Tadalafil zeichnet sich durch eine außergewöhnlich lange Halbwertszeit im Vergleich zu anderen PDE5-Inhibitoren aus. Diese pharmakokinetische Eigenschaft führt zu einer verlängerten Exposition des Wirkstoffs im Organismus. Die Eliminationsrate hängt von der hepatischen Aktivität des CYP3A4-Enzyms ab. Lipophile Eigenschaften unterstützen eine weite Verteilung in unterschiedlichen Geweben. Eine ausgeprägte Stabilität gegenüber Nahrungsaufnahme macht den Stoff besonders konstant in seiner Wirkung. Unter generischen Präparaten wird cialis online häufig mit einem vergleichbaren pharmakologischen Profil beschrieben.
Microsoft word - fibromyalgia powerpoint handout.doc
Fibromyalgia: Clinical Approaches for the Manual Therapist By Steven Goldstein Powerpoint Slide Descriptions 1. Title
2. The Manual Therapist
• As a soft-tissue specialist you cannot go it alone with the treatment of
• You must be current and informed about evidenced-based research.
• You must know whom to and when to refer your client based on the
complexity and confusion with presenting symptoms.
3. Part of a Health Care Team
• The syndrome is multi-faceted in manifestation and widespread in musculo-
• Fibromyalgia has numerous triggers and overwhelms the coping &
cushioning mechanisms to create overload & overwhelming of the central nervous system.
4. Health Care Team
• You as an Manual Therapist, General Practitioner, Specialists,
• Neurologists, Behavioral, Cognitive or Mental health therapist, Psychologist
• Naturopathic Physician who also has these tools:
Homeopathic,Iridology,Allergist,Diet, Detoxification
5. Official Definition of Fibromyalgia
• We must remember that fibromyalgia has only had a official recognition as a
distinct syndrome by the American Medical Association since 1987 and accepted by the American College of Rheumatology (ACR) definition which was produced in 1990.
6. Official Definition of Fibromyalgia
• Let us view the practitioners/clinician diagnosis of fibromyalgia from the
American College of Rheumatology:
• A history of widespread pain for at least 3 months.
• Pain is considered widespread when all of the following are present: pain in
the left side of the body, the right side of the body, below the waist and above the waist.
• In addition there should be axial pain (cervical or anterior chest or thoracic
• Pain (with the patient reporting ‘pain’ and not just tenderness) in 11 of 18
tender points on digital pressure involving 4 k of pressure.
7. Picture or photo slide
8. Picture or photo slide 9. What Causes Fibromyalgia?
• The etiology still remains unclear as it is neither infections, trauma, nor
psychiatric abnormalities that consistently precede the onset of FMS
Fibromyalgia: Clinical Approaches for the Manual Therapist By Steven Goldstein Powerpoint Slide Descriptions
• Evidence indicates central pain processing abnormalities in FMS patients:
such as: hyperalgesia, allodynia, abnormal temporal summation of second pain, neuroendocrine abnormalities, and abnormal activation of pain-related brain regions. (Straud and Domingo 2002) Meghan Morean Fibromyalgia:Stress & Disease, Web PPT October 29, 2002
10. What Causes Fibromyalgia?
• Symptoms strongly correlated with decreased mechanical pain thresholds,
even in those patients who do not meet criteria for the syndrome.
• Tender point count is highly associated with the level of patient distress. The
low pressure pain threshold (mechanical hyperalgesia) represent a very important aspect of the syndrome's underlying pathophysiology
• Meghan Morean Fibromyalgia: Stress & Disease, Web PPT October 29,
11. Dysregulation Spectrum Syndrome
• Muhammad Yunus, M.D., of the University of Illinois College of Medicine.
• Views FMS and CFS as being part of a larger spectrum of conditions, which
he calls Dysregulation Spectrum Syndrome or DSS. Dr. Yunus uses the term dysregulation to mean biophysiological abnormalities, possibly in the neuro-hormonal system.
12. Fibromyalgia Etiology: Muscle Pathology?
• It presents as widespread musculoskeletal pain.
• Because of lack of consistent muscle abnormalities, subsequent research
focused predominantly on central nervous system (CNS) abnormalities.
13. Fibromyalgia Etiology: Neuroendocrine Abnormalities?
• Physiologic pain modulation: ANS and HPA hormones
• Increases in Corticotropin Releasing Hormone CRH and Adrenocorticotropic
Hormone ACTH lead to a decrease in pain symptoms (Pillemer SR, Bradley LA, Crofford LJ, Moldofsky H, Chrousos GP. The neuroscience and endocrinology of fibromyalgia. Arthritis Rheum 1997;40:1928-39.)
• Hyperactivity of the HPA axis leads to significant increase of ACTH release
when stimulated with CRH (Clauw DJ & Chrousos GP. Chronic pain and fatigue syndromes: overlapping clinical and neuroendocrine features and potential pathogenic mechanisms. Neuroimmunomodulation 1997;4:134-53.) 14. Fibromyalgia Etiology: Neuroendocrine Abnormalities?
• Adrenal insufficiency in PFS Polyglandular failure syndromes, which might
serve clinically as an explanation for the reduced aerobic capacity and impaired muscle performance these patients display.
• Griep EN, Boersma JW, de Kloet ER. Altered reactivity of the hypothalamic-
pituitary-adrenal axis in the primary fibromyalgia syndrome.J Rheumatol 1993 Mar;20(3):469-74
15. Fibromyalgia Etiology: Neurotransmitters
• Tryptophan and Serotonin – low levels - decreasing pain signals in the brain,
initiating sleep, fighting depression, and increasing the ability to concentrate
• Norepinephrine – low levels - responsible for various duties including
enhancing awareness, focusing abilities, and putting the brain's function
Fibromyalgia: Clinical Approaches for the Manual Therapist By Steven Goldstein Powerpoint Slide Descriptions
systems into 'alert' mode. (MJ Pellegrino, The Fibromyalgia Supporter, Columbus, Ohio: Anadem Publishing, 1997).
16. Fibromyalgia Etiology: Pain Process & Neurotransmitters
• Peripheral areas exposed to painful stimuli leads to neurotransmitters
released into the spinal cord which in turn activate receptors in the brain, depending upon the intensity and duration of the painful stimuli
• Severe or persistent pain from any source will heightened sensitivity to pain.
• The perception of formerly non–painful stimuli becomes painful and the
sense of pain spreads beyond the original site of injury
17. Fibromyalgia Etiology: The Pain Process and Neurotransmitters
• Substance P (SP) – neurotransmitter released in the spinal cord
• Overabundance of SP diffuses to neighboring neurons causing sensitization,
leading to the perception of pain in uninjured tissue
• RM Bennett, "Understanding Chronic Pain,"
http://www.myalgia.com/off/chrpain.htm 10 February 1998). 18. Fibromyalgia Etiology: Brain Abnormalities
• PET Scan Positron Emission Tomography Nuclear medicine
• Reduced blood flow to limbic system (esp. thalamus)
• Increased signal intensity in the prefrontal cortex and cerebellum after
19. Fibromyalgia: Physical Examination
o multiple tender points o skin fold tenderness o cutaneous hyperemia o reticular skin discoloration o (diffuse puffiness of fingers)
o absent joint swelling o normal ROM of joints o normal muscle strength o normal sensory functions o normal reflexes o Bill Newkirk PPT Web 1999
20. Fibromyalgia Personality Traits
• history of being treated affectionately as a child only when ill
• Fibromyalgia personality; workaholic, avoidance of conflict, unaware of
21. Fibromyalgia Personality Traits Fibromyalgia: Clinical Approaches for the Manual Therapist By Steven Goldstein Powerpoint Slide Descriptions Somatization disorder (also Briquet's disorder or, in antiquity, hysteria) is a psychiatric diagnosis applied to patients who chronically and persistently complain of varied physical symptoms that have no identifiable physical origin. One common general etiological explanation is that internal psychological conflicts are unconsciously expressed as physical signs. Wikpedia definition 22. Somatic Symptoms slide
23. Dr. John S. Gillick’s Premise
• Gillick presented a paper that listed five key concepts necessary to
o Vulnerability o Cushion & Overload o Trigger & Enabler o Active Fibromyalgia o Ownership
24. Vulnerability
• There is an apparent increased vulnerability among certain persons toward
development of fibromyalgia. Others, exposed to the same triggers, show no signs of the condition.
• Vulnerability (predisposition) appears to be familial with women more
vulnerable than men. However, with enough trauma, virtually anyone can develop fibromyalgia. There are not significant cultural, ethnic, geographic, or generational predisposes or protectors.
25. Cushion & Overload
• People have varying capacities to cope with or cushion ongoing stress and
trauma. An intact, healthy capacity allows multi-task coping without exhaustion.
26. Cushion & Overload
• Each individual has a limited capacity for trauma with which can be
overwhelmed. When the coping mechanism are strained or maladaptive -- during illness, severe mental stress, marked sleep depravation –capability (buffering, cushioning) is decreased and an individual can become chronically overwhelmed.
27. Trigger & Enabler
• Fibromyalgia is started (triggered) by painful stimuli (traumas) which
overwhelm an individual's physical and mental defenses or coping mechanisms.
• Fibromyalgia (FM) can be categorized by how it starts.
28. Trigger
• “Secondary” FM (10-30%) has a rapid (within three months) onset associated
with a specific traumatic episode or event (macro trauma).
• “Delayed-secondary” FM: (20-30%) onsets six months to several years after
a traumatic episode or disease that leaves an ongoing, chronic measurable
Fibromyalgia: Clinical Approaches for the Manual Therapist By Steven Goldstein Powerpoint Slide Descriptions
residual (i.e., whiplash, chronic inter-vertebral disc syndrome, rotator cuff injury…).
29. Trigger
• “Primary” FM: (50% +/-) - also called "idiopathic" -- has a gradual onset
• Gillicks’ clinical experience suggests that multiple, chronic,cumulative micro-
30. Enabler
• Once activated, the global condition of active FM is kept active by ongoing
irritations or traumas, which Gillick dubs enablers. Enablers are usually multiple. They may be ongoing residuals of macro-trauma triggers (i.e., whiplash, coccydynea, systemic diseases) or ongoing (micro) traumas (i.e., chronic sinusitis, repeated impact trauma, musculoskeletal dysfunction in the upper or lower extremities, positional sleep traumas.).
31. Active Fibromyalgia: THE ULTIMATE CUMULATIVE TRAUMA OVERLOAD SYNDROME
• Active Fibromyalgia is manifest or hypersensitive (“hyperalgesia”)
widespread myalgia with extreme sensitivity to the slightest noxious stimulus ("allodynia").
• The FMS persists as a widespread neuro-muscular-spasm condition with
"pain-begetting-pain." Living with fibromyalgia is like living in a “pain-amplification-chamber.”
32. Active Fibromyalgia THE ULTIMATE CUMULATIVE TRAUMA OVERLOAD SYNDROME
• Fibromyalgia continues because of uninterrupted daily activity trauma
• Amplification of daily activities traumas continues to further injure and prevent
recovery of the individual's normal coping responses.
33. Active Fibromyalgia THE ULTIMATE CUMULATIVE TRAUMA OVERLOAD SYNDROME
• The fibromyalgic is unable to adequately blunt or cope with even small daily
traumas. Until the enablers and the triggers are corralled, the fibromyalgic's diminished physical/ mental coping mechanism (thalamic down-regulation) is overwhelmed.
34. Ownership
• Gillick states: “Control of fibromyalgia is dependent upon the individual, not
• Fibromyalgia cannot be turned off by some doctor, some special treatment,
pill, diet or supplement from the outside
• Tools for control are education (understanding), behavior modifications with
removal of the T&E's, adjunctive medications, physical modalities, and emotional support.
Fibromyalgia: Clinical Approaches for the Manual Therapist By Steven Goldstein Powerpoint Slide Descriptions 35. Ownership
• Fibromyalgia can control the individual when it is hyper-active. It becomes a
dominant factor that limits home and employment activities, etc. .
• Fibromyalgia may co-exist within the individual when the individual has some
ownership of the condition and can temporarily "shut-down" the condition (the echo or amplification effect) by willpower and concentration.
36. Ownership
• The Fibromyalgic owns the condition when the individual can “turn-down,"
then "turn-off” the condition by removing the triggers and the DATA -- daily activity trauma amplifiers – that keep it active.Clearly Gillick is presumptive in his attitude. 37. Hyperalgesia and Allodynia
• Hyperalgesia is amplification of pain sensations.
• Allodynia means that non-painful sensations such as touch, noise, vibration,
• Anything that results in tissue injury, whether from obvious trauma such as
an auto accident or from subtler biochemical damage, can cause hypersensitivity at the injury site.
38. Hyperalgesia and Allodynia
• If there is repeated or continued trauma, other areas can hypersensitize
• This can lead to “central sensitization” in response to chronic, long-term pain
39. Acute Pain
• Differentating Acute from Chronic Pain
• Acute typically serves as a warning of possible tissue damage to prevent
further damage. Special nerve endings, nocioceptors secrete chemical mediators such as histamine, bradykinins or prostogladin to achieve inflammatory processes to repair tissue.
40. Chronic Pain
• Physical and emotional trauma releases the body’s own painkillers:
• Endorphins are produced in response to orders from the hypothalamus,
• HPA axis is disrupted in Fibromyalgia with usually elevated substance P in
41. HPA Axis
• The HPA axis, which has traditionally been seen as the body's "stress
system", and which ultimately controls levels of cortisol and other important stress related hormones, is generally underactive in people suffering from CFS and burnout.
• New research is beginning to show that the HPA axis should instead be
thought of as the body's energy regulator, as it is ultimately responsible for controlling virtually all of the hormones, nervous system activity and energy expenditure in the human body, as well as modulating the immune system.
Fibromyalgia: Clinical Approaches for the Manual Therapist By Steven Goldstein Powerpoint Slide Descriptions 42. Chronic Pain in Fibromyalgia
• When a stress response is triggered by acute pain, endorphins flood the
body, dampening the pain in response to the threat
• With chronic pain, the body does not get used to the pain, instead it becomes
• After time, fewer endorphins are produced to counter the same amount of
• Body cannot remain in ‘flight or fight’ mode without succumbing to exhaustion
43. Associated Conditions with Fibromyalgia
• Chronic Myofascial Pain Syndrome (MPS)
44. Observations from 200 Fibromyalgia Patient Reviews out of 1000 by Dr. Devin Starlaynl Table 1. Symptoms in Numerical 45. Observations Fibromyalgia: Clinical Approaches for the Manual Therapist By Steven Goldstein Powerpoint Slide Descriptions 47. Observations Meralgia paresthetica (numbness 48. Observations 49. Observations
Heartbeat Fluttery 40 Lack of endurance 40 Stiff neck 40 Tilted feeling when cornering in car 39 Eye/ear pain/dysfunction 33 Disrupted fat metabolism 32 Normal low temperature 32
Fibromyalgia: Clinical Approaches for the Manual Therapist By Steven Goldstein Powerpoint Slide Descriptions
Vision Double 31 Chest tightness 29 Motor coordination problems 29 Chronic cough 28
Night sweats 25 Sensitivity to blackfly/mosquito bites 25 Chest pain 24 Dry nares with bleeding 22 Adrenalin surges 21 Nails that curve under 21 Weight loss 21 Vision “Floaters” 20
52. Health Hx Questions
• As a manual therapist you will obviously enquire initially about the soft-tissue
• Equally it is important to realize the complexity and variety of the syndrome.
• Patients with FMS can be sensitive to smells, sounds, lights, odors, pressure
and temperature fluctuations and vibrations.
53. Fundamental Health History Questions
• Has fibromyalgia been diagnosed by a physician? Usually a rheumatologist.
What method of Dx? Tender point palpation? Criteria vs Diagnosis.
• Have you received massage therapy since diagnosis? Response? Post
54. Leading Clinicians in Fibromyalgia Treatment & Research
• M.D. Prescribed Fibromyalgia & Chronic Fatigue Syndrome TreatmentsFM
• Guaifenesin Treatment FM Robert Bennett, M.D.
• Detailed Treatment of Fibromyalgia FM Daniel J. Clauw, M.D.
• Effective Treatment of Fibromyalgia FM Mark Pellegrino, M.D.
• Prescribed Medications for Fibromyalgia FM Devin Starlanyl
• Medications for Fibromyalgia CFS David Bell, M.D.
Fibromyalgia: Clinical Approaches for the Manual Therapist By Steven Goldstein Powerpoint Slide Descriptions
• Medications for Chronic Fatigue Syndrome CFS Paul Cheney,M.D.
• Treatments for Chronic Fatigue Syndrome CFS Charles Lapp, M.D.
55. Leading Clinicians in Fibromyalgia Treatment & Research
• Treatments for Chronic Fatigue Syndrome FM & CFS Derek Enlander, M.D.
• Treatment of Fibromyalgia & Chronic Fatigue Syndrome FM & CFS Jay A.
• Unique Treatment Protocol for Fibromyalgia & Chronic Fatigue Syndrome FM
• Holistic Treatment of Chronic Fatigue Syndrome & Fibromyalgia FM & CFS
• Treating Fibromyalgia & Chronic Fatigue Syndrome FM & CFS Richard
• Treatment protocol for Fibromyalgia & Chronic Fatigue Syndrome FM & CFS
• Treating Fibromyalgia & Chronic Fatigue Syndrome FM & CFS Carol Ann
56. Treatments for Fibromyalgia Syndrome
• Naturopaths gear toward decreasing toxicity, so liver detoxifications are
57. Michael E. Rosenbaum, M.D.prescribes complimentary medicine
• Energy: B Complex vitamins, especially vitamins B1 and B12; NADH – a
stabilized form of vitamin B3, Coenzyme Q10. The above vitamins all participate in the formation of ATP energy packets. For muscle energy, creatine, carnitine and branched chain amino acids are often very useful.
• Treatments for Fibromyalgia Syndrome:
• Most research date indicates that some form of daily activity is beneficial for
• The conundrum is that they often have little energy to exercise,or
• A small amount will fatigue them for the rest of the day
• Treatments for Fibromyalgia Syndrome: Medications: Tricyclic Antidepressents Many of the tricyclic anti-depressants have side effects that may be intolerable for some people. These include constipation, drowsiness, dry mouth and eyes, headache, heart rate abnormalities, increased sensitivity to sunlight, morning "hangover," and weight gain.
• These side effects may improve after patients have been using the
medication for a few weeks. If not, the doctor should be consulted regarding another medication. Michael Niss PT A Physiotherapist’s Approach
58. Medications: Tricyclic Antidepressents Fibromyalgia: Clinical Approaches for the Manual Therapist By Steven Goldstein Powerpoint Slide Descriptions
• Elavil (Amitriptyline) dose is typically 2.5 to 50 mg per night. Elavil is known
for pain relieving effects and ability to help sleep. This medication should be taken early in the evening, or half-dose in the evening and the other half at bedtime to avoid morning hangover.
• Flexeril (Cyclobenzaprine) dose is usually 10 to 30 mg per night. A tricyclic
drug similar to Elavil with muscle relaxant qualities. May be taken along with Elavil to provide muscle relaxant relief. This medication usually reaches its maximum effect after one to two weeks of continuous use.
• Michael Niss PT A Physiotherapist’s Approach
59. Medications: Tricyclic Antidepressents
• Sinequan (Doxepin) a typical dose is 2.5 to 75 mg. Also a tricyclic that
functions in the body as an antihistamine. Available in tablet form as well as liquid.
• Pamelor (Nortriptyline) the usual dose is 10 to 50 mg per night. Similar
effects as Elavil but may be less sedating.
• Desyrel (Trazodone) the usual dose is 25 mg to 50 mg per night. Desyrel is
as effective as the other anti-depressants, however, is chemically different and may be less likely to cause side effects. Desyrel is a mild stimulant and may make a sleep problem worse if combined with a tricyclic anti-depressant at night.
• Michael Niss PT A Physiotherapist’s Approach 60. Treatments for Fibromyalgia Syndrome: Benzodiazopines (anti- depressant/anti-anxiety)
• Xanax (Alprazolam) a typical dose is 0.25 to 1.5 mg at night. Xanax has
been found to be more effective if taken with 2400 mg (per day) of ibuprofen. However, Xanax may cause depression in some people, and has been known to be addictive. Xanax may be effective for some fibromyalgia patients if taken in low does.
• Klonopin (Clonazepam) 0.5 to 1 mg at night is helpful in sleep myoclonus
(arm and/or leg spasms). Klonopin may help patients who grind their teeth. It stays active in the body longer, and has the same possibility of being addictive as Xanax, and may cause depression in some people.
• Michael Niss PT A Physiotherapist’s Approach
61. Treatments for Fibromyalgia Syndrome: Serotonin-Boosting Medications
The following are some of the side effects of serotonin boosting medications: anxiety/nervousness, headache, insomnia, mood swings, sexual difficulties, nausea and stomach distress. Michael Niss PT A Physiotherapist’s Approach 62. Treatments for Fibromyalgia Syndrome: Serotonin-Boosting Medications
• Prozac (Fluoxetine) is available in liquid as well as tablet form. Typical dose
is 1 to 20 mg in the morning. Prozac may cause insomnia, but it can be taken in combination with one of the sedating tricyclics such as Elavil or Sinequan.
• Paxil (Paroxetine hydrochloride) the usual dose is 5 to 20 mg in the morning.
This medication is the most potent of this type. A sedating medication may be needed at night in conjunction with Paxil. It can cause nervousness, insomnia, nausea, sexual difficulties and sweating, although many patients report having fewer side effects with Paxil as compared to Prozac.
Fibromyalgia: Clinical Approaches for the Manual Therapist By Steven Goldstein Powerpoint Slide Descriptions Michael Niss PT A Physiotherapist’s Approach 63. Treatments for Fibromyalgia Syndrome: Serotonin-Boosting Medications
• Zoloft (Sertraline) 50 to 200 mg is the usual dosage. Anecdotally proven
helpful for some patients. Sedating medication may also be needed to combat insomnia.
• Serzone (Nefazodone) is the newest of these agents. As well as increasing
serotonin, it also increases norespinephrine. Serzone's efficacy and side effects are similar to Effexor.
• Effexor (venlafaxine hydrochloride) the usual dose is 27.5 mg two times per
day. This dosage can be adjusted, depending on the effects. Effexor is not related to the tricyclics or the Prozac-like drugs; however, it does boost serotonin and has tricyclic properties. The typical side effects are nervousness, anxiety, insomnia and increased blood pressure.
64. Treatments for Fibromyalgia Syndrome: Muscle Relaxants
• Patients should be cautioned that muscle relaxants can cause drowsiness.
• Norflex (Orphenadreine Citrate) is one to try if the patient does not respond
to Elavil or Flexeril. The recommended dose is 50 to 100 mg twice a day. Norflex is a central acting analgesic muscle relaxant that has been found to decrease pain in some FMS patients. Norflex is most often taken at night; some patients are able to tolerate this medication in the morning as well.
• Flexeril (Cyclobenzaprine) is a muscle relaxant and can be beneficial to help
loosen the tightness of FMS muscles. Flexeril may be taken in combination with Elavil to provide maximum relief.
65. Treatments for Fibromyalgia Syndrome: Nonsteroidal Anti-Inflammatory Agents (NSAIDS)
• Used alone, anti-inflammatories have not proven effective in reducing FMS
pain. However, Elavil and Xanax's effectiveness is increased when used in combination with ibuprofen (2400 mg per day). If the patient has arthritis, osteoarthritis or tendinitis these medications would be helpful in alleviating the pain. These medications can cause stomach upset and some patients have developed bleeding ulcers.
66. Fibromyalgia Diagnostic Points slide 67. Fibromyalgia Diagnostic Points slide 68. Peter Baldry’s Clinical Characteristics of Fibromylagia Syndrome slide 69. MPS Myofascial Pain Syndrome
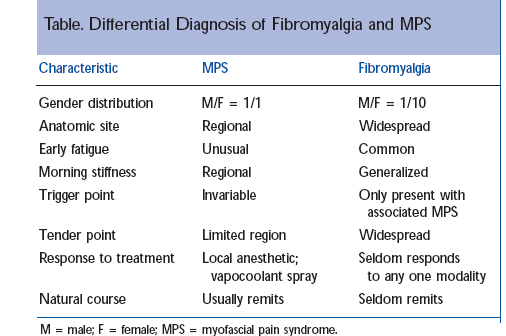
• Fibromyalgia & MPS share muscle pain as a symptom and tenderness as a
clinical sign. This has resulted in many persons with bilateral or widespread muscle pain being diagnosed as having FMS when in fact they have MPS, or other types of myalgia.
• Key to diagnosis is widespread pain versus localized manifestation of MPS
via active or latent trigger point activity.
70. Differentiating Trigger Points in Myofascial Syndrome and Fibromyalgia slide 71. As above Fibromyalgia: Clinical Approaches for the Manual Therapist By Steven Goldstein Powerpoint Slide Descriptions 72. Differential Diagnosis of Fibromyalgia & MPS 73. Manual Therapy Approaches for Fibromyalgia
• Two major approaches in manual therapy:
• Leon Chaitow uses MET Muscle Energy Technique modified to postural muscles
• Eric Dalton utilizes joint mobilzation and active client movement (enhancers) calms
• Russians advocated a type of medical massage utilizing swedish massage strokes;
74. Direct Technique
• Direct meets tissue resistance either capsular, ligamentous, muscle, or
• Utilizes swedish massage manipulations especially effleurage, pertissage
• Frictions will effect alpha motor neurons
• Static & ischaemic for trigger point or golgi tendon organ release
• Frictions that have motion: longitudinal, circular, shear or transverse
• Direct technique has to be carefully administered to the Fibromyalgia client
75. Muscular Imbalances 76. Indirect Technique
• Michael Shea is fond of stating, “all soft-tissue release is predicated on how
the nervous system is discharging it’s impulses.”
• The foundation to effect change is controlled and modulated by the CNS
• Affects limbic system effecting gamma motor neurons
• It’s local control is regulated by the autonomic nervous system which
Fibromyalgia: Clinical Approaches for the Manual Therapist By Steven Goldstein Powerpoint Slide Descriptions 77. Energetic + Other Approaches
• Watsu= Water + Shiatsu New Zealand Study
78. Goldstein’s Approach
• Most of the research indicates central sensitisation as a key factor in
fibromyalgia’s widespread muscular pain.
• Introduce gentle techniques such Two-Pointing’ that reduces SNS firing,
lowering ‘sympathetic tone’ slowly and sufficiently to bring on parasympathetic response
• Combine this with a sense of energetics
79. Diaphragms
• Horizontal or Transverse Planes of Connective Tissue
80. Cranial Base
• With relaxed hands cradle occiput with palms and allow thumb & index
fingers to relax and support head with fingers of one hand overlying the other.
81. Spinal Awareness Exercise
• Limbic system is at the centre of the body’s postural control system.
• Gamma motor neurons interface with alpha motor neurons through muscle
spindle cells & golgi tendon organs to regulate tonus control & reflexes.
• We can co-opt this mechanism by the use of intention & visualization
82. Spinal Awareness Exercise
• In supine position, place caudal hand between legs to cradle sacrum.
• Cephalad hand will start at C7 & move segmentally inferiorly to L4
• Ask patient to image the curves of their spine.
• You will work three dimensionally, that is you will focus your patient’s
83. Sagittal Plane
• First awareness of the sagittal plane by asking the patient to image anterior
(lordotic)-posterior (kyphotic) curves of the spine, then…
• Imaging or pretending that this plane of motion actually moves. They think
about movement with out actually using voluntary control of motion.
• Practitioner will usually feel some subtle change either energetically or
84. Sagittal Plane Fibromyalgia: Clinical Approaches for the Manual Therapist By Steven Goldstein Powerpoint Slide Descriptions
• Your ability to have your patient participate depends on your dialogue you
• “Imagine that your spine can move or that ou are floating horizontally or
vertically. As you float allow for the slightest of ‘wave-like’ motion to occur.
• Do not force this motion, just allow it in your mind’s eye to have gentle
85. Spinal Awareness: Frontal Plane Motion
• Next have your patient image side to side motion, that the vertebral
segments of the spine can move side to side.
• Decide whether to start at the head or the sacrum. If in doubt ask your patient
which ‘feels’ better. Or just decide by starting in one area & then reverse it by doing the other.
• I use metaphors such as imaging a snake slithering along in that plane of
86. Spinal Awareness:Rotational Plane Motion
• Finally we image that the spine can move in a spiral.
• I ask the patient which do they prefer, clockwise CW or counter-clockwise
• Then where they wish it to begin, C1 or Sacrum?
87. Positional Release Technique
• The commonality of all of these approaches is that they move the patient or
the affected tissues away from any resistance barriers and towards positions of comfort.
• The shorthand terms used for these two extremes are ‘bind’ and ‘ease’
88. PRT Variations: Lawrence Jones’ Strain Counterstrain
• ‘Positions of Ease’ were usually an ‘Exaggeration of Distortion’
• Stated simply, the tissues which were already shortened were made
comfortable by being supported in an even shorter state, so allowing neurological and circulatory mechanisms to operate and to assist in resolution of the dysfunctional state.
PRT Variations:
• Lawrence Jones’StrainCounterstrain
• Replication of the position of strain
• If, as SCS suggests, the position of ease often equals the position of strain –
then the patient needs to go back (or rather be taken back) into the direction of strain, in slow motion, until tenderness vanishes from a tender point which was being monitored, and/or until a sense of ease was perceived in the previously hypertonic shortened tissues.
89. PRT Concepts
• True SCS follows rules laid out by Jones and his tender point protocol
• No pain should be felt anywhere else in the body when using PRT
• Jones found all somatic dysfunction has palpatable areas of tenderness
• Points are often only tender when palpated or probed
Fibromyalgia: Clinical Approaches for the Manual Therapist By Steven Goldstein Powerpoint Slide Descriptions References
1. Meghan Morean Fibromyalgia: Stress & Disease, Web PPT October 29, 2002 2. Pillemer SR, Bradley LA, Crofford LJ, Moldofsky H, Chrousos GP. The neuroscience
and endocrinology of fibromyalgia. Arthritis Rheum 1997;40:1928-39.)
3. Clauw DJ & Chrousos GP. Chronic pain and fatigue syndromes: overlapping clinical
and neuroendocrine features and potential pathogenic mechanisms. Neuroimmunomodulation 1997;4:134-53.)
4. Griep EN, Boersma JW, de Kloet ER. Altered reactivity of the hypothalamic-pituitary-
adrenal axis in the primary fibromyalgia syndrome.J Rheumatol 1993 Mar;20(3):469-74
5. RM Bennett, "Understanding Chronic Pain,"
http://www.myalgia.com/off/chrpain.htm 10 February 1998).
6. Kalyan-Raman UP, Kalyan-Raman K, Yunus MB, Masi AT. Muscle pathology in
primary fibromyalgia syndrome: a light microscopic, histochemical and ultrastructural study. J Rheumatol 1984;11:808-13.)
7. Hench PK, Nonarticular Rheumatism, Twenty-Second Rheumatism Review: Review of the American and English Literature for the Years 1973 and 1974, Arthritis and Rheumatism, 1976; Supplement 19:1081-1089
8. Wilke,W.Treatment of resistant fibromyalgia. Rheumatic Disease Clinic of North America 1995 Feb 21;21(1),247–60.
9. Yunus, Muhammad B.Towards a model of pathophysiology of fibromyalgia.Aberrant
central pain mechanisms with peripheral modulation. The Journal of Rheumatology. 1992 31:2464–7.
10. Gillick, J. S., How to Tame Fibromyalgia, Paper presented April 26, 2001at the
11. Chaitow, Leon, Fibromyalgia Syndrome:A Practitioners Guide to Treatment, Churchill
12. Baldry, Peter E, Myofascial Pain and Fibromyalgia Symdromes: A Clinical Guide To
Diagnosis and Management, Churchill Livingstone, p1
13. Michael Niss PT ‘A Current Perspective: Goals & Objectives October 2004
14. Dalton, Eric, Ph.D. Fibromyalgia: Fact or Fiction, Massage & Bodywork Magazine,
15. Starlanyl, Devin, 1995-2004 Web Notes: Fibromyalgia and Chronic Myofascial Pain
16. Baldry, Peter E, Myofascial Pain and Fibromyalgia Symdromes: A Clinical Guide To
Diagnosis and Management, Churchill Livingstone, p35
17. Starlanyl, Devin, 1995-2004 Web Notes: What Your Bodyworker Should Know About
18. Staud R., Smitherman M.L. 2002. Peripheral and central sensitization in fibromyalgia:
pathogenetic role. Curr Pain Headache Rep 64:259-66.
19. Wilke,W.Treatment of resistant fibromyalgia. Rheumatic Disease Clinic of North America 1995 Feb 21;21(1),247–60.
20. Yunus, Muhammad B.Towards a model of pathophysiology of fibromyalgia.Aberrant
central pain mechanisms with peripheral modulation. The Journal of Rheumatology. 1992 31:2464–7.
21. Chaitow, Leon, Positional Release Technique, 2nd Ed Churchill-Livingstone 2002:
Extracts of the Federation Circular letter No. 31/2013 dated 04.03.2013 Sub: Our W/P 184/2011--Hearing held on 27-2-2013 We wish to advise that at the above hearing, the Hon'ble Judges asked the Asstt. Solicitor General the response of the Central Government on granting of our pension as per the prayers made in our above Writ Petition. The ASG responded that the Government is against g
Innovator duty of care in the pharmaceutical industryDoes the inventor or “innovator” of a brand-name drug have a duty of care to the consumers of that drug’s generic equivalent manufactured by a competitor? The Ontario Superior Court of Justice considered this question in the recent case of Goodridge v Pfizer Canada1 and determined that, for now, no such duty exists. In that decision, th
 Fibromyalgia: Clinical Approaches for the Manual Therapist
Fibromyalgia: Clinical Approaches for the Manual Therapist