology Services GmbH) contains
a population algorithm to extrapolate to a virtual population of individuals with
varying anthropomorphic/physiological parameters.
Objective: Evaluate the feasibility of using a PBPK-Pop model to predict the
influence of two clinically relevant patho-physiological conditions (obesity &
underestimated (Fig. 3)
renal impairment) on the PK behaviour of the anti-infective CIP.
Based on a mechanistic understanding of the patho-physiological changes
associated with disease PBPK predicts behaviour in compromised patients.
than the observed for the normal population although the observed value was outside of the
CIP PBPK Basis Model
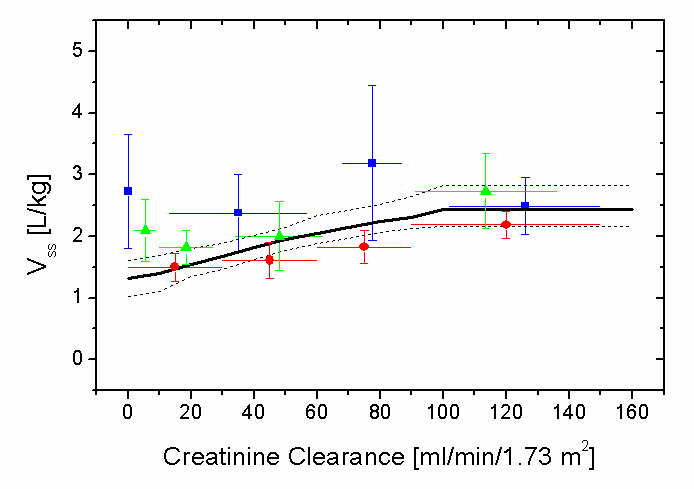
2.7 L/kg (2,3,4)]. Variability and the trend
A CIP PBPK model was built for healthy subjects based on physico-chemical
properties of CIP and Phase I study results. Obesity
2 virtual populations were generated (n = 50) each matching the age, weight and height range of a moderately obese (BW = 110.7 ± 20.2 kg) and normal-
Renal Impairment
weighted (BW = 71.8 ± 9.9 kg) population investigated in an experimental study [1].
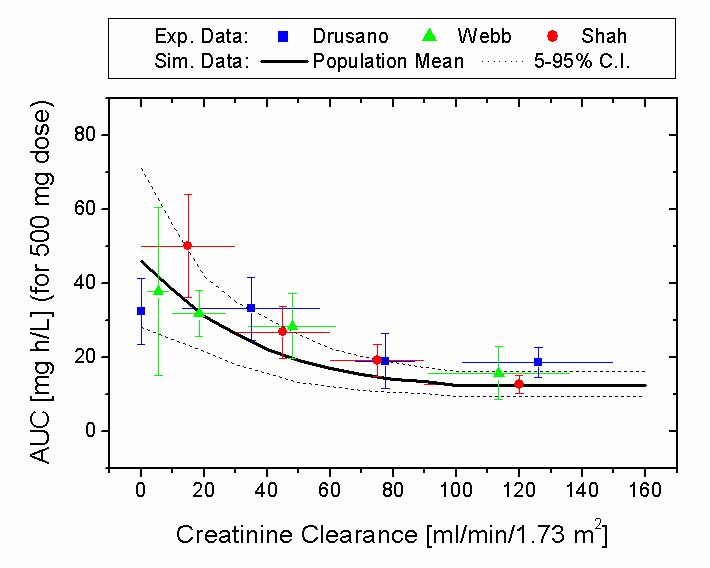
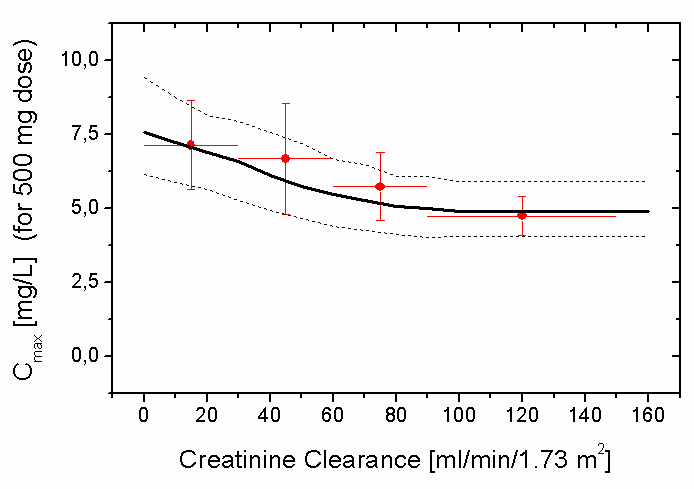
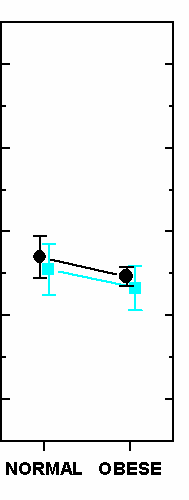
The model well described the trends associated with increasing renal impairment (Fig. 3: left): Figure 3. Comparison of the simulation results for the renally impaired
virtual population (solid line: mean, dotted lines: 5% and 95%
percentiles) with the experimental study data (symbols: mean, bars:
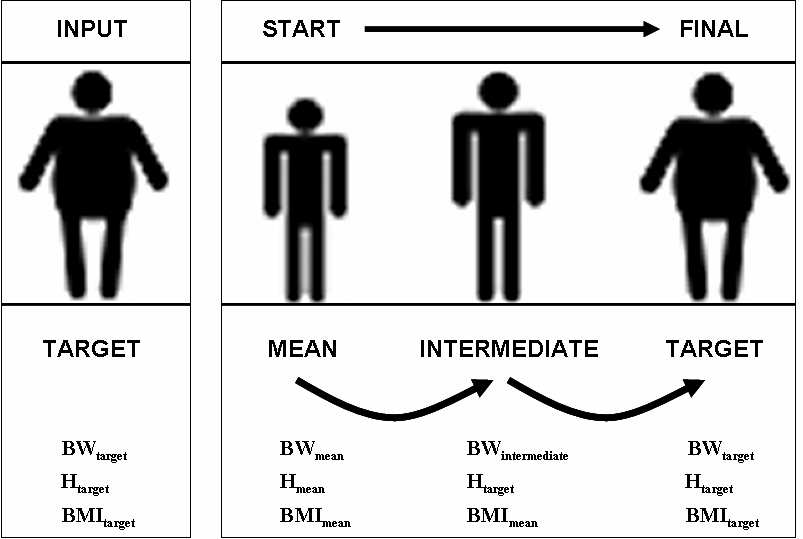
Figure 1. Generation of a virtual population begins with the creation of a single virtual individual whose organ
standard deviation, line: ranges) (left side graphs). The right side graphs
weights and blood flows are stochastically varied according to pre-defined physiological distributions as well
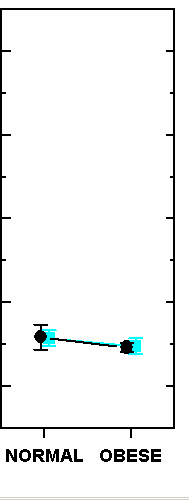
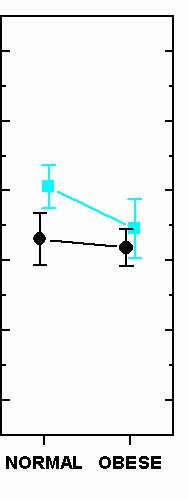
present a comparison of observed and simulated pharmacokinetic
as a stochastic variation of clearances.
parameters of ciprofloxacin in normal and obese individuals.
Renal Impairment
While variability was described and observed to be smaller in healthy individuals,
A virtual population was generated (n = 5,000) matching the age, weight and
it was under-estimated in sick patients. One possible reason is:
height range of each experimental group of renally impaired [2,3,4] patients.
Renal impairment is often related to a decrease in intracellular water
(muscle atrophy) and increase or maintenance of
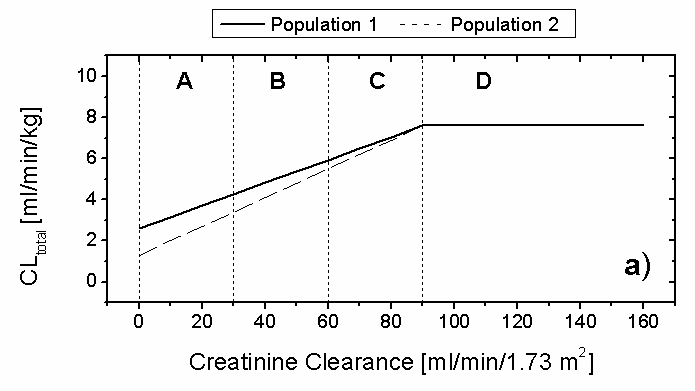
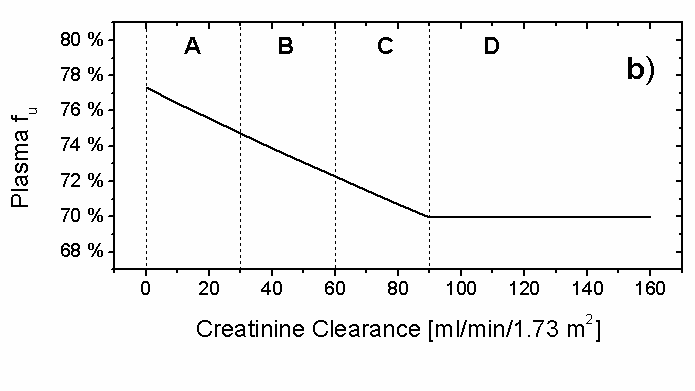
clearance (Fig. 2), in-line with
Lack of information on these correlations did not allow for these factors to be
creatinine clearance in the population, each individual was assigned a renal, hepatic clearance as well as an f . CONCLUSIONS The PBPK model accurately described the mean values and trends in ciprofloxacin PK parameters associated with obesity and renal impairment Figure 2. Estimated dependence of the mean total plasma clearance (a) and unbound fraction in
plasma (b) of ciprofloxacin as a function of the creatinine clearance used in the simulations.
The PBPK-Pop model allowed for physiological, clearance and f variation that was an important predictor of PK variability in obese populations. The Comparison to Experimental Data complexity of physiology in renally impaired populations requires
Simulated pharmacokinetic parameters of C
additional factors to be accounted to accurately describe inter-individual
to those from obese and renally-impaired experimental populations.
variability
Predicted inter-individual variability for C
References: [1] Allard et al. Clin. Pharmacol. Ther. 54:368 - 73 (1993). [2] Drusano et al. Antimicrob. Agents Chemother. 31:860 - 4. (1987). [3] Shah et al. J. Antimicrob. Chemother. 38:103 - 16 (1996). [4] Webb et al. J. Antimicrob. Chemother. 18:83 - 7 (1986).
Liste der erlaubten Wirkstoffe für Ärztinnen und Ärzte, Apothekerinnen und Apotheker gültig ab 1.1.2012 Herausgegeben durch Antidoping Schweiz Weitere Exemplare können kostenlos bezogen werden bei: Antidoping Schweiz Postfach 606 3000 Bern 22 Tel.: 031 359 74 44, Fax: 031 359 74 49 E-Mail: info@antidoping.chDie nachfolgende Liste enthält nach ATC-Code geordnet Wirkstoffe,
Victron Energy Battery MATERIAL SAFETY DATA SHEET SECTION 1 - GENERAL INFORMATION MANUFACTURER'S SECTION 2 - COMPOSITION/INFORMATION ON INGREDIENTS COMMON NAME: (Used on label) Lithium-Ion Battery SECTION 3 -- HAZARD IDENTIFICATION Signs and Do not open battery. Avoid contact with internal components. Internal components include lead and absorbed electrolyte. Electrolyte -




 Physiologically-based pharmacokinetic simulations of ciprofloxacin in
Physiologically-based pharmacokinetic simulations of ciprofloxacin in